Pathology of the Head and Neck: Basic Considerations and New Concepts
Pathology of the Head and Neck: Basic Considerations and New Concepts
Elizabeth G. Demicco
Bruce M. Wenig
The role of the modern surgical pathologist is to identify tissue-based lesions and describe their known theranostic characteristics in order to accurately inform patient prognosis and clinical therapy. As such, the pathologist is an integral member of the multidisciplinary team responsible for the management of cancer of the head and neck. In the modern era, the creation of a pathologic diagnosis goes far beyond the straightforward “naming” of an entity based on histologic appearance, and may require close correlation with the gross specimen, clinical, radiographic, or molecular characteristics in order to evaluate and convey relevant information for appropriate patient care.
This chapter provides an overview of pathologic issues related to cancer of the head and neck and is divided into three sections. In the first, a general overview of the role of pathology in head and neck neoplasia is provided. “Histopathologic Parameters” section addresses histopathologic parameters evaluated by pathologists, with focus on those relevant in the assessment of mucosal squamous cell carcinoma. “Ancillary Studies (Pathologic Toolbox) and Applications” section provides an update of the diagnostic tools used by pathologists in routine clinical analysis, as well as a look at emerging technologies.
BASICS OF PATHOLOGY
Pathology Reporting
The pathology report provides the basis for all tissue-based clinical decisions. As such, it is a vital part of the patient’s medical record. At the most basic level, the pathology report contains a description of the tissue examined by the pathologist, at both the gross and microscopic levels. If a lesion is present, the pathologist is responsible for establishing the general type of process (inflammatory, infectious, benign neoplastic, or malignant) and subclassifying it as specifically as possible with a name that conveys the lineage of the cells involved and the etiology of the process. In addition, adequate diagnosis of malignant tumors requires further specification as to cellular differentiation. Where evaluable, the extent of tumor is reported, including whether it is in situ or invasive, its size, presence or absence of vascular/lymphatic invasion, perineural invasion, or presence at surgical margins. Lymph nodes must be identified and examined for metastases and extranodal extension. Ancillary testing required for diagnosis or therapeutic applications may also be contained within the surgical pathology report.
The Surgical Pathology Specimen
Pathology specimens come in a variety of forms, ranging from cyst contents or solid tumor aspirations, to needle core biopsies and incisional or excisional biopsies, to radical, complex resections. Each specimen type must be properly labeled and promptly submitted to ensure that it is appropriately processed for subsequent evaluation. Pathologic examination begins with examination of the gross surgical specimen. Note is made as to the type of specimen, for example, biopsy (shave, core, punch, incisional, excisional), resection, or lymph node dissection, and the overall size.
Gross examination of biopsy specimens may be relatively simple. The tissue biopsied should be noted, if identifiable, as epithelial/mucosal, bone, cartilage, or soft tissue, and the specimen should be submitted entirely, with or without additional sectioning, depending on specimen size.
For excisions and resections consisting of large, complex specimens, as frequently results from head and neck resections, the gross examination may be more involved. The intricate anatomy of the head and neck requires the surgical pathologist to be aware of the normal structures and their relationships to one another, in order to properly assess tumor involvement. Correct orientation is key to the establishment of the status of the surgical margins and requires a close working relationship between the pathologist and the surgeon. In many cases, surgeons can ensure proper orientation using sutures or ink to indicate critical margins. In complex cases, or those where nonmargin tissue has been disrupted, personal orientation of the pathologist to the specimen by the surgeon may be required.
After specimen orientation, the pathologist documents the structures present, sections the specimen, and records the size, appearance, and extent of the tumor. Sections submitted for histologic evaluation must represent areas requiring special attention, for example, surgical margins, lymph nodes, or bone invasion, that may impact the patient’s prognosis and future management. Failure to properly evaluate and section the gross specimen can have significant adverse effects on patient care.
Subsequent to appropriate fixation of the specimen in formalin or other agents, the tissue is further mechanically processed, dehydrated, and infiltrated with paraffin. Depending on the type of tissue, the length of time needed for proper fixation varies; for instance, adipose tissue requires a longer processing time. Calcified specimens such as bones must be decalcified in acid or chelating agents prior to processing. Decalcification can take from hours to weeks, based on the specific agent used, the density of bone, and the thickness of the section. Processed tissue is embedded by hand into paraffin blocks, sectioned into 4- to 5-µm sections, and stained with hematoxylin and eosin (H&E) or other histochemical stain for routine histologic evaluation. Typically, specimen processing for routine formalin-fixed, paraffin-embedded (FFPE) tissues may take from a few hours to a day for small biopsies rapidly processed in specialized processors, to many days for complex bone resection specimens.
The surgical pathologist is completely dependent upon the tissue procured by the surgeon. Without appropriate or adequate material, an accurate diagnosis cannot be rendered. In general, biopsies should avoid necrotic tissues near the center of lesions. Transitional areas showing the interface between normal and abnormal tissue are preferred, such as the edge of an ulcer or the line of demarcation between a verrucous proliferation and flat epithelium. Superficial biopsies are rarely helpful; invasion of epithelial lesions cannot be determined without evaluation of the epithelial-stromal interface, in a full-thickness section. Failure to provide an adequate biopsy results in diagnostic and therapeutic delays as well as frustration for the patient, clinician, and pathologist alike. Repeat biopsies may be distorted by postbiopsy inflammatory changes and degenerative artifact, further adding difficulty to appropriate interpretation.
It is also necessary to consider the differential diagnosis before placing biopsy tissue in fixative and sending it to pathology. Although in most circumstances, immediately placing tissue in fixative at the time of surgery is preferred, because tissues undergo ischemic changes and progressive autolysis the longer they remain unfixed, fresh tissue may be required by the pathology laboratory in certain circumstances. Ancillary studies such as flow cytometry or cytogenetics, which are frequently utilized in diagnosis of hematolymphoid proliferations, require fresh viable tissue, which must be sent directly from the operating room without delay for processing. Some laboratories may wish to save a portion of tissue in fixatives other than formalin for lymphoid biopsies for better preservation of cellular morphology.1 If ancillary studies such as electron microscopy, molecular studies, or cytogenetics are anticipated, it is also recommended that fresh tissue be sent without transport delay and the pathologist be notified that special handling is required.
The use of frozen tissue biorepositories established from fresh tissue after minimal ischemic time is encouraged for preservation of neoplastic and uninvolved tissues. However, gross specimen dissection is best handled by the pathologist, and incision or sectioning of the specimen by the surgical team is discouraged, as it may create difficulties in appropriate pathologic evaluation of margins, or sectioning for microscopy.
Cytology
Cytologic preparations may be obtained from bodily site washings, cyst fluid aspirations, or solid tumor aspirations or may be made directly from the surgical specimen. Touch imprints, squash preparations, and scrape cytology specimens prepared from surgical specimens are commonly used as an adjunct technique to frozen section evaluation, particularly for evaluation of thyroid nodules, lesions of the central nervous system, or hematolymphoid lesions. Touch imprints are prepared by pressing a glass slide against the cut surface of tumor and are best used for lymphoid or hematopoietic processes, where cells easily transfer from tissue to glass. Squash preparation involves cutting minute portions of tumor (<1 mm3) and pressing it between two slides to spread out cells. Squash preparations are best reserved for very soft tissues that spread easily under pressure. To harvest cells for scrape preparations, a scalpel blade is used to scrape the cut surface of a lesion, and the material is then smeared onto a glass slide.
Fine needle aspiration (FNA) biopsies are performed by inserting a thin needle attached to a syringe into the mass of interest. Cells are harvested by using light suction applied to the syringe while the needle is rapidly moved back and forth through the tissue to loosen cells and obtain a sample from different regions. Material collected may be smeared directly on slides or saved in fluid for paraffin-embedded cell block preparation or for fluid-based cytologic preparations created using filtration or centrifugation. Smeared slides are rapidly fixed or allowed to air dry and stained for histologic evaluation with H&E, Papanicolaou stain, or Diff-Quick preparation. Additional unstained preparations can also be set aside for immunohistochemistry or molecular studies.
