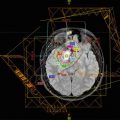
Fig. 22.1
(a) Contrast-enhanced CT scan with solitary ring-enhancing lesion (white arrow), (b) contrast-enhanced T1-weigted MRI with solitary ring-enhancing lesion with hypointense necrotic core (white arrow), (c) T2-weighted MRI and (d) FLAIR images demonstrating hyperintensity extending beyond the lesion reflecting vasogenic edema (black arrow)
22.5.1 Ewing Sarcoma
Ewing sarcoma is the second most common bone tumor in pediatric patients, resulting in 200–250 cases a year in the United States. Primary sites of involvement include the pelvis, femur, and ribs. Due to advances in surgery, chemotherapy, and radiation therapy, survival approaches 70–80% for localized disease (Goldman et al. 2007). Though the main sites of metastases are the lungs, bone, and bone marrow, Ewing sarcoma is one of the most common types of pediatric cancers to develop BM, with 3–16% of patients progressing to CNS metastases. Sixty to 100% of cases reported in the literature were found to have simultaneous lung lesions (Bouffet et al. 1997; Stefanowicz et al. 2011; Kebudi et al. 2005; Paulino et al. 2003; Parasuraman et al. 1999). Parasuram et al. who included both parenchymal and direct extension estimated that close to half of the metastases are hematogenous in origin while the other half are via direct extension (Parasuraman et al. 1999). In their analysis, Bouffett et al. only included patients with parenchymal metastases and excluded patients with disease arising from direct extension; estimating the rate of parenchymal disease from hematogenous spread as approximately 5.4% (Bouffet et al. 1997).
The management of BM arising from Ewing sarcoma has generally included consideration of surgical resection in the setting of symptomatic or solitary lesions as well as whole brain radiation therapy (WBRT) and chemotherapy. Paulino et al. reported six cases of Ewing sarcoma patients with BM. While BM was identified at autopsy in one case, the balance were treated with either chemotherapy alone, surgery followed by radiation, or a combination of radiation and chemotherapy. Two patients died of their metastatic CNS disease, and the remaining three died from systemic disease. The median survival after the diagnosis of BM was 1.5 months (Range: 1–9 months) (Paulino et al. 2003). Weins et al. reported three Ewing sarcoma patients in their series with BM were treated with a combination of surgery and radiation with a median survival of 4 months from the diagnosis of CNS spread (Wiens and Hattab 2014). While most patients were treated with WBRT in published series, there are isolated case reports utilizing stereotactic radiation in the setting of adjuvant treatment (van Dams et al. 2016). Nonetheless, the outcomes have been poor with most patients dying within 1 year of the development of BM though there are some reports of long-term survivors (Paulino et al. 2003; Parasuraman et al. 1999; van Dams et al. 2016).
22.5.2 Rhabdomyosarcoma
Rhabdomyosarcomas are the most common pediatric soft tissue sarcomas with approximately 250 cases a year in the United States, comprising approximately 10% of childhood solid tumors. Up to 20% of patients will eventually progress to metastases, most frequently in the lungs, lymph nodes, and bone marrow (Goldman et al. 2007). The incidence of BM in the literature has ranged from 2 to 10%. In a study of 104 patients with rhabdomyosarcoma, 6.7% of patients developed BM, with all seven patients having prior or synchronous distant metastatic disease (Paulino et al. 2003). BM develops at a median of 12 months after initial diagnosis via hematogenous spread or through direct extension (Paulino et al. 2003; Parasuraman et al. 1999).
