Pelvic Masses
Paula J. Adams Hillard
KEY WORDS
Adnexal torsion
Corpus luteum cyst
Dermoid cyst
Follicular cyst
Functional cyst
Imperforate hymen
Ovarian cyst
Paratubal cyst
A pelvic mass may be identified during a routine screening examination, or it can be discovered during an evaluation for abdominopelvic pain or abnormal bleeding. It may also be an incidental finding at the time of imaging for an unrelated medical concern. The list of likely diagnoses of a pelvic mass for prepubertal, adolescent and young adult (AYA) females is different than that for older women, although there may be some overlap.1 Table 52.1 lists a number of conditions that may be diagnosed as a pelvic mass in women of reproductive age.
Uterine Defects: Incomplete Fusion
Anatomical genital anomalies, which typically present as a pelvic mass during adolescence, are rare, but they can have profound implications for future reproductive capability.2 It is uncommon, but not unheard of for nonobstructing anomalies to present in young adulthood. Embryologically, the uterus is formed by fusion of paramesonephric ducts in the midline (Fig. 52.1). If lateral fusion is incomplete, then a uterine didelphys may form with two separate uterine halves (each with its own cervix, corpus, attached fallopian tube and ovary, and possibly vaginal canal) (Fig. 52.2). On examination, one of the two uteri may be mistaken for an adnexal mass. If uterine fusion is partial, there may be a bicornuate uterus or blind uterine horn. There may be a unilateral obstructed horn, and if functional endometrium is present within this obstructed horn, severe cyclic pain can occur. The diagnosis can be suggested on the basis of a screening pelvic ultrasound examination. If a developmental anomaly is suspected on ultrasound examination, magnetic resonance imaging (MRI) is the best technique for clarifying genital anomalies.3 Renal and skeletal anomalies are common in conjunction with uterine lateral fusion defects.4
TABLE 52.1 Conditions Diagnosed as a Pelvic Mass in Women of Reproductive Age | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
The vagina also forms in two parts, and defects typically occur as a result of failure of longitudinal fusion or canalization. If the upper and lower vaginal portions do not fuse, then a transverse vaginal septum forms. Similarly, if the solid core of tissue at the junction of the vaginal plate and the urogenital sinus not canalize completely, the woman can have an imperforate hymen or vaginal agenesis. If a uterus with functional endometrium is present along with a transverse vaginal septum or imperforate hymen, menstrual fluid accumulates within the patent portion of the vagina (hematocolpos) and within the uterus (hematometra), which then presents as a “pelvic mass” (Fig. 52.3). Imperforate hymen is the most frequent obstructive anomaly of the female genital tract, but estimates of its frequency vary from 1 case per 1,000 population to 1 case per 10,000 population.5
Uterovaginal Agenesis
Women with uterovaginal agenesis—Mayer-Rokitansky-Küster-Hauser syndrome—may have uterine remnants that may or may not contain functioning endometrium, which can cause pain, and a mass that is diagnosed with ultrasonography or MRI.
Müllerian Duct Remnants
Another class of anatomical congenital anomalies that can create pelvic masses arises from remnants of the mesonephric/müllerian duct system or mesovarium that should have degenerated in utero in the presence of antimüllerian hormone. At least 25% of adult women have small remnants of these systems. These remnants can be present in the lateral adnexa as paraovarian cysts or paratubal cysts (Fig. 52.4). They are often multiple and can vary in size from <1 cm to 20 cm. Along the lateral wall of the vagina or uterus, these remnants present as Gartner duct cysts. These müllerian
remnants are rarely symptomatic; however, torsion of an adnexal mass can occur, and persistent larger masses may be confused with an ovarian neoplasm.
remnants are rarely symptomatic; however, torsion of an adnexal mass can occur, and persistent larger masses may be confused with an ovarian neoplasm.