FNA is a reliable and safe method to obtain cytology specimens from cystic lesions, lymph nodes, and many types of solid tumors. Early concerns about nerve damage and biopsy tract seeding by tumor cells were largely unfounded,2,3 with the most frequent complications being hematoma and infection. FNA biopsy is easily performed on palpable masses and may be used in conjunction with ultrasound imaging to improve accuracy and to target deep lesions.4,5 Because it is relatively cost- and labor-effective when applied to the readily accessible structures of the head and neck, FNA biopsy has become the preferred screening diagnostic modality for clinically concerning neck masses, including lesions arising in the parotid, thyroid, or lateral neck. As with all techniques in medicine, FNA biopsy and interpretation is highly dependent on experience, with higher diagnostic accuracies reported by high-volume academic centers,6 and improved rates of biopsy adequacy when performed or screened on-site for adequacy by cytopathologists.7,8,9,10 FNA biopsy has proved invaluable in presurgical planning and patient counseling, particularly in regard to defining the need for procedures with higher risk of morbidity, such as nerve sacrifice or neck dissection.11,12 FNA also allows for serial follow-up if a lesion continues to grow over time. Many surgeons do, however, prefer to verify cytologic diagnoses at the time of surgery with intraoperative frozen section (further discussed below).
Salivary Glands
Diagnosis of salivary gland neoplasms by FNA biopsy can be challenging. Many tumors are composed of a mixture of cell types, and even cytologically bland tumors can demonstrate an infiltrative growth pattern definitive for malignancy on final pathology.13 Common sources of diagnostic error include cellular pleomorphic adenoma, low-grade carcinomas such as low-grade mucoepidermoid or papillary cystadenocarcinoma, lymphoepithelial cysts, and lymphoproliferative disorders.14 Fortunately, the majority of tumors of the major salivary gland are benign, with pleomorphic adenoma and Warthin tumor representing the most common subtypes,15 resulting in a high pretest probability of benign diagnoses. FNA biopsy of lesions of the major salivary glands has a high specificity for malignancy, with reported sensitivity, specificity, and accuracy for malignant diagnosis ranging from 73% to 92%, 94% to 100%, and 90% to 98%, respectively.11,16,17,18
Because FNA biopsy allows for the creation of cell block tissues, diagnostic accuracy may be improved by incorporating immunohistochemical or molecular analyses into final pathologic interpretation. In most instances, salivary tumors will undergo resection for definitive therapy, regardless of the FNA interpretation as benign or malignant. However, because FNA biopsy is largely comparable in accuracy to frozen section,11,19,20 prior knowledge of the likely malignant potential enables the surgeon to better counsel the patients and prepare them in advance as to the necessity of wide resection, possibly including sacrifice of the facial nerve, or elective neck dissection. Discussions may also be entered into about postsurgical management and adjuvant therapy options, if required.
Neck Masses
It may be difficult to distinguish a benign from a malignant mass in the neck on the basis of clinical and radiographic information alone. Lesions may represent reactive lymphadenopathy, primary lymphomas, enlarging developmental cysts, infection (lymphadenitis), metastases to the lymph nodes, or benign or malignant mesenchymal tumors arising in soft tissue of the neck. Fortunately, ultrasound-guided FNA is one of the most accurate modalities for confirming the presence of metastatic disease in enlarged cervical nodes, with reported sensitivity for squamous cell carcinoma in solid lymph nodes ranging from 80% to 90%.21,22 FNA is less sensitive for malignancy in cystic neck masses, with sensitivity as low as 33%.23,24
Sensitivity and accuracy of FNA biopsy diagnosis of lymphoproliferative lesions is enhanced by concurrent immunocytochemistry, flow cytometry, and/or cytogenetic analyses. Dedicated FNA passes in addition to those needed for smear and cell block preparations may be required to obtain adequate material for these studies. In the absence of ancillary immunophenotyping studies or flow cytometry, the ability of FNA to correctly identify and classify lymphoma has been reported to be as low as 52%.25 Immunocytochemistry increases accuracy to 70% and flow cytometry to 75% to 81%.25,26 Flow cytometric analysis improves the ability to distinguish reactive lymphadenopathy from non-Hodgkin lymphoma, although it has little effect on identification of Hodgkin lymphoma. In other contemporary analyses, overall diagnostic accuracy of FNA biopsy of cervical lymphadenopathy reaches 82%,27 with highest overall accuracy (up to 100%) reported for identification of metastatic carcinoma and lowest (˜75%) for diagnosis of Hodgkin and non-Hodgkin lymphomas.26,27 Sensitivity and specificity of FNA biopsy for lymphoma is user dependent, and some series have noted no benefit to FNA biopsy of cervical lymphadenopathy.28 In the vast majority of cases, however, FNA biopsy interpretation by an experienced cytopathologist is an acceptable screening tool to triage management of a mass in the neck. Diagnoses of metastatic carcinoma in a cervical node appropriately trigger further evaluation to identify primary site or tumor-specific management protocols, while lesions concerning for lymphoma should undergo excisional biopsy for definitive diagnosis and subtyping. Benign or reactive lesions may be followed or rebiopsied depending on the level of clinical suspicion for malignancy.
Table 3.1 Bethesda Classification of Thyroid Cytology
Bethesda Classification
Frequency of Diagnosis
Risk of Malignancy
Recommended Management
1. Nondiagnostic, Unsatisfactory
<15%
N/A
Repeat FNA with ultrasound guidance
2. Benign
30%-75%
<2%
Clinical follow-up
3. Atypia of undetermined significance, Follicular lesion of uncertain significance
<10%
20%-40%
Repeat FNA
4. Follicular neoplasm, Suspicious for follicular neoplasm
˜5%
40%
Lobectomy
5. Suspicious for malignancy
<5%
70%
Thyroidectomy or lobectomy
6. Malignant
˜5%
>95%
Thyroidectomy
Thyroid Lesions
Thyroid nodules are one of the most common indications for neck FNA. Palpable nodules are identified in ˜5% of the adult population,29,30 with between 20% and 75% of the population having clinically unrecognized nodules.31,32 Reported incidence of thyroid carcinoma averages 5% in solitary nodules and 3% in multinodular goiter.33 Presurgical diagnosis via FNA biopsy prevents unneeded surgery for benign, nonprogressive lesions and helps to triage patients with a neoplasm for the appropriate procedure. Diagnostic accuracy of FNA biopsy of the thyroid is well established, with both specificity and sensitivity for malignancy of over 90% in large historical series.34,35,36,37
Standardization and interpretation of thyroid cytology has been greatly improved by the widespread adoption of systems such as the Bethesda reporting system, which classifies biopsies in a 6-tiered system as: Bethesda Class 1—nondiagnostic or unsatisfactory, Bethesda Class 2—benign, Bethesda Class 3— atypia of uncertain significance or follicular lesion of uncertain significance, Bethesda Class 4—follicular neoplasm or suspicious for follicular neoplasm, Bethesda Class 5—suspicious for malignancy, and Bethesda Class 6—malignant (Table 3.1).38,39,40
Nondiagnostic biopsies occur in 3% to 14% of thyroid FNA,41,42 with higher percentages resulting from procedures performed by less experienced clinicians in the absence of immediate pathologic assessment of adequacy and a lower incidence when performed and assessed in FNA clinics by trained cytopathologists.8,9,43 Ultrasound guidance further increases diagnostic success rates for difficult-to-palpate nodules.43 Benign lesions, for example, nodular hyperplasia or chronic thyroiditis, are identified on cytology in approximately 30% to 70% of aspirated nodules,41,44 with reported false-negative rates as low as 0% to 2%.44,45
The most challenging cases to manage are those diagnosed as Bethesda 3, as final diagnosis may range from benign nodular hyperplasia to papillary or follicular thyroid carcinoma. Initially, lesions with atypia of uncertain significance were predicted to run a 5% to 15% risk of malignancy.38 In practice, studies have reported malignancy rates ranging from 20% to 38%, not including incidentally discovered second lesions in the resected specimen.41,42,46 Moreover, the Bethesda category 3 is intended to account for no more than 10% of cases in a given practice.38 Overusage of the category can lead to additional management dilemmas. Although the Bethesda guidelines recommend repeat FNA for indeterminate lesions, and studies have shown that 40% to 50% of indeterminate lesions can be classified as benign on repeat FNA,42,46 other consensus guidelines recommend surgery as the next step.47 Triage of cytologically indeterminate lesions to reflex mutational analysis or commercial propriety gene expression analyses to more clearly delineate benign from malignant based on molecular signature has become increasing popular and is discussed in greater detail in “Ancillary Studies (Pathologic Toolbox) and Applications” section.
