Short peripherally placed catheters have long been the standard of care for time-limited infusion therapy and remain so today. The term short peripheral catheter denotes a product that is <3 inches long, usually about 1 inch in length; it is inserted into a peripheral vein, and the tip terminates in a peripheral vein. Still considered a peripheral catheter is the midline catheter; it is 3 to 8 inches in length and inserted in the upper arm or antecubital area. Short catheters are used for infusions, bolus drug administration, and phlebotomy for blood sampling. Midline catheters enable more concentrated solutions to be infused and may remain in place longer than does a short catheter.
In 2008, over 200 million short peripheral intravenous (PIV) catheters were used in the United States alone (Maki, 2008). Almost 70% of acute care inpatients receive a PIV at some point in their stay (Zingg & Pittet, 2009). Short PIV catheters encompass a variety of devices, including over-the-needle catheters (ONCs) with or without stabilizing features, winged infusion needles (butterfly needles), and blood collection needles.
Safety has become a priority in all health care settings. Considerations to promote safety with PIV catheters include minimizing blood exposure, clinician needlesticks, and leakage. Manufacturers tackle these issues through a variety of strategies, including closed systems and retractable needles. Needleless systems have been the standard of care for several years. Devices and safety features are addressed in Chapter 12. Techniques associated with infusion therapy remain consistent regardless of the clinical settings in which care is delivered. Adherence to institutional guidelines and Standards of Practice (INS, 2011) ensures quality outcomes.
PATIENT PREPARATION FOR PERIPHERAL VENOUS ACCESS
The nurse’s approach to the patient about to receive infusion therapy may have a direct bearing on that patient’s response to treatment. Because an undesirable response can affect the patient’s ability to accept treatment, the nurse’s manner and attitude are significant factors. Although routine for the nurse, infusion therapy may be a new and frightening experience for any patient unfamiliar with the procedure and with the health care process in general.
Patient-centered care helps the nurse to focus on the patient’s perspective of events. Being patient-centered means “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” (Institute of Medicine, 2001, p. 6). Components of patient-centered care include sharing with the patient relevant information and providing emotional support, such as relieving anxiety.
Prior experience with infusion therapy, good or bad, affects the patient’s experience of, and agreement with, treatment. If the patient has had a positive and successful venipuncture by a clinician, he or she may feel more comfortable and relaxed. If the patient’s history includes complications associated with intravenous (IV) therapy, venipuncture may be difficult. Other factors enter into the patient’s perception of infusion care, including accounts in the mass media, rumors related to errors or fatalities, or simple miscommunications. By offering a careful explanation of the procedure and keeping the patient’s privacy and comfort uppermost, the nurse can alleviate fear or anxiety and ensure patient compliance with the procedure and treatment.
Education is critical in allaying anxiety and preparing the patient for the procedure. Explain that an assessment is needed before a final decision on potential site and device can be made. Once a decision is made, in collaboration with the patient if possible, explain in lay terms what will happen and what the patient may feel and see. Education includes the necessity for infusion therapy, how long the catheter will remain in place, and signs and symptoms to report. Take time to explain the patient’s role in the process, such as opening/closing the fist or remaining still. Repeating these instructions during the procedure keeps the patient involved and may distract him or her from the possible discomfort of the needle puncture.
Knowledge of the patient’s past experiences with infusion therapy, as well as clinical condition, mental status, and other treatment modalities currently in place are important considerations in preparing the patient for venipuncture and successful infusion therapy.
Past Experience with Venipuncture and Infusion Therapy
A common reaction in health care situations is syncope. The patient may be feeling unwell, nauseous, or may have been standing and/or waiting an extended length of time. The patient may know they faint or become “light-headed” at the sight of blood. Alternatively, the patient may be experiencing emotional or physical strain. All of these situations can contribute to a vasovagal reaction, stimulated by the parasympathetic nervous system, part of the autonomic nervous system. The vasovagal reaction, which results in dilated blood vessels, slowed heart rate, and lowered blood pressure, manifests itself as syncope. It is important to assess the patient’s current status and history so that venipuncture does not contribute to further anxiety or adverse events, such as a fall and possible injury. Precipitating and aggravating factors for vasovagal syncope are found in Table 13-1.