Risk factors include parameningeal disease and distant disease at extracranial sites. Parameningeal rhabdomyosarcoma with cranial nerve palsies, intracranial tumor extension, and skull base erosion are at a particularly increased risk of metastatic spread to the brain. The treatment approach of BM has similarly included possible surgical resection of solitary and symptomatic lesions as well as radiotherapy and chemotherapy, with parenchymal BM carrying a poor overall prognosis with most patients dying within 1 year (Kebudi et al. 2005; Paulino et al. 2003; Parasuraman et al. 1999). Chemotherapy has typically consisted of multiple agents, at times including intrathecal methotrexate. Reported radiation doses and fields have not been standardized but have in general consisted of WBRT with doses ranging from 30 Gy in 20 fractions to 50 Gy in 25 fractions (Stefanowicz et al. 2011; Paulino et al. 2003). A recent case series reported the outcomes of two rhabdomyosarcoma patients with infratentorial metastases. Both patients were treated with aggressive trimodality treatment. One patient aged 1 year and 11 months underwent a gross total resection followed by 23.4 Gy to the tumor cavity and ifosfamide/carboplatin/etoposide (ICE) chemotherapy and remains alive without disease at 8 months. The second patient developed metastatic disease involving the pons and cerebellum 16 months after initial diagnosis and was treated with subtotal resection, craniospinal irradiation (CSI) to 30.6 Gy followed by an additional 14.4 Gy boost, ICE chemotherapy, and allogenic stem cell transplant. He remains alive without disease at 10 months (Osawa et al. 2011).
22.5.3 Osteosarcoma
Osteosarcoma is the most common pediatric primary bone tumor, typically arising from the femur, proximal tibia, or pelvis. Although the lungs are the most common site of distant metastases, approximately 1.8–16% of pediatric osteosarcoma patients will develop CNS metastases, making it one of the most common primary solid tumors to develop BM (Graus et al. 1983; Wiens and Hattab 2014; Suki et al. 2014; Paulino et al. 2003; Marina et al. 1993). In some series, the incidence of BM has increased in the setting of modern chemotherapy, from 4.5% before 1982 to 15.5% from 1982 onward (Marina et al. 1993). Patients develop CNS lesions at a median of 22–24 months from initial diagnosis (Graus et al. 1983; Paulino et al. 2003). Although metastatic disease can arise from extracranial extension from lesions in the calvarium, the primary method of spread is thought to be most frequently hematogenous. In a retrospective study of 254 patients treated at St. Jude Children’s Hospital, 13 patients developed parenchymal metastatic disease compared to 3 with spread from adjacent sites (Marina et al. 1993). Moreover, most osteosarcoma patients with BM have extracranial metastatic disease, with 70–100% patients presenting with prior or simultaneous pulmonary metastases (Wiens and Hattab 2014; Paulino et al. 2003; Marina et al. 1993). Nevertheless, there are rare reports of patients presenting with a parenchymal BM as their first site of relapse (Niazi et al. 2009).
Similar to the management strategies employed in other sarcomas, such as rhabdomyosarcoma and Ewing sarcoma, the treatment of BM in osteosarcoma involves surgical resection for solitary or symptomatic lesions as well as radiation therapy and possibly further chemotherapy. The prognosis after the diagnosis of BM is typically bleak, with most patients succumbing within 6 months, although there are some exceptional reported cases of long-term survivors after 5 years treated with multimodal therapies (Wiens and Hattab 2014; Marina et al. 1993; Wexler et al. 1993).
22.5.4 Neuroblastoma
Neuroblastoma comprises 8–10% of all childhood cancers, making it the most common extracranial solid tumor in children. The treatment approach is multimodal and may include chemotherapy, surgery, radiation therapy, high-dose chemotherapy with stem cell rescue, and immunotherapy. Although infants less than 1 year old tend to have very favorable outcomes despite the presence of metastatic disease, older children may present with extensive metastatic disease at the time of diagnosis with a very poor prognosis. Metastases typically develop by means of lymphatic and hematogenous spread, most commonly to bone marrow, bone, liver, skin, and uncommonly lungs (Goldman et al. 2007). BM are a rather rare occurrence in neuroblastoma although they have been reported in a number of series with increasing incidence over time. In fact, the incidence of BM in newly diagnosed neuroblastoma has been reported to have increased from 1.7% in the early 1980s to 11.7% in the 1990s, likely due to more effective systemic therapies (Kramer et al. 2001). Contemporary series estimate the incidence of BM between 1 and 10.4% (Suki et al. 2014; Paulino et al. 2003; Matthay et al. 2003; Zhu et al. 2015). Patients typically present in conjunction with extracranial disease or as isolated metastases, and disease may involve both the parenchyma and the leptomeninges, with the former being more common in infants older than 1 year of age and the later more common in infants less than 1 year old (Matthay et al. 2003; DuBois et al. 1999). As metaiodobenzylguanidine (MIBG) imaging has been reported to have a low sensitivity for smaller brain metastases, MRI imaging remains the favored imaging modality when BM are suspected (Nabavizadeh et al. 2014; Matthay et al. 2003).