Lesions diagnosed as suspicious for follicular neoplasm on resection are found to be hyperplasias, adenomas, follicular carcinomas, and less frequently, papillary carcinoma, with malignancy rates of up to 40% to 46%.45,48 Determination of malignancy in an encapsulated follicular nodule requires identification of capsular or vascular invasion, features for which neither FNA nor frozen section is sensitive. Thus, appropriate management for Bethesda 4 lesions is lobectomy with evaluation of the entire capsule of the lesion on paraffin section. Oncocytic or “Hürthle cell” features are seen in nonneoplastic conditions as well as both benign and malignant neoplasms and have little diagnostic significance when reported on FNA.49,50
Approximately 70% of thyroid nodules reported as suspicious for malignancy on FNA (Bethesda 5) turn out to be malignant after definitive excision,48 and the vast majority of these are papillary thyroid carcinoma (PTC), whereas >95% of lesions with cytologic diagnosis of malignancy are confirmed after resection.51,52
FNA biopsy of the thyroid does elicit biopsy site changes in the thyroid gland, including hemorrhage, necrosis, cystic degeneration, fibrosis, inflammation, and nuclear cytologic atypia of adjacent tumor cells as well as squamous or oncocytic metaplasia. Capsular disruption by biopsy tract and subsequent entrapment of follicular cells may simulate capsular invasion. Such changes may be mistaken as evidence of malignancy on subsequent FNA biopsy or resection53,54,55 and must be interpreted with caution in postbiopsy resection specimens.
Orbit
FNA is sometimes used to diagnose deep unresectable posterior orbital tumors or those for which access would require large, complex craniofacial surgery. Reported success rate (defined as being diagnostically helpful or accurate) approached 80% in older studies,56,57 with the majority of lesions being lymphoproliferative or inflammatory conditions. FNA is rarely used in this location, due to the rarity of orbital masses and the technical skill required for the procedure. In the modern era, endoscopic surgery with direct visualization of the lesion is preferred to procure tissue for histopathologic evaluation.58,59 FNA has also been proposed as a diagnostic tool for uveal melanomas and other intraocular tumors,60,61 with sensitivity and specificity for malignancy reported as 100% and 98%, respectively. Complications include intraocular hemorrhage and rarely retinal detachment or tumor seeding.62
Intraoperative Consultation (Frozen Section)
During the course of surgery, it may be necessary to send a specimen for immediate pathologic examination, to help guide surgical decision making. Intraoperative consultation may take the form of gross specimen examination; cytologic preparations, as discussed above; or frozen section. Specimens may also be sent to the frozen section laboratory for rapid processing for biorepository or for tissue harvesting for cytogenetics, microbiology studies, flow cytometry, diagnostic mutational screening, or gene expression assays. Because the frozen section laboratory works in a time-sensitive fashion and may have multiple cases waiting for results before surgery may proceed, “curiosity frozens,” the result of which will not affect the procedure under way, but which may cause harm to the diagnostic material or delay other waiting cases, are strongly discouraged. It must be clearly understood that the frozen section interpretation is a preliminary diagnosis, intended only to provide immediate actionable information to the surgeons at the time of surgery, and is not meant to be the basis for postsurgical treatment or patient management. Decisions about adjuvant therapy must therefore be deferred until a definitive final diagnosis is rendered on FFPE tissues.
Appropriate uses of intraoperative consultation include establishing biopsy adequacy, triage of tissue for ancillary studies such as flow cytometry, or to make a preliminary diagnosis that will affect the extent of surgery. Margins are evaluated for adequacy of clearance, and additional margins may be sent until tumor clearance is achieved. Specimens may also be sent for tissue confirmation, such as confirmation of parathyroid glands in need of preservation during thyroidectomy.
Frozen section analysis requires that tissue be rapidly examined at the gross level, oriented, and inked if indicated and sections cut for histologic analysis. These tissue sections are embedded in gel matrix and rapidly frozen at -20°C to -30°C. Thin, 4- to 7-µm sections are cut using a microtome, and the tissue is stained with H&E for evaluation. Different tissues have varying water and lipid contents causing them to freeze at different rates, which may lead to tissue and cellular distortion. Sectioning frozen tissue may be technically difficult, particularly for adipose or dense fibrous tissue, and may not produce satisfactory sections for interpretation. Heavily calcified tissues, such as bone, often cannot be sectioned at all. Air-drying artifact may also be introduced if sections are not fixed rapidly enough after being cut. Some tumors, in particular melanocytic lesions, should not be sent for frozen evaluation, as frozen artifact precludes sufficiently accurate identification of malignant cells.
Due to the above technical limitations of the technique combined with the rapid turnaround time required (within 20 minutes from receipt as recommended by the College of American Pathologists), frozen section may be less accurate than paraffin sections. Reported overall error rates for frozen section vary, based on both specimen type and experience. In large studies of general surgical cases, accuracy of frozen section reaches 98%, with deferral rates of 2% to 3%.63,64,65 Overall, historical concordance rates are similar for head and neck surgeries,66,67 which are among the services most heavily reliant on intraoperative consultation.65 Discrepancy rates on surgical margins are much higher than those for any other specimen type68,69,70,71,72 and are further discussed below.
In addition to specimen-, technical-, and sampling-related errors, frozen section “errors” also include misinterpretation or miscommunication of results.73 Read-back verification by the surgeon is required to ensure proper diagnosis communication between the interpreting pathologist and treating surgeon.74
Margins
Negative surgical resection margins with complete clearance of malignancy are required for local cancer control.75 Margins are therefore frequently sent for frozen section during the course of resection of mucosal squamous cell carcinomas and may be a point of controversy for both pathologists and surgeons. Factors impacting on proper evaluation of margins include the type and complexity of surgical specimen, orientation of the specimen, adequate sectioning and gross evaluation, and correct interpretation of histologic findings. Despite best efforts, all frozen section diagnoses carry the risk that permanent section will reveal tumor not diagnosed at the time of frozen section. In general, accuracy of frozen section in the diagnosis of margins ranges from 89% to 99%,76,77,78 with specificity >95%, but low sensitivity. Many groups report that approximately half of the cases with positive final margins were not identified on frozen (range of missed positive margins, 15% to 83%).68,69,70,71,72,77 False-negative margins on frozen section most frequently result from sampling error, in which carcinoma is absent on the frozen section slide but is found on permanent sections after deeper sectioning.76 False negatives also occur when the area sampled on frozen section did not truly represent the closest extent of tumor to margin.68,79 Less frequently, false negatives result from diagnostic misinterpretation of tissue present on the slide, a source of error that may depend on the specimen type, case volume, degree of experience with head and neck tumor evaluation by involved surgical pathologists, and presence of altered tissue states after adjuvant therapy. Frozen section evaluation of margins is particularly problematic in tumors that have been previously irradiated.69,77
Historically, the value of frozen section margin evaluation in improving survival was based on the observation that patients with negative margins at the time of frozen section had local recurrence rates of 14%, compared with 20% in patients who required additional supplementary margins to be taken for clearance and 80% in patients for whom adequate clearance was not achievable.75
Some authors have questioned the value of frozen section evaluation on local disease control and survival.69,70,80 Gerber et al.68 recently reported that, in a retrospective series of 178 patients undergoing primary resection of oral cavity squamous cell carcinomas with curative intent, frozen section was performed in 111 patients, with positive final margins in 20% of cases, compared with 28% of those who did not undergo intraoperative consult. This difference was not statistically significant.68 DiNardo and coauthors69 had similar results and suggested that, after taking into account both accuracy and cost-effectiveness, frozen section evaluation was best used judiciously and largely reserved for patients in whom subsequent margin revision would have the highest chance of success. Effect of frozen section on margin status is also dependent on other factors, such as tumor size,68 site,67 and the skill of both the surgeon and the pathologist. Studies have reported widely varying rates of positive margins on final pathology, from between 4% and 53%,71,72,81,82,83,84,85,86,87 suggesting that individual institutions should establish their own quality assurance parameters for when to perform margin frozen section and how those results should affect patient management.