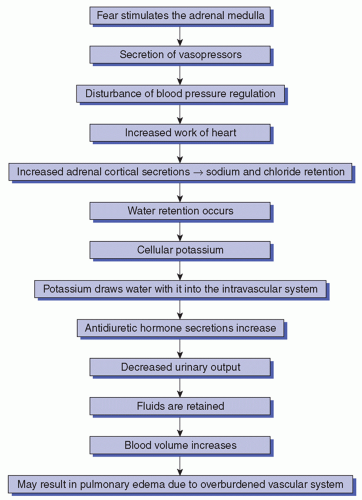
The critically ill patient is particularly susceptible to fears, triggering a fight or flight response, or an alarm reaction. This is an autonomic nervous system response, through the sympathetic nervous system, resulting in vasoconstriction, increased heart rate, increased blood pressure, and increased respiratory rate. Whether the fear is real or imagined, the patient experiences this physiologic response to a perceived threat. When there is an exaggerated reaction to fear, the fear cascade can result in decreased venous access and may constitute a real threat to the patient, particularly one with severe cardiac disease (Figure 13-1).
However, emotion and reason are difficult to separate, and researchers now believe that persons can regulate or adjust their own emotions to some extent (Kappas, 2011). In the concept of self-regulation, we do not live in an emotionally neutral state but seek out a desired state that is slightly positive. If past experiences with infusion therapy were unpleasant or painful or the patient anticipates this type of situation, it can trigger a negative feedback loop. This negative feedback loop can result in distress and anxiety for the patient, with the possible alarm reaction and attendant vasoconstriction, resulting in peripheral venous constriction and limited available veins for venipuncture. Repeated attempts at venipuncture can result in an experience so traumatic as to affect the further course of infusion therapy.
Several nursing interventions may reduce these experiences for the patient. The nurse needs to appear confident and reassuring. A skilled clinician will have a higher probability of initial venipuncture success with an anxious patient who has limited access and difficult veins. Helping the patient identify his or her commonly used coping strategies may also be effective. Or, the nurse can supplement these with other strategies such as distraction or emotional support. Establishing a relationship with the patient may assist the patient toward a more positive emotional state, as well as promote trust in the nurse’s skill.
Clinical Condition and Mental Status
A patient’s comorbidities and clinical history influence infusion therapy. A history of stroke, breast cancer, or renal dysfunction influences vein selection, as described later. If the clinician has minimal information about the patient, ask the patient if he or she has an implanted vascular device or tunneled catheter, using terms a patient would understand. A comprehensive assessment will avoid having a patient ask, “Why can’t you use the port (or Hickman) to draw blood?” This is an important assessment, particularly if the patient has a cancer or hematological diagnosis.
TABLE 13-1 PRECIPITATING AND AGGRAVATING FACTORS FOR VASOVAGAL SYNCOPE
Precipitated by
Aggravated by
Sudden emotional stress (adaptogenicity)
Pain or fear of anticipated harm
Sudden relief of anxiety
Vascular cannulation
Arterial decannulation
Fasting
Dehydration
Challenged physical condition
Room temperature
Fatigue
FIGURE 13-1 The fear cascade.
The ambulatory surgical patient has decidedly different needs than does the critically ill patient with multiple IV accesses. If the patient will be involved in self-care and selfadministration of IV medications and solutions, the approach must encourage and support the patient’s independence and confidence. Plans for promoting self-care and independence should begin at the time of admission to the hospital, treatment at the clinic, or with the patient’s first encounter with infusion therapy.
Mental status influences the clinician’s assessment. Is the patient able to provide an accurate history? Will mental status influence the patient’s ability to comprehend instructions or follow directions? If a patient is confused, there may be a risk of inadvertent catheter removal. Last, is the patient able to give consent or assent to the procedure? Involving the family and/or caregiver may be key to the collection of this information.
Other Treatment Modalities
Use of multiple clinical modalities (i.e., nutritional support, antibiotics, or transfusions) has a significant effect on preparation for infusion therapy. In such cases, the clinician may consider using a multilumen catheter so that administration of subsequent medications can be timed to avoid interference with the line providing nutrition or the line providing transfusion therapy. Other concerns include non-IV therapies. For example, if the patient is also undergoing physical or occupational therapy, the nurse may find it difficult to use the dorsal aspect of the hand for an IV because such placement makes maintaining secure, dry connections and a tightly sealed dressing difficult.
CONSIDERATIONS FOR SHORT PERIPHERAL CATHETER INFUSION
There are several considerations in selecting peripheral venous access using a short catheter. Among these are patient preferences and values. Foremost is the patient’s consent for treatment. Engaging the patient in the discussion, such as which type of device or which arm is more suitable for venipuncture, may promote a positive attitude and adherence to the plan. Other considerations are described below and outlined in Box 13-1.