Management of neuroblastoma BM may consist of surgical resection of isolated or symptomatic lesions, WBRT or focal irradiation, and salvage chemotherapy with stem cell rescue. Even with aggressive multimodal treatment, the prognosis remains very poor and most patients with BM succumb to their disease (Paulino et al. 2003; Croog et al. 2010). Nevertheless, rare long-term survivors have been reported (Stefanowicz et al. 2011; Zhu et al. 2015; Croog et al. 2010). A study from St. Jude’s Children’s Research Hospital of high risk neuroblastoma patients treated for BM between 1979 and 1989 reported two long-term survivors who were treated with CSI and were alive at 50 and 62 months after diagnosis of relapse (Kellie et al. 1991). More recently, Croog et al. reported the results of 26 patients with parenchymal BM treated at Memorial Sloan Kettering Cancer Center from 1989 to 2007. The study included two cohorts: 16 patients who received CSI and 13 patients who received WBRT or focal irradiation in conjunction with their salvage treatment. The patients in the CSI cohort received between 12.6 and 21.6 Gy to the neuroaxis with or without a boost to the tumor cavity from 25.2 to 36.6 Gy in conjunction with intra-Ommaya radio-immunotherapy with 131I-8H9 and 131I-3F8. While 2 patients died of their disease (did not receive intra-Ommaya radio-immunotherapy) and 1 patient died of other causes, 13 patients remain alive at a median follow-up of 28 months. Three patients experienced a CNS recurrence which was treated with additional craniospinal or focal radiation therapy. Patients who were treated with WBRT or focal irradiation had a median survival of 8.8 months after CNS diagnosis, and 62% of patients experienced a CNS recurrence. Of note, the patients not receiving CSI also did not receive intra-Ommaya radioimmunotherapy at diagnosis of CNS disease (Croog et al. 2010). Zhu et al. reported their series of eight patients with high-risk neuroblastoma with brain metastases; of three long-term survivors (>2 years), two received craniospinal irradiation. None of these patients received intra-Ommaya radio-immunotherapy (Zhu et al. 2015). While the optimal regimen has not been determined, given that most long-term survivors reported in the literature received CSI, incorporating the neuroaxis in the radiotherapy treatment field and consideration of radio-immunotherapy appears to be the most effective treatment approach reported to date.
22.6 Hepatoblastoma
Hepatoblastoma is associated with multiple genetic syndromes (Beckwith-Wiedemann syndrome, Familial Adenomatous Polyposis syndrome, Li-Fraumeni syndrome, and Trisomy 18). It presents with right upper quadrant mass, anemia, thrombocytosis, abdominal pain, and increase in alpha-fetoprotein (AFP). Neoadjuvant chemotherapy followed by resection has improved survival to over 80% for patients who underwent a total resection (Goldman et al. 2007). As with many of the discussed tumors, the most common site of metastases is the lung. The incidence is between 3 and 5% (Wiens and Hattab 2014). A recent review of brain metastases arising from hepatoblastoma reports 39 cases of BM in published literature. Of these patients, 24% patients were diagnosed at age older than 4, and 63% had synchronous or prior pulmonary metastases. Treatment is similar to other brain metastases: surgery for solitary lesions, radiation, and/or chemotherapy (Rai and Feusner 2016). The cases of prolonged survival beyond 1 year were achieved with a combination of surgical resection, focal radiation therapy, and systemic chemotherapy (Rai and Feusner 2016; Robertson et al. 1997).