Diagnosis
Masses of every conceivable anatomic site pass through the frozen section laboratory for intraoperative diagnosis on a regular basis. In the head and neck, salivary tumors, thyroid nodules, parathyroid lesions, lymph nodes, and mucosal biopsies form the bulk of this material. FNA has made inroads in diminishing the use of frozen section diagnosis in many of these lesions, but some surgeons prefer a cautious approach with review of tissue-based diagnostic material prior to embarking upon an aggressive surgical procedure.
Frozen section has been reported to have sensitivity and specificity as high as 98.5% and 99%, respectively, for diagnosis of malignant lesions of the parotid, although it is less accurate at distinguishing between different types of benign or malignant tumor.88,89,90 Frozen section can also distinguish true salivary gland processes from metastatic tumor in periparotid lymph nodes and can triage lymphoid proliferations to appropriate ancillary studies. Compared to cytology, frozen section is reported to have a lower false-negative rate for detection of salivary gland malignancy.91
Thyroid lesions are frequently sent for frozen section to confirm malignant diagnoses made on FNA or to attempt a definitive diagnosis of lesions with indeterminate or suspicious cytology. Not all such frozen sections are appropriate. FNA diagnosis of PTC (Bethesda 6) has a <5% false-positive rate,92,93,94 and frozen section is not warranted prior to proceeding with total thyroidectomy. Likewise, frozen section of nodules with a benign diagnosis on FNA is unwarranted95,96,97 and provides no additional diagnostic information unless a clinically suspicious second nodule that was not previously biopsied is detected during the course of the operation. Frozen section is insensitive for malignancy in tumors with an FNA diagnosis of “follicular neoplasm,” which may include hyperplasia, follicular adenoma, non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), follicular carcinoma, or follicular variant of papillary carcinoma in the differential diagnosis.98,99 Follicular carcinoma requires identification of vascular and/or capsular invasion for diagnosis, features that are often focal and unlikely to be serendipitously present on frozen section, whereas the follicular variant of papillary carcinoma may present with subtle nuclear features that cannot be recognized in frozen tissue.100,101 Frozen section has a variable sensitivity of 17% to 70% and specificity of 100% in malignant diagnosis of follicular pattern neoplasms, but a deferral rate of over 50%.102,103,104,105,106,107
Frozen section, in conjunction with intraoperative touch or scrape preparations, is best used to evaluate lesions diagnosed as atypical or suspicious for malignancy and can usually detect PTC; medullary carcinoma, poorly differentiated; and anaplastic carcinoma, among other malignancies, with an 84% sensitivity for malignancy, 100% specificity, and 57% likelihood of diagnosing PTC in cases with a preoperative diagnosis of Bethesda 5 lesion.93,108 Cytologic preparations are recommended as an adjunct study to better examine nuclear details for characteristic features of PTC. It is estimated that frozen section consultation alters the surgical procedure in <1% of cases with preoperative benign diagnosis on FNA,96 ˜5% of those with follicular diagnosis,109 and 20% to 57% of those with cytologically suspicious diagnosis.96,110
Although lymphoid proliferations are rarely diagnosed on frozen section, frozen section of lymph nodes is valuable in intraoperative diagnosis of lymph nodes metastases111 and has been suggested as a methodology for sentinel lymph node evaluation in squamous cell carcinomas of the head and neck112 (discussed in greater detail in “Histopathologic Parameters” section below).
HISTOPATHOLOGIC PARAMETERS
Tissue lesions can be characterized by a number of different parameters. At the most basic level, histologic review determines if the sampled tissue is normal or atypical. Atypical conditions include reactive, inflammatory, and neoplastic conditions among others. For neoplastic lesions, one critical distinction is benign or malignant. However, classifying a tumor simply as malignant conveys insufficient prognostic and therapeutic information. To this end, the art of pathology has developed multiple systems of tumor classification and subclassification to more precisely delineate behavior.
Tumor Classification
Lineage
Tumors are typically classified based on the histologic line of differentiation (commonly referred to as the cell of origin) as epithelial, mesenchymal, hematopoietic/lymphoid, or neural/neuroectodermal. Within lineage, there exists a myriad of more specific subtypes, which can generally be identified based on histologic, immunophenotypic, and/or molecular characteristics. By far, the most common malignant tumors affecting the head and neck arise from mucosal or glandular epithelium. Non-glandular-derived epithelial malignancies are carcinomas, with squamous cell carcinoma being the most common subtype. Gland-forming epithelial malignancies are adenocarcinomas. Malignant mesenchymal tumors are termed sarcomas, whereas lymphoproliferative malignancies are lymphomas. Neuroectodermal structures give rise to a variety of benign and malignant tumors, including melanoma, olfactory neuroblastomas, malignant peripheral nerve sheath tumors, and others.
Squamous Cell Carcinoma. Squamous cell carcinoma is the single most common type of carcinoma affecting the head and neck. Tumors arise within stratified squamous epithelium, both cutaneous and mucosal, including oral cavity, pharynx, larynx, and nasal cavity. Squamous cell carcinoma may be further classified into conventional type or as one of several uncommon subtypes, each with its own distinctive clinicopathologic characteristics and behaviors (Table 3.2).
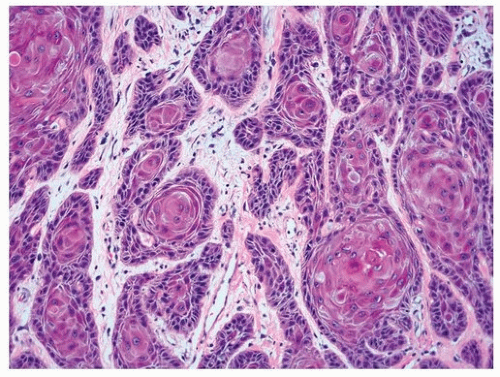
Within the category of conventional squamous cell carcinoma, a further distinction is made between keratinizing and nonkeratinizing or hybrid tumors (Table 3.3).113,114,115,116,117 Keratinizing squamous cell carcinomas historically represent the bulk of squamous cell carcinomas arising in the oral cavity and larynx and are associated with a history of alcohol consumption, smoking, or chronic epithelial inflammatory conditions. Histologically, keratinizing squamous cell carcinomas are characterized by stratified malignant epithelium with distinct cell borders and intercellular bridging. Keratinization may be represented as cytoplasmic eosinophilia in more poorly differentiated cases or more typically by the presence of anucleate keratinocytes or “pearl” formation in well-differentiated tumors (Fig. 3.1). Keratinizing squamous cell carcinomas are, in general, highly aggressive, and advanced disease responds poorly to therapy.118,119 Five-year survival rates depend on TNM stage and site and vary from up to 85% for glottic tumors to ˜50% for supraglottic, hypopharyngeal, or buccal tumors.119,120
Table 3.2 Classification of Squamous Cell Carcinoma Variants of the Head and Neck
Conventional squamous cell carcinoma
Keratinizing
Nonkeratinizing (frequently HPV associated)
Variants
Acantholytic
Adenosquamous
Basaloid
Spindle cell
Verrucous
Nasopharyngeal carcinoma
Basaloid
Keratinizing
Nonkeratinizing (EBV-associated)
Differentiated
Undifferentiated
Sinonasal undifferentiated carcinoma
NUT midline carcinoma
EBV, Epstein-Barr virus; HPV, human papillomavirus.