Type of Therapy
Infusion therapy may involve isotonic solutions for hydration, solutions with high viscosity or high osmolarity, or vesicant or irritant medications, thus influencing the site for infusion and type of device selected. Additionally, the desired infusion rate needs to be considered. Larger veins have more blood flow volume, which provides rapid disbursement of fluid and rapid dilution. Thus, larger veins are recommended for infusions of
Large quantities of solution with rapid administration
Solutions using positive pressure
Fluids with high viscosity, such as packed red blood cells (RBCs)
Irritant or vesicant medications
A new peripheral venous access site is needed when vesicant medications are administered through a short catheter (INS, 2011, p. S88). Continuous infusions of vesicant medications should be administered only through a central vascular access device (CVAD), not a short peripheral catheter (INS, 2011, p. S88).
BOX 13-1 CONSIDERATIONS FOR SHORT CATHETER PIV INFUSION
Patient preferences and values
Type of therapy
Duration of therapy
Catheter gauge
Vascular assessment
Parenteral nutrition administration is recommended through a CVAD. However, until a CVAD is placed, a short peripheral catheter or midline may be used for specific parenteral nutrition solutions. Only those solutions with a final concentration of 10% dextrose or lower, or with osmolarity not exceeding 600 mOsm, may be administered in this manner (INS, 2011, pp. S91-S92). However, peripheral administration of parenteral nutrition causes phlebitis; several strategies can minimize the inflammation and prolong the infusion until a CVAD is placed (INS, 2011, p. S92). More frequent site rotation can reduce the incidence of phlebitis; regular assessment and monitoring by the nurse will promote the most advantageous rotation for safety while reducing painful venipunctures for the patient.
If the solution’s pH is <5 or >9, it must be administered through a CVAD (INS, 2011, S37). A final consideration is whether the medication is at risk for diversion. This would influence the type of device and the method of administration. All actions to prevent or reduce the risk of this scenario are necessary.
Duration of Therapy
A prolonged course of therapy requires multiple infusions and possibly multiple venipunctures, which makes preservation of the veins essential. Performing the venipuncture distally with each subsequent puncture proximal to the previous one and alternating arms contributes to venous preservation. Short peripheral catheters are usually indicated for infusion therapy of <1 week, and winged steel needles should be limited to single-dose administration or short-term therapy (INS, 2011, p. S37). Whether using and replacing a short peripheral catheter for 1 to several weeks or considering a midline, a peripherally inserted central catheter (PICC), or other CVAD, the health care team and patient need to discuss the options when infusion therapy is anticipated to be lengthy.
Patient comfort always needs to be considered, but especially when infusions are required over an extended period. For instance, performing venipunctures on veins located on the dorsal surface of the extremities provide more freedom and comfort for the patient.
Catheter Gauge
Selection of the gauge of the PIV catheter to be inserted is a nursing decision. The standard is to use the smallest gauge needed to accommodate the prescribed therapy (INS, 2011, p. S37). Short peripheral catheters come in sizes from 14- to 27-gauge. Small-gauge catheters are able to infuse solutions quite rapidly, almost 1 L/h for some sizes; for example, one 24-gauge peripheral catheter has the capacity to infuse 960 mL/h (BD Medical, 2013). Special populations, such as the elderly, neonates, and infants often require extremely small-gauge catheters. Otherwise, it is the type of therapy or procedure that drives the catheter gauge. If the catheter is to be used for a power injection, special catheters identified for this purpose are required to withstand the administration pressure. Patients having a surgical procedure may need a larger device, such as an 18 gauge; the gauge may be specified in preoperative orders. Transfusion of blood and blood products can generally be accommodated with short peripheral catheter gauges as small as 22 to 24 (INS, 2011, p. S37).
Vascular Assessment
The nurse responsible for venipuncture or team may make the vascular assessment. If findings confirm that limited vascular access precludes successful peripheral venipuncture or the treatment is long-term, consideration should be given to the use of alternative access devices, such as a midline, PICC, or other CVAD. If, after assessment of therapy type and duration, a PIV catheter is indicated, the nurse proceeds with vein selection and then the procedure for a PIV catheter insertion and infusion or locked catheter.