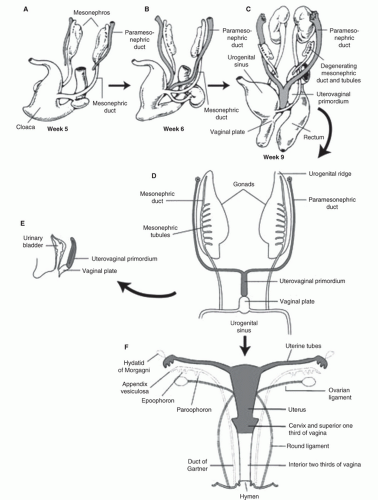 FIGURE 52.1 Development of uterus from paired paramesonephric ducts. (From Dudek RW. BRS embryology. 5th ed. Philadelphia, PA; Lippincott Williams & Wilkins, 2010.) |
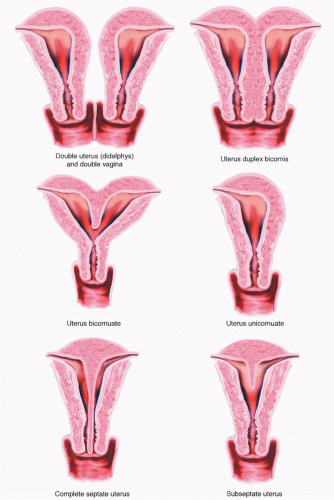 FIGURE 52.2 Uterine fusion abnormalities. (From Baggish MS, Valle RF, Guedj H. Hysteroscopy: visual perspectives of uterine anatomy, physiology and pathology. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2007.) |
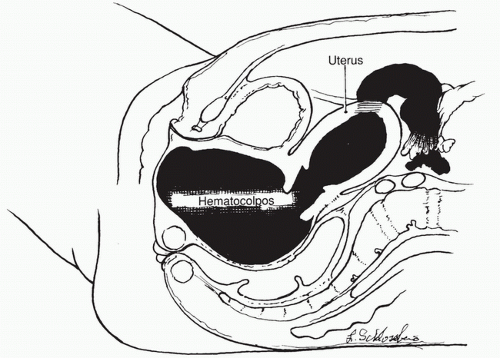 FIGURE 52.3 Hematocolpos, hematometra, hematosalpinx due to imperforate hymen. (From Rock JA, Jones HW. Te Linde’s operative gynecology. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008.) |
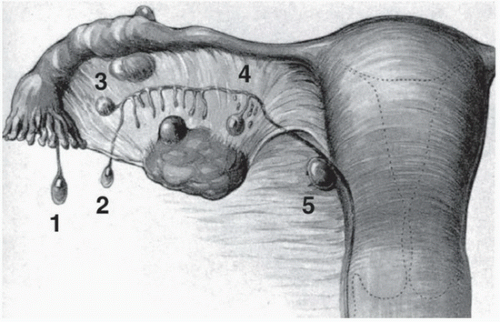 FIGURE 52.4 Paratubal cysts from embryologic remnants. (From Dudek RW. BRS embryology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.) |
Urachal Cysts and Pelvic Kidneys
Urachal cysts, although rare, can be found along the midline above the bladder and can be confused with other pelvic masses. A pelvic kidney must also be included in the differential diagnosis (Fig. 52.5). Any other structure in the pelvis, such as a full bladder or hard stool in the bowel, can be confused with a pelvic mass.
The possibility of an intrauterine pregnancy enlarging the uterus or an ectopic pregnancy (see Chapter 53) causing an abdominal or adnexal mass must be considered in the differential diagnosis of every young woman with secondary sexual characteristics (Fig. 52.6). A sensitive urine pregnancy test can reliably rule out a clinically significant pregnancy. However, in many instances, the test is not ordered because the provider does not consider it likely that the adolescent or young adult has been sexually active. Adolescents may be unwilling or unable to disclose their history of sexual activity for a variety of reasons—they may fear disappointing their parents or the clinician; they may have insufficient knowledge or awareness of pregnancy-related symptoms; they may deny the possibility of pregnancy; the clinician may not have established or discussed provisions of confidentiality; or the question may not have been asked in a sensitive manner in a private setting. Both sexual abuse and early consensual sexual activity may occur, resulting in pregnancy. If pregnancy testing is a routine order, then its use in any individual case does not require justification. The consequences of missing a pregnancy-related cause of pain, bleeding, or asymptomatic pelvic mass justify routine pregnancy testing in all young women presenting with pain, amenorrhea, abnormal bleeding, or a pelvic mass.6
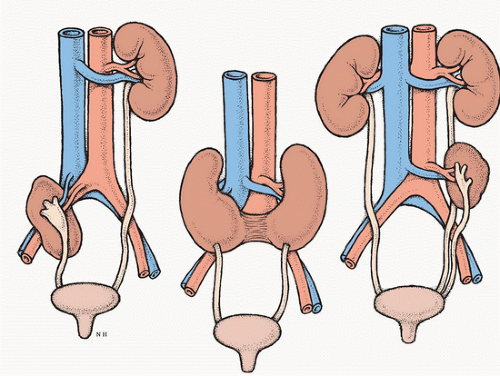 FIGURE 52.5 Pelvic kidney, horseshoe kidney, and supernumerary kidney. (Courtesy of Neil O. Hardy, Westpoint, CT.) |
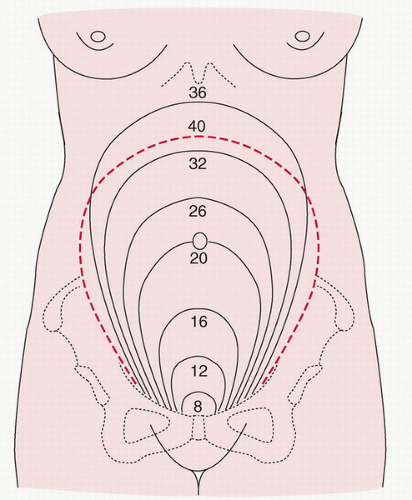 FIGURE 52.6 Pregnancy with fundal height corresponding to gestational age. (From Beckmann CRB, Ling FW, Smith RP et al. Obstetrics and gynecology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
AYAs have the highest age-specific rates of chlamydia, and thus are at risk for upper track involvement with salpingitis or pelvic abscess (tuboovarian abscess [TOA]) (see Chapter 58)7. In the acute stage, pelvic infection may be indolent in its presentation or, alternatively, accompanied by fever, discharge, cervical motion tenderness, and possibly adnexal masses (pyosalpinges or TOAs) (Fig. 52.7). After resolution of the acute infection, the tubes may remain dilated and filled with fluid (hydrosalpinges), particularly if their fimbriae have been sealed. Treated pelvic abscesses may also cause palpable masses due to adhesions-pelvic scarring with matting or agglutination of bowel, ovary, fallopian tube, and other structures. Other infectious causes of pelvic masses include an appendiceal abscess or (rarely in young girls) diverticulitis or Meckel diverticulum.