Table 3.3 Distinction Between HPV-Positive and HPV-Negative Squamous Cell Carcinoma
HPV Positive
HPV Negative
Age
<60 y
>60 y
Gender
M > F
M > F
Site
Oropharynx (lingual and palatine tonsils)
All mucosal sites of oral cavity, pharynx, larynx, nasal cavity
Risk factors
Number of sexual partners, Immunosuppression
Tobacco, alcohol, chronic inflammatory conditions
Histology
Nonkeratinizing
Keratinizing
P16 expression
Positive (strong nuclear and cytoplasmic expression in >70% of cells)
Negative to patchy weak expression
Stage at presentation
Early metastasis with small primary tumor (pT1N2)
Larger primary tumor, but later metastasis. (pT1-2, N0-1)
Morphology of metastases
Cystic
Solid
Prognosis
5-year survival 70%-80%
5-year survival 25%-85%
HPV, human papillomavirus.
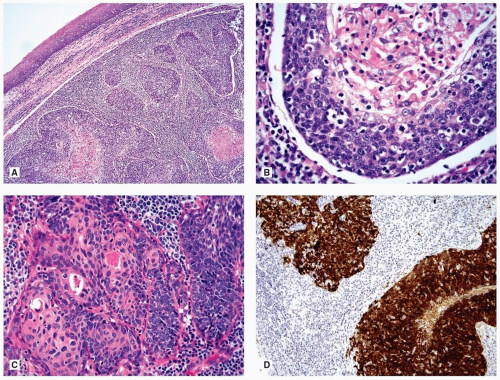
Nonkeratinizing and hybrid (focally keratinizing) squamous cell carcinomas are characterized by the complete/near absence of keratinization or by the admixture of nonkeratinizing and keratinizing cells, respectively. These tumors arise nearly exclusively in the oropharynx in association with tonsillar crypt epithelium and are most often associated with infection by high-risk human papillomavirus (HPV) genotypes, mainly HPV16, 33, 35 or 18 (Fig. 3.2).121,122 As keratinizing squamous cell carcinomas have shown declining incidence in the past decade with decreased smoking prevalence, the proportion of HPV-associated carcinomas has increased.123,124,125 These tumors possess a distinctive pathophysiology, with early lymph node metastasis, but superior outcomes compared to conventional squamous cell carcinoma, even in advanced disease.113,126,127 Five-year relative survival rates are estimated to be ˜75% compared to 24% to 40% for non-HPV-associated oropharyngeal cancers.128
Figure 3.1. Invasive keratinizing squamous cell carcinoma characterized by cells with prominent cytoplasmic eosinophilia (keratinization) and clear spaces in between cells (intercellular bridging).
Figure 3.2. Oropharyngeal HPV-associated carcinoma. A: Low magnification of a submucosal infiltrative solid and cystic neoplasm. B: At higher magnification, the lesional cells are devoid of keratinization (i.e., nonkeratinizing). C: Hybrid carcinoma showing an admixture of nonkeratinizing and keratinizing malignant cells. D: Diffuse and strong p16 immunoreactivity (nuclear and cytoplasmic) represents a surrogate marker for HPV16 confirms the neoplasm as HPV associated; reflex in situ hybridization and PCR analysis identified the presence of high-risk HPV (not shown).
Nonkeratinizing squamous cell carcinoma often presents with neck metastasis and clinically occult primary lesion. Deep biopsy of lingual and pharyngeal tonsils or tonsillectomy may be required to locate the primary tumor, as microscopic tumors often arise deep within tonsillar crypts and are not detectable by superficial biopsy.129 Nonkeratinizing tumors are variously described as having “immature,” “transitional,” “basaloid,” or “poorly differentiated” histologic features, although they are now thought to represent relatively well-differentiated tumors recapitulating the phenotype of tonsillar crypt epithelium. Tumors characteristically express strong and diffuse nuclear and cytoplasmic p16 protein as a side effect of oncogenic viral protein inhibition of RB-mediated cell cycle arrest.130 The presence of p16 immunoreactivity in a cervical nodal metastasis without a known primary cancer is strongly correlated to an oropharyngeal primary cancer.
Basaloid squamous cell carcinoma was initially described as a highly aggressive subset of squamous cell carcinoma that occurred in older males with a peak incidence from 60 to 80 years and showed malignant differentiation toward a phenotype similar to that of basal cells.131 Basaloid squamous cell carcinoma may arise in a variety of mucosal sites in the upper aerodigestive tract including the larynx, hypopharynx, oropharynx, and sinonasal tract. Irrespective of site of origin, the histologic findings are similar, and tumors are characterized by multilobular, nested growth pattern with frequent comedonecrosis, foci of abrupt keratinization, and stromal hyalinization (Fig. 3.3). The overlying mucosa shows only limited foci of intraepithelial dysplasia. Unfortunately, nonkeratinizing, HPV-associated carcinomas have a similar-appearing cellular differentiation, and the term basaloid squamous cell carcinoma has been subverted by many authors to include both the highly aggressive “true” HPV-negative basaloid squamous cell carcinomas and the less aggressive nonkeratinizing HPVassociated variant.132,133 Communication between pathologist and treating clinician is essential to ensure that the appropriate prognostic information is conveyed. When in doubt, HPV testing is essential.132,133
Figure 3.3. Basaloid squamous cell carcinoma composed of cells with hyperchromatic nuclei (basaloid cells), nuclear pleomorphism, and increased mitotic activity. The tumor nests include comedo-type necrosis (top) and associated stromal hyalinization (bottom) resembling the reduplicated basement membrane seen in salivary gland neoplasms. In areas not shown, there was evidence of squamous differentiation. This tumor was HPV negative.
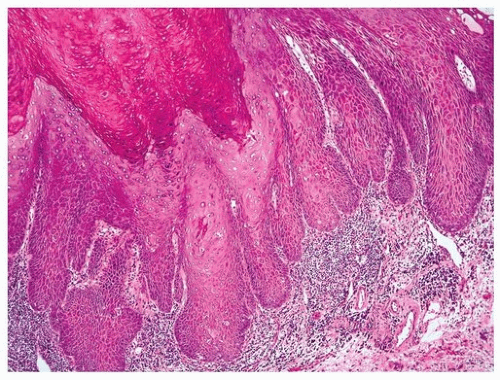
Figure 3.4. Verrucous carcinoma characterized by (tiered) keratosis of the surface and a bland epithelial proliferation with downward extending rete ridges (so-called pushing margin) and absence of epithelial dysplasia.