VEIN SELECTION
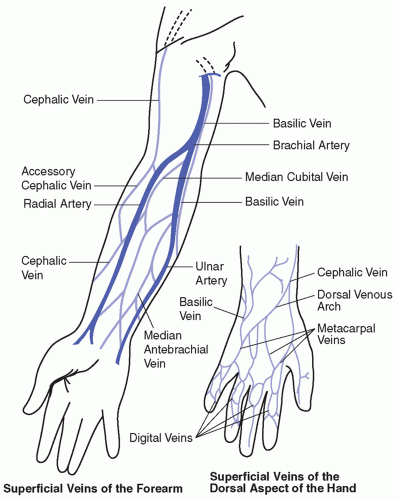
The selection of the vein may be a deciding factor in the success of the infusion and the preservation of veins for subsequent treatment (Table 13-2). The most prominent vein is not necessarily the most suitable for venipuncture. Prominence may result from a sclerosed condition, which occludes the lumen and interferes with the flow of solution, or the prominent vein may be located in an area impractical for infusion purposes. Scrutiny of the veins in both arms is desirable before a choice is made. Using the nondominant side is recommended to avoid restricting patient function. However, asking the patient which side is preferred or identifying benefits of using one side versus the other may elicit more cooperation from adult patients. Factors to be considered in selecting a vein include location and condition of the vein.
TABLE 13-2 SITE SELECTION: SUPERFICIAL VEINS OF THE ARM
Vein
Location
Device
Considerations
Cephalic
Radial aspect of lower arm along radial bone of the forearm
18- to 22-gauge cannula; usually ONC
Large vein, easily accessed
Start distal and work upward Good for infusing blood or chemically irritating drugs
Basilic
Ulnar aspect of lower arm along the ulnar bone
18- to 22-gauge ONC
Difficult to access
Large vein, easily palpated
Stabilize during venipuncture
Accessory cephalic
Branches off cephalic vein along radial bone
18- to 22-gauge ONC
Medium-large vein, easily stabilized
Valves at cephalic junction may inhibit catheterization
Short length may require short (1-inch) catheter
Upper cephalic
Radial aspect of upper arm above elbow
16- to 20-gauge ONC
Difficult to visualize
Good site for confused patients
Median antebrachial
Extends up front of forearm from median antecubital
18- to 22-gauge ONC
Nerve endings preclude cannulation Infiltration may occur
Median basilic
Ulnar aspect of forearm
18- to 22-gauge ONC
Appropriate site
Median cubital
Radial aspect of forearm
18- to 22-gauge ONC
Appropriate site
Veins in area of antecubital fossa
Bend of elbow
Any size; may be used for midline or PICC insertion
Best for emergency interventions
ONC, over-the-needle catheter.
Location
Most superficial veins are accessible for venipuncture (Figure 13-2), but some of these veins, because of their location, are not practical. For example, the antecubital veins are a poor choice for routine therapy because they are located over an area of joint flexion where any motion could dislodge the IV catheter and cause infiltration or result in mechanical phlebitis. If these large veins are impaired or damaged, phlebothrombosis may occur, which can limit access to the many available hand veins. The antecubital veins offer excellent sources for withdrawing blood and may be used many times without damage to the vein, provided good technique is used. However, one infusion of long duration may traumatize the vein, limiting the availability of vessels that most readily provide ample quantities of blood when needed.
Because of the proximity of the arteries to the veins in the antecubital fossa, special care must be taken to prevent intra-arterial injection when medications are introduced. Aberrant arteries in the antecubital area are present in 1 of 10 people. When a patient complains of severe pain in the hand or arm on infusion, an arteriospasm caused by an intra-arterial injection is to be suspected, and the infusion must be stopped immediately.
FIGURE 13-2 IV placement chart. (Courtesy of Becton Dickinson Vascular Access.)
The ventral surface of the wrist should be avoided due to the pain on insertion and risk of damage to the radial nerve (INS, 2011, p. S41). Other potential venous sites to avoid would be areas of pain on palpation; compromised veins such as those that are bruised, infiltrated, inflamed, corded, or sclerosed; or areas of planned procedures (INS, 2011, p. S41).
Several factors influence which arm should be avoided, if possible. These include an upper extremity on the side with an axillary node dissection, radiation therapy, or lymphedema; these are conditions where circulation may be impaired, affecting the flow of the infusion and possibly increasing or causing edema. If a stroke has affected the functioning of an upper extremity, that side should be avoided. However, choices for venous access may be limited. In this case, a “collaborative discussion” between the patient and the physician/licensed independent practitioner (LIP) and/or team is needed to review the risks and benefits of using a vein in the affected extremity (INS, 2011, p. S41).