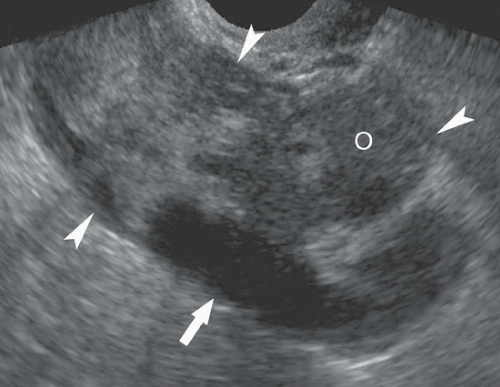 FIGURE 52.7 Tuboovarian abscess. Ultrasound of the pelvis shows complex mass (arrowheads) around the ovary (O) and dilated tube (arrow). (From Brant WE; Helms CA. Brant and Helms solution. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
Adnexal torsion involves the acute rotation of adnexal structures, and is a cause of acute pelvic pain, which may be accompanied by nausea and vomiting. The diagnosis may be missed if the possibility of torsion is not considered.8 Torsion of the normal adnexa can occur; however, torsion is more likely to occur when an adnexal mass rotates around its vascular pedicle. Once rotated, the venous flow to the mass is obstructed while arterial flow continues, inflating the mass until arterial flow is compressed (Fig. 52.8). The adnexal structures become edematous and ultimately gangrenous.
Diagnosis
Findings on examination include peritoneal signs with rebound tenderness. Typical findings on ultrasound examination with Doppler flow studies include the presence of a mass, edema, adnexal asymmetry, and absent venous and/or arterial flow; unfortunately, these findings are neither perfectly sensitive nor specific, and clinical judgment must be used, including a high index of suspicion.8 Consultation with a gynecologist is essential, as adnexal torsion is a surgical emergency.
Treatment
Treatment consists of untwisting the adnexa, even if hemorrhage and apparent necrosis are present, as ovarian preservation is almost always possible. This can usually be performed laparoscopically. Excision of the cyst can be performed laparoscopically, or may be delayed and performed as an interval procedure once edema has resolved. Every attempt should be made to preserve the involved ovary.
In AYA women, uterine neoplasms are quite rare. Benign leiomyomas (fibroids) may cause abnormal bleeding, and will be evident on pelvic imaging.
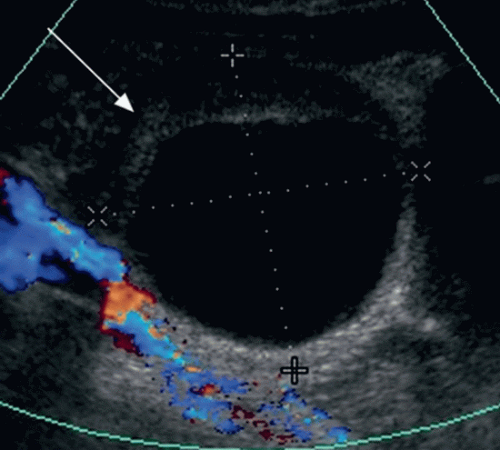 FIGURE 52.8 Ovarian torsion. Ultrasound with ovarian cyst with no Doppler flow. (From Shirkhoda A. Variants and pitfalls in body imaging. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.) |
Benign ovarian masses include functional ovarian cysts, endometriomas, and benign ovarian neoplasms. Whenever an ovarian mass is diagnosed in an adolescent female or prepubertal child, every effort must be made to preserve the reproductive function, whether the mass is physiologic or neoplastic, benign, or malignant.9 Table 52.2 lists benign ovarian tumors. Figure 52.9 provides a plan for management of pelvic masses in premenarchal and adolescent girls.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