Verrucous squamous cell carcinoma is a locally aggressive variant most commonly arising in the oral cavity of older patients and characterized by a markedly hyperplastic, filiform, warty architecture, and a broad, pushing invasive growth pattern (Fig. 3.4).134,135 These tumors may be extremely difficult to diagnose on biopsy, as the large cell size and abundant keratinizing cytoplasm often make nuclear enlargement difficult to appreciate. Moreover, invasion is difficult to assess in the absence of infiltration. Proper diagnosis therefore relies on an adequate biopsy specimen. Biopsy is best taken from the edge of the lesion to show the interface between tumor and normal mucosa and should be deep enough to reach underlying submucosa. Pure verrucous carcinomas do not exhibit any infiltrative growth and do not metastasize. The presence of infiltrative nests, “hybrid verrucous carcinoma,” is associated with behavior akin to conventional squamous cell carcinomas. Verrucous carcinomas are associated with chronic inflammation and usage of smokeless tobacco.136 Tumors may cause extensive local morbidity if left untreated, but in general, prognosis is good, with 5-year survival rates reported from 80% to 95%.118,136
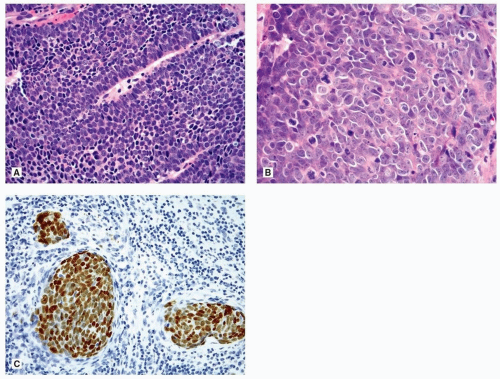
Sinonasal Undifferentiated Carcinoma. Sinonasal undifferentiated carcinoma (SNUC) is a rare, aggressive malignancy characterized by rapid local spread. Tumors are composed of nests, sheets, and trabeculae of malignant, poorly differentiated cells with scant cytoplasm, large nuclei, and, typically, prominent nucleoli (Fig. 3.5). Mitotic rate is high, and necrosis is frequently abundant. Malignant cells may express simple keratins and rarely neuroendocrine markers.137 The etiology of SNUC is unclear; tumors are negative for Epstein-Barr virus (EBV) and HPV. Because of their rapid onset and extensive local involvement at presentation, SNUC have poor prognosis. The major differential diagnoses for SNUC include (in no particular order) rhabdomyosarcoma, olfactory neuroblastoma, nasopharyngeal undifferentiated carcinoma, small cell neuroendocrine carcinoma, poorly differentiated squamous cell carcinoma, and NUT midline carcinoma among others (Table 3.4). When the diagnosis is in question, correlation with the clinical and radiographic features is critical to making the correct diagnosis. Successful treatment is dependent on radical resection in conjunction with adjunct chemoradiation.137
Figure 3.5. Sinonasal undifferentiated carcinoma (SNUC). A: Sinonasal high-grade malignant neoplasm characterized by cells with large nuclei, prominent nucleoli, scant cytoplasm, and increased mitotic activity lacking evidence of cellular differentiation. B: Cytokeratin (CAM5.2) immunoreactivity confirms the neoplasm as being of epithelial cell origin and in the absence of immunoreactivity indicative of any other tumor type as well as absence of EBV, the clinical findings, and location of the tumor coupled with the light microscopic findings would be diagnostic for SNUC.
Table 3.4 Small Round Cell Malignant Tumors of the Sinonasal Tract
Epithelial
Neuroendocrine carcinomas
NUT midline carcinoma
Sinonasal undifferentiated carcinoma
SMARCB1 (INI-1)-deficient carcinoma of the sinonasal tract
Mesenchymal
Ewing family of tumors (Ewing sarcoma/primitive neuroectodermal tumor)
Rhabdomyosarcoma
Alveolar
Embryonal
Neuroectodermal
Melanoma
Olfactory neuroblastoma
Hematolymphoid
Lymphomas (i.e., NK/T cell lymphoma, nasal type)
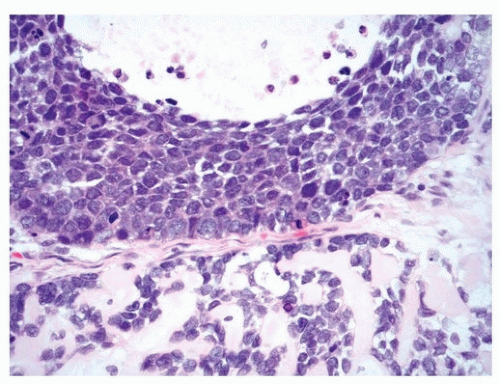
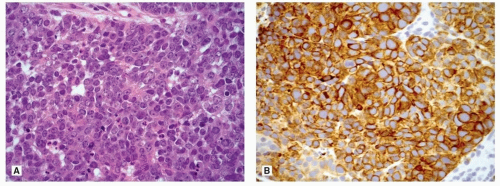
Nasopharyngeal Carcinoma. Nasopharyngeal carcinoma (NPC) represents a phenotypic spectrum of squamous cell carcinoma types, including keratinizing, nonkeratinizing, and basaloid morphologies. The nonkeratinizing type is most common and accounts for 75% of all cases of NPC. Nonkeratinizing NPC typically occurs in adults, with peak incidence between 40 and 60 years, and is two to three times more common in men than women. Tumors tend to have extensive local spread, early lymph node metastases, and the propensity for hematogenous metastases.138 Nonkeratinizing NPC is subdivided into two morphologic types including differentiated (15% of all NPC) and undifferentiated (60% of all NPC). The differentiated subtype of nonkeratinizing NPC (formerly referred to as lymphoepithelioma) is characterized by the presence of stratification of malignant cells with well-defined borders (Fig. 3.6), whereas the undifferentiated subtype of NPC (NPUC) shows a syncytial growth pattern with crowding of cells and large, vesicular nuclei with prominent nucleoli (Fig. 3.6). In some cases, the malignant cells may be spindle shaped. Clinically, there is no relevance to the distinction between differentiated and undifferentiated NPC. Both types are characterized by an associated nonneoplastic (benign) lymphoid proliferation that may overrun and obscure the malignant cells, resulting in the so-called lymphoepithelial morphology with tumor cells arrayed in plexiform nests interrupted by aggregates of nonneoplastic lymphocytes.
Nonkeratinizing NPCs are frequently associated with Epstein-Barr virus (EBV), and the presence of diffuse (nuclear) positivity for Epstein-Barr encoded RNA (EBER) by in situ hybridization (ISH) is diagnostic (Fig. 3.6).138 NPC is more common in regions where EBV is endemic (e.g., China) and is rare in the United States.138 It is critical to make the distinction between nasopharyngeal nonkeratinizing carcinoma (associated with EBV) and oropharyngeal nonkeratinizing carcinoma (associated with HPV) as the behavior and prognosis are different, although both result from viral infections. Another potential diagnostic dilemma given overlapping histologic features and presence of cytokeratin immunoreactivity includes differentiating NPC from SNUC. The presence or absence of EBV will allow the distinction between these tumors with NPC associated with EBV and SNUC negative for EBV. Keratinizing and basaloid NPC behave similarly to their counterparts arising elsewhere in the upper aerodigestive tract.
Of note, the use of the designation viral-associated carcinoma for NPC (EBV-associated) and oropharyngeal carcinoma (HPV-associated) may be adopted in future classifications of head and neck neoplasm.
Figure 3.6. Nasopharyngeal carcinoma, nonkeratinizing types. A: Differentiated type characterized by cohesive cords, stratification of malignant cells with well-defined borders. B: Undifferentiated type shows syncytial growth pattern with crowded cells and large vesicular nuclei with prominent nucleoli. C: In situ hybridization for Epstein-Barr-encoded RNA (EBER) is diffusely positive (nuclear staining). Both subtypes of nasopharyngeal carcinoma, nonkeratinizing types, are associated with EBV.