For patients with renal dysfunction, several factors are identified. Avoid the use of an extremity with an arteriovenous fistula or graft inserted for dialysis. Additionally, for patients with chronic kidney disease stage 4 or 5, “avoid forearm and upper arm veins ‘suitable for placement of vascular access’” (INS, 2011, p. S41). This protects vascular access for future use in the case of kidney failure and the need for hemodialysis or renal replacement therapy.
Surgery often dictates which extremity can be used and is often identified in the preoperative orders. When the patient is turned to the side-lying position during an operation, the upper arm is used for the infusion; increased venous pressure in the lower arm may interfere with free flow of the solution.
The use of veins in the lower extremities of adults is discouraged because of the risk of thrombophlebitis, tissue damage, and ulceration (CDC, 2011; INS, 2011, p. S41). There is also the danger of pulmonary embolism caused by a thrombus extending into the deep veins. Complications may arise from the stagnant blood in varicosities, which makes them susceptible to trauma. If a catheter is inserted into a lower extremity vein, replace the catheter into an upper extremity as soon as possible (CDC, 2011).
Condition of the Vein
Frequently, the dorsal metacarpal veins provide points of entry that may be used first to preserve the proximal veins for further therapy. The use of these veins depends on their condition. In some elderly patients, the dorsal metacarpal veins may be a poor choice; blood extravasation occurs more readily in small, thin veins, and it may be difficult to secure the catheter adequately because of thin skin and lack of supportive tissue. At times, these veins do not dilate sufficiently to allow for successful venipuncture; when hypovolemia occurs, the peripheral veins collapse more quickly than do larger, more proximal ones.
Palpation of the vein is an important step in determining the condition of the vein and in differentiating it from a pulsating artery. A thrombosed vein may be detected by its lack of resilience; its hard, cordlike feeling; and by the ease with which it rolls. Use of such traumatized veins results in repeated attempts at venipuncture, pain, and undue stress. Often, large veins may be detected by palpation and offer advantages over the smaller but more readily discernible veins. Because of the small blood volume, the more superficial veins may not be easily palpated and may not make a satisfactory choice for venipuncture.
Continual use by the nurse of the same fingers for palpation increases their sensitivity. The thumb should never be used because it is not as sensitive as the fingers; also, a pulse may be detected in the nurse’s thumb, and this may be confused with an aberrant artery.
Although not apparent, edema may conceal an available vein; application of finger pressure for a few seconds may help to disperse the fluid and define the vein.
Large veins are used when hypertonic solutions or solutions containing irritating drugs are to be infused. Large vessels provide better hemodilution of the drug or solution, thereby minimizing the potential for developing phlebitis. Such solutions traumatize small veins; the supply of blood in these veins is not sufficient to dilute the infused fluid.
INITIATING PERIPHERAL VENOUS ACESS WITH SHORT CATHETERS
Hand hygiene cannot be overemphasized. It “should be performed before and after palpating catheter insertion sites as well as before and after inserting, replacing, accessing, repairing, or dressing an intravascular catheter. Palpation of the insertion site should not be performed after the application of antiseptic, unless aseptic technique is maintained” (CDC, 2011, p. S3).
Environment
For patient privacy, close the door or the bedside curtains if the patient has a roommate. Ask the patient if they wish visitors to leave the room during the procedure. Clean an area on which to place the equipment and support the patient’s arm. The patient should be in a comfortable position with the arm on a flat surface. If the patient is uncooperative or disoriented, determine the best method and/or strategy to prevent the patient from moving the arm during catheter insertion. A restraint may escalate the situation. Solicit the assistance of a family member or another caregiver to soothe or distract the patient and/or secure the arm. Last, the type of intervention is dependent on the urgency of the vascular access.
Proper lighting is very important and should not be overlooked. A few extra seconds spent in obtaining adequate light may actually save time and free the patient from unnecessary venipunctures. The ideal light is either ample daylight or a spotlight that does not shine directly on the vein but leaves enough shadow for clearly defining the vessel.
Solution, Administration Set, IV Pole, and Venipuncture Equipment
Venipuncture and initiation of an IV infusion or locked PIV are carried out upon the order of a physician/LIP. The solution, volume, any additives, rate, duration, and route (e.g., PIV, “Start IV”) are specified in the order. Verify with the order that the solution obtained is that which is ordered.