22.7 Germ Cell Tumors
Extracranial germ cell tumors account for approximately 3–5% of all pediatric cancers, typically arising from the ovaries, testes, coccyx, and mediastinum (Goldman et al. 2007). As intracranial germ cell tumors are discussed elsewhere in this book, the discussion below focuses specifically on BM from extracranial primaries.
The reported incidence of brain metastases from germ cell tumors varies significantly, ranging between 0.005 and 20% (Wiens and Hattab 2014; Suki et al. 2014; Spunt et al. 2004; Gobel et al. 2010). A study of 206 patients with extracranial germ cell tumors treated at St. Jude Children’s Research Hospital over a period of 40 years found 16 patients with CNS metastases. Two were diagnosed with metastases at presentation; 21 developed CNS disease during the disease course; and 2 patients were found incidentally to have CNS disease at autopsy evaluation (Spunt et al. 2004). Recent series from Indiana University reported an incidence of 0.5% with follow-up of over 3000 patients treated for germ cell tumors, while Suki et al. reported an incidence of 43%, with an elevated incidence particularly among patients with the choriocarcinoma histologic subtype (Wiens and Hattab 2014; Suki et al. 2014). Moreover, Stefanowicz et al. reported a case of patient with a mixed germ cell tumor who developed BM with pathologic evaluation demonstrating predominantly features of the choriocarcinoma component (Stefanowicz et al. 2011). As such, patients with choriocarcinoma may be at relative increased risk of BM in comparison to other histologic subtypes of germ cell tumors. Patients develop BM at a median of 7 months after initial diagnosis, with the majority of patients having pulmonary metastases prior to or at the time of BM (Spunt et al. 2004). In addition to histologic subtype and pulmonary metastases, primary mediastinal disease is also associated with increased risk for BM (Gobel et al. 2010).
Similar to other pediatric BM, patients with extracranial germ cell tumors with BM are treated with a combination of surgical resection, radiation, and chemotherapy. Most patients treated with radiation received between 20 and 35 Gy to the partial brain or 30–35 Gy to the whole brain with a boost of 3.5–14.8 Gy (Spunt et al. 2004). Though outcomes are generally poor, aggressive multimodal therapy may lead to rare long-term survivors (Wiens and Hattab 2014; Spunt et al. 2004).
22.8 Melanoma
Melanoma accounts for 1–3% of all pediatric cancers. Prognosis is dependent on stage, similar to that of adults. The incidence of BM in patients with melanoma has been reported between 8 and 18% and at a median of 20 months following diagnosis (Goldman et al. 2007; Rodriguez-Galindo et al. 1997). In a review of 44 pediatric melanoma patients treated at St. Jude’s Children’s Research Hospital, Rodriguez-Galindo et al. reported the outcomes of 8 patients who developed CNS disease. Of the six patients with available demographic information, five had extracranial metastatic disease, four with pulmonary metastases. On imaging, most of the lesions were supratentorial, though two patients had cerebellar lesions; three patients had solitary metastases; and most of the lesions demonstrated intralesional hemorrhage. The patients were treated with a combination of symptomatic management, WBRT to 45 Gy, chemotherapy, surgery, and interferon-alpha. Despite aggressive therapy, only three of eight patients were alive at a median of 5 months, with most dying of their CNS disease. The one long-term survivor in this series (alive without disease at 34 months) was treated with surgical resection, radiation therapy, multi-agent chemotherapy, and interferon-alpha (Rodriguez-Galindo et al. 1997). Similarly, in another reported case of a long-term survival of 13 years, the patient was treated with a similar multimodal approach, including surgical resection, radiotherapy, chemotherapy, and immunotherapy (Suki et al. 2014).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