NUT Midline Carcinoma. NUT midline carcinoma is a rare, aggressive malignancy defined by chromosomal rearrangements, most commonly between 15q14 and 19p13.1, resulting in fusion of the NUT gene locus to BRDU4 or BRDU3, among other partners, and subsequent overexpression of NUT protein.139,140 Although NUT midline carcinoma may arise anywhere in the body, the majority of reported cases arise in the upper respiratory tract and mediastinum.139 Histologically, NUT midline carcinomas appear poorly differentiated and may or may not exhibit evidence of squamous differentiation in the form of abrupt keratinization. The presence of immunoreactivity for NUT protein marker (nuclear staining) confirms the diagnosis. In the sinonasal tract, NUT carcinomas are thought to be frequently misdiagnosed as squamous cell carcinoma or SNUC. The distinction is important because NUT midline carcinomas may present at any age and have an average survival of less than a year.139
Carcinoma of the Salivary Glands. Salivary gland carcinomas are rare, with reported incidence annual rates in the United States of only 1.3/100,000 individuals. The parotid gland is the most common site and accounts for up to 80% of cases, followed by the minor salivary glands, submandibular gland, and sublingual gland. Most malignant tumors arise in the superficial lobe of the parotid gland. The likelihood of a salivary gland tumor to be malignant also varies by site. Carcinoma is identified in <30% of parotid tumors, 40% of submandibular gland tumors, 50% of minor salivary gland tumors, and up to 90% of sublingual masses.141
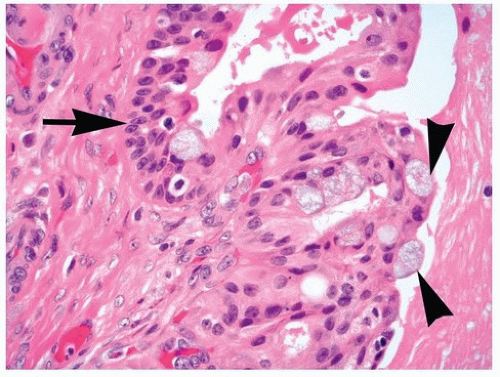
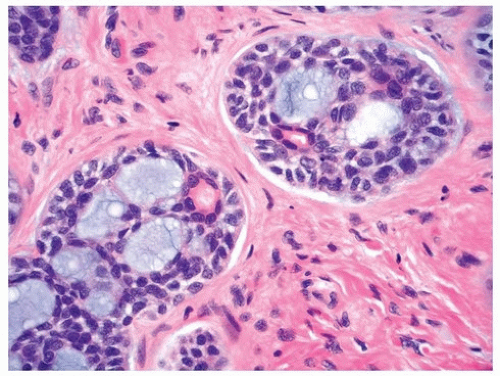
Diagnosis of salivary gland neoplasia is made more complex by the number of described types of carcinoma, with over 20 malignant salivary gland carcinomas recognized (Table 3.5). The most common primary salivary gland malignancies, each accounting for 10% to 25% of cases, are mucoepidermoid carcinoma and adenoid cystic carcinoma (Figs. 3.7 and 3.8), with specific incidence rates showing geographic variation.142,143 Precise histologic diagnosis of salivary gland tumors can be difficult, as many tumors are composed of a mixture of cell types or may show a spectrum of morphologic phenotypes. As a result, adenocarcinoma not otherwise specified (NOS) accounts for ˜10% of cases.142
The in-depth description of the many types of salivary gland carcinoma is beyond the scope of this chapter. However, recent studies have elucidated characteristic genomic alterations associated with several variants, which may enable improved diagnosis in future (Table 3.6).144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159 Moreover, our improved ability to accurately segregate tumors by molecular alterations will enable more accurate prognostication.
Thyroid and Parathyroid Carcinomas. Thyroid carcinoma is the most common endocrine malignancy. Tumors arise from either the follicular epithelium (papillary, follicular, poorly differentiated, and anaplastic thyroid carcinomas) or parafollicular C-cells of neuroectodermal origin (medullary thyroid carcinoma [MTC]) and have been shown to demonstrate specific genetic mutations (Table 3.7).
PTC is by far the most common variant of thyroid carcinoma, accounting for ˜86% of thyroid carcinomas, with a rising incidence over the past few decades.160,161 Controversy exists as to the cause of this dramatic increase.160 Whereas some authors cite the improved ability to detect disease, and more frequent discovery of incidental thyroid nodules on imaging studies undertaken for other reasons.161,162 It is now thought that the reported increase in carcinoma is due to overdiagnosis of indolent disease.163,164 In particular, the non-invasive, encapsulated follicular variant of papillary thyroid carcinoma has been determined to have low risk of aggressive behavior and has been recently renamed as non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP).165 In addition, it is suspected that many incidentally discovered “microcarcinomas” found on resection for benign solitary nodule or multinodular goiter represent at best, premalignant change and, based on their benign behavior in recent series, should not truly be considered to be a true malignant disease.166,167
Table 3.5 Classification of Salivary Gland Carcinoma
Acinic cell carcinoma
Adenoid cystic carcinoma
Adenocarcinoma, NOS
Adenosquamous carcinoma
Basal cell adenocarcinoma
Carcinoma ex pleomorphic adenoma
Intracapsular
Invasive
Metastasizing pleomorphic adenoma
Carcinosarcoma
Cribriform adenocarcinoma of minor salivary gland origin
Figure 3.7. Mucoepidermoid carcinoma of the parotid gland demonstrating the classic admixture of cell types including mucocytes (arrowheads), epidermoid cells (arrow), and intermediate cells, the latter composed of cells that are more spindle shaped with hyperchromatic nuclei.
Figure 3.8. Adenoid cystic carcinoma with classic histology including the cribriform growth pattern (“Swiss cheese”) predominantly composed of abluminal (myoepithelial) cells surrounding cystic spaces and less conspicuous but identifiable true glands surrounded by luminal (epithelial) cells.
Table 3.7 Common Genetic Alterations in Thyroid Neoplasia
Tumor Type
Affected Genes
Prevalence
Follicular adenoma
RAS
10%
Noninvasive follicular thyroid
RAS
30%
Neoplasm with papillarylike nuclear features (NIFTP)
BRAF
PAX8/PPARγ
<5%
20%
Follicular carcinoma
RAS
BRAF
PAX8/PPARγ
translocation
45%
<10%
35%-45%
Papillary carcinoma
TRK
<5%
Follicular variant
RAS
BRAF
PAX8/PPARγ
translocation
RET/PTC
translocation
40%
10%
10%
3%
Classical variant
RAS
BRAF
RET/PTC
translocation
1%
70%
10%
Poorly differentiated carcinoma
RAS
BRAF
20%
20%
Anaplastic carcinoma
RAS
BRAF
45%
25%
Medullary carcinoma
Sporadic
Familial
RET
RET, germ-line mutation
50%
>95%
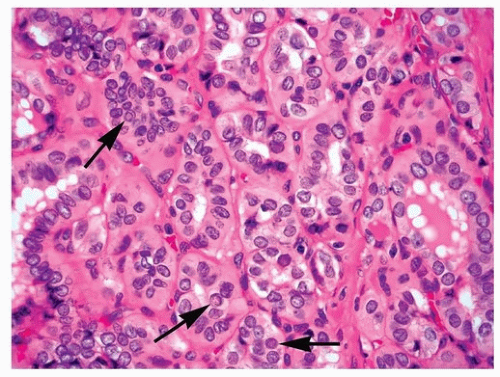
Classical papillary carcinomas are diagnosed based on their nuclear features on FFPE sections. These features include enlarged, pale to optically clear nuclei with peripherally located, small nucleoli and the presence of nuclear membrane irregularities typically visualized as longitudinal grooves and pseudoinclusions (Fig. 3.9). Clearing of the nuclei is an artifact of formalin fixation and is not seen in frozen sections, cytology preparations, or tumors fixed in other media.101,168 Tumor cells often have abundant cytoplasm. The architecture of papillary tumors may be papillary or follicular; colloid is often scant. Intratumoral fibrosis and calcification is common. At the molecular level, classical PTC is characterized by a high frequency of mutations in the mitogen-activated protein kinase (MAPK) pathway, with activating BRAF mutations (most commonly n.T1796A (p.V600E)) accounting for nearly 70% of cases,169,170,171,172 whereas RET/PTC gene rearrangements each account for 10% to 20% and TRK rearrangements for ˜5%.173RAS mutations are rare in classical papillary carcinoma (Table 3.7).172,174,175,176,177,178,179 Papillary carcinomas invade lymphatics early and spread to lymph nodes of the neck. Despite early nodal metastasis, papillary carcinomas have a relatively good prognosis. Survival is predicted by age and tumor size; younger patients have excellent long-term survival rates, whereas older patients and those with large primaries progress more rapidly.180,181
Figure 3.9. Papillary thyroid carcinoma. The diagnosis is predicated on the nuclear alterations including enlarged nuclei with variation in size and shape, very fine-appearing nuclear chromatin, overlapping, and crowding of nuclei, nuclear grooves, and nuclear (pseudo)inclusions (arrows).