Obtain all equipment and solution. A PIV kit is recommended to ensure that all supplies are easily available and to reduce time away from the patient by the nurse (Figure 13-3). Careful inspection is necessary to ensure that the fluid is clear and free of particulates and the container intact—with no cracks in the glass bottle or holes in the plastic bag. The label must be checked to verify that the correct solution is being used and that the container is not outdated. The nurse also needs to check the time and the date the container was opened. After 24 hours, the fluid is outdated and should not be used; expiration dates are specified in institutional policy.
FIGURE 13-3 Peripheral intravenous catheter kit.
Open the IV administration set, close the roller clamp, remove the cap to the tubing insertion spike, and insert the spike into the container with a thrust, not a twisting motion. Hang the solution container on the pole. Squeeze the drip chamber so that it fills almost half full. Prime the tubing by slowly opening the roller clamp to fill the tubing fully. Close roller clamp. If extension tubing is needed, use sterile technique to attach it, and prime it as well. The fluid container is suspended approximately 3 feet above the injection site. The pressure from this height is adequate to ensure a maximum flow rate. The greater the height of the container, the greater the force with which the fluid flows into the vein should the flow-control clamp release. Many institutions have policies on which infusions require electronic control devices or pumps. Verify whether the ordered infusion requires a pump. Follow manufacturer’s directions for priming the pump with device-specific tubing. Ensure that there is no air or air bubbles in the tubing; firm tapping will remove any air bubbles. Although air embolism is rare, air bubbles concern the nurse and alarm the patient (Cook, 2013; Wilkins & Unverdorben, 2012).
PATIENT SAFETY
To prevent air embolism, expel all air from IV tubing or pump cartridges before connecting to the patient’s catheter. “Do not leave tubing attached to fluid but unprimed at the bedside if it is intended to be connected” (p. 32).
Cook, L. S. (2013). Infusion-related air embolism. Journal of Infusion Nursing, 36, 26-36.
Many units or areas have an infusion tray with all necessary equipment and supplies to start a PIV. There may also be prepackaged sets with the PIV catheter, cleansing solution, and dressing. The patient’s blood pressure cuff may be used to distend the vein or a singlepatient use tourniquet may be applied (INS, 2011). For infection control purposes, tourniquets are not carried from patient to patient.
Vascular Access Site Preparation
If the area selected for venipuncture is hairy, clipping the hair permits better cleansing of the skin and makes removal of the catheter less painful when the infusion is terminated. Shaving is not recommended (INS, 2011, p. S44). If the area is visibly soiled, soap and water cleansing is necessary.
The designated venous site should be scrubbed with an antiseptic that remains in contact with the skin for at least 30 seconds before venipuncture. An appropriate single-dose antiseptic agent should be used. Site preparation with chlorhexidine solution is preferred for antisepsis (INS, 2011); other solutions that may be used include 70% alcohol, 2% tincture of iodine, or 10% povidone-iodine (CDC, 2011). It is important to note that a 2% chlorhexidine in 70% ethanol solution was used for site preparation in a study where the peripheral catheter was replaced only when signs and symptoms of phlebitis occurred (Rickard et al., 2012). Avoid aqueous benzalkonium-like compounds or hexachlorophene.
PATIENT SAFETY
Allow antiseptic agent to air dry. If using povidone-iodine as the primary antiseptic agent, do not apply alcohol, as it will negate povidone-iodine’s antimicrobial effect. If using alcohol as a single agent, apply for a minimum of 30 seconds. If using tincture of iodine, allow it to dry, then remove with alcohol, and allow it to dry.
Local Anesthetic Considerations
It is important for the nurse to consider local anesthesia based on the patient’s past experiences or current state. It is advised for all painful IV procedures in children and some adults (INS, 2011, p. S43). Using the least invasive method of local anesthesia will reduce the risk of infection.
A topical transdermal medication, such as EMLATM (eutectic mixture of local anesthetics), is noninvasive. It is a cream mixture of two local anesthetics (lidocaine 2.5% and prilocaine 2.5%) and applied under an occlusive dressing for a specified time, from 30, 60, to 120 minutes (Table 13-3). The release of lidocaine and prilocaine into the epidermal and dermal layers of the skin provides anesthesia. The two agents stabilize neuronal membranes by inhibiting the conduction of impulses (Astra Zeneca). Use of this product is contraindicated in patients with a known history of sensitivity to local anesthetics of the amide type.
Only gold members can continue reading. Log In or Register to continue
 PATIENT SAFETY
PATIENT SAFETY PATIENT SAFETY
PATIENT SAFETY