Several variants of papillary thyroid carcinoma exist, the most controversial of which is the follicular variant papillary thyroid carcinoma (FVPTC). FVPTCs are distinguished by a lack of papillary architecture and subtle nuclear features of papillary carcinoma. The main differential diagnosis for invasive FVPTC is follicular carcinoma. Up until recently, encapsulated FVPTC without evidence of vascular or capsular invasion were also considered to be malignant despite low intraobserver agreement on the diagnosis.182,183 However, increased recognition of the non-aggressive behavior of these tumors, and histologic and molecular similarity to follicular adenoma and carcinoma175,184,185,186 has led to a new nomenclature of NIFTP. The new terminology was selected to reduce overdiagnosis of carcinoma and overtreatment of a tumor which poses little risk to the patient.166,187
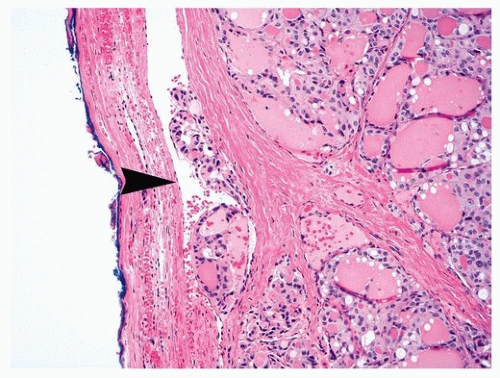
Follicular thyroid carcinomas constitute about 10% of thyroid malignancies.160 Tumors typically have a microfollicular growth pattern and bland nuclear features, and are distinguishable from adenomas only by the presence of invasion. All solitary encapsulated nodules of the thyroid must have the entire capsule submitted for histologic evaluation, as the presence of either tumor invasion through the capsule into normal thyroid gland parenchyma or angioinvasion is diagnostic of malignancy (Fig. 3.10). Because they have a predilection for angioinvasion, follicular carcinomas spread hematogenously, generally bypassing regional lymph nodes to metastasize directly to the bone or lungs.188 Subsequently, follicular carcinoma has a worse prognosis than does papillary carcinoma.188 Follicular carcinomas have higher frequency of RAS mutations than do classical papillary carcinomas, with ˜50% of tumors having activating mutation in RAS present. Another 35% or so are characterized by PAX8/PPARγ gene fusion.189 Of note, RAS mutations are also seen in follicular adenomas and NIFTP and are not considered diagnostic for malignancy.174
Anaplastic thyroid carcinoma is a rare, highly aggressive tumor, accounting for 1% of thyroid malignancies,161 with a propensity to arise in elderly patients with long-standing thyroid disease. Anaplastic carcinoma presents as a rapidly growing mass in the neck, often with airway compromise, and by the time of presentation, is usually unresectable. One-year survival rates are as low as 35%,190 and death is commonly due to local extension.191 Histopathologic evidence of residual differentiated carcinoma suggests that anaplastic carcinomas arise in preexisting papillary or follicular carcinomas.191 This theory is supported by molecular evidence of progressive genetic alterations as tumors advance from differentiated carcinoma to poorly differentiated carcinoma and anaplastic carcinoma.176 Anaplastic carcinomas display a variety of morphologies, from spindled, sarcomatoid cells, to large epithelioid cells, and some cases may show squamoid differentiation. One characteristic feature is a marked tumoral inflammatory response.
Figure 3.10. Follicular carcinoma. The tumor lacks nuclear features diagnostic for papillary carcinoma but shows an invasive growth pattern including invasion through the capsule and into an extracapsular endothelial-lined vascular space (arrowhead).
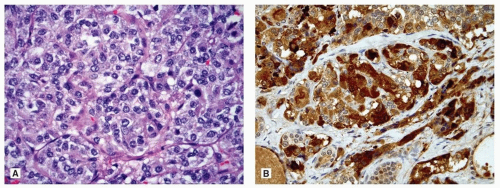
Figure 3.11. Medullary carcinoma of the thyroid. A: Intrathyroidal neoplasm characterized by organoid or cell nest growth pattern, absence of colloid formation, and presence of nuclei with stippled-appearing nuclear chromatin. B: Diffuse calcitonin immunoreactivity confirms the diagnosis; note the absence of calcitonin staining in residual thyroid follicular epithelial cells (lower left).
MTC constitutes about 2% of thyroid malignancies.160 Whereas the majority of cases are sporadic, 20% to 40% are familial medullary thyroid carcinoma (FMTC).192,193,194 Activating RET mutations are found in the majority of cases, with at least 39 different germ-line mutations described in familial cases (MEN 2A, MEN 2B, FMTC).193,195,196 Familial tumors arise in younger patients (peaking in the fourth decade) and tend to be bilateral or associated with multifocal C-cell hyperplasia. Sporadic cases arise in the fifth to seventh decades and are usually solitary. Five-year survival rates approximate 85%.196 Histologically, tumors have classical neuroendocrine appearance with abundant granular cytoplasm and round nuclei with “salt and pepper” stippled chromatin (Fig. 3.11A). Cells may be round, spindled, or plasmacytoid, whereas the stroma is frequently fibrotic and highly vascular. Calcitonin-derived amyloid deposition is a common feature (Fig. 3.11B).
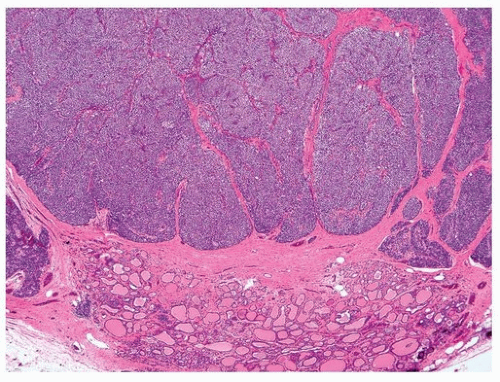
Parathyroid carcinomas are very rare, accounting for <1% of parathyroid tumors.197 Diagnosis requires close communication between the resecting surgeon and diagnosing pathologist. Parathyroid carcinomas produce very high elevations of parathyroid hormone to levels greater than typically seen in cases of hyperplasia or adenoma.198 At the time of surgery, tumors are found to be densely fibrotic and may be difficult to resect from adjacent structures. This fibrotic reaction may be an indicator of invasion of thyroid or skeletal muscle, which, along with lymph-vascular invasion (LVI), are the only reliable histologically diagnostic features of parathyroid carcinoma (Fig. 3.12). In isolation, solid tumor growth, the presence of fibrosis, mitotic activity, and necrosis all suggest malignancy but are usually not adequate to make the diagnosis. Mutations in CDC73 (HRPT2), the gene encoding parafibromin protein, are frequent in both sporadic and familial parathyroid carcinomas.197 Presence of mutation is often reflected in the absence of parafibromin protein, a feature that may be detected by immunohistochemistry. Absence of parafibromin expression in borderline lesions possessing some, but not all of the features of carcinoma (atypical adenomas), may help support a diagnosis of malignancy.199,200 The prognosis of parathyroid carcinomas depends on the success of resection, with lower recurrence rates (˜30%) associated with preoperative diagnosis and complete en bloc resection.197
Figure 3.12. Parathyroid carcinoma. Clinically, the tumor was adherent to the thyroid gland necessitating ipsilateral lobectomy (inferior) and was histologically characterized by the presence of intralesional fibrosis creating a nodular-appearing proliferation extending to the thyroid parenchyma.
Neuroectodemal and Neuroendocrine Malignancies. Neural crest cells migrate throughout the body during development and are thought to be precursors to melanocytic cells, receptor and endocrine cells of perivascular glomus bodies, the olfactory sensory apparatus, and Merkel cells associated with cutaneous mechanoreceptors, among others.
Malignancies arising from sensory apparatuses, including paragangliomas and olfactory neuroblastoma, share similar histologic features with other neural crest-derived tumors such as MTC and pheochromocytoma. Tumors have a nested, highly vascular growth pattern, with balls of neoplastic cells surrounded by S100 protein-positive sustentacular cells. Malignant cells may display a wide spectrum of neuroendocrine differentiation, from bland cells with round nuclei and abundant granular cytoplasm, as in most paragangliomas, to aggressive-appearing small cells with scant cytoplasm, necrosis, and high proliferative index, as in high-grade olfactory neuroblastoma. Most tumors express neuroendocrine markers (e.g., chromogranin, synaptophysin), at least focally and typically lack immunoreactivity with epithelial-related markers (e.g., cytokeratins).
Only gold members can continue reading. Log In or Register to continue