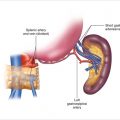
Figure 18.1
Exposure of the body and tail of the pancreas
18.5.1.2 Exposure of the Pancreas (Head and Uncinate)
After gaining access to the peritoneal cavity, the hepatic flexure of the colon is mobilized and reflected inferiorly to expose the head of the pancreas and the duodenum. A complete Kocher maneuver is performed, elevating the head of the pancreas out of the retroperitoneum (Fig. 18.2). To maximize exposure of the pancreas, it is often necessary to divide the right gastroepiploic vein as it enters the superior mesenteric vein. Dividing this vessel connects the dissection of the head with the body and tail allowing for complete exposure of the anterior surface of the pancreas.
Figure 18.2
(a) A Kocher maneuver is performed to elevate the head of the pancreas out of the retroperitoneum. (b) Palpation of the head and uncinate process of the pancreas
18.5.1.3 Mobilization of the Pancreas
Once the pancreas is completely exposed, the peritoneum on the inferior border of the pancreas is sharply incised (Fig. 18.3), and the pancreas is lifted out of the retroperitoneum. Caution should be taken to avoid any injury to the splenic vein, inferior mesenteric vein, or superior mesenteric vein.
Figure 18.3
The peritoneum on the inferior border of the pancreas is sharply incised
18.5.1.4 Bimanual Palpation and Ultrasound
The pancreas can now be palpated bimanually to identify any tumors. Intraoperative ultrasound imaging of the pancreas can be performed (Fig. 18.4) to localize nonvisible lesions and to further assess the relationship of the tumor to the main pancreatic duct. If concern exists that enucleation will result in injury to the main pancreatic duct, a formal pancreatic resection should be considered.
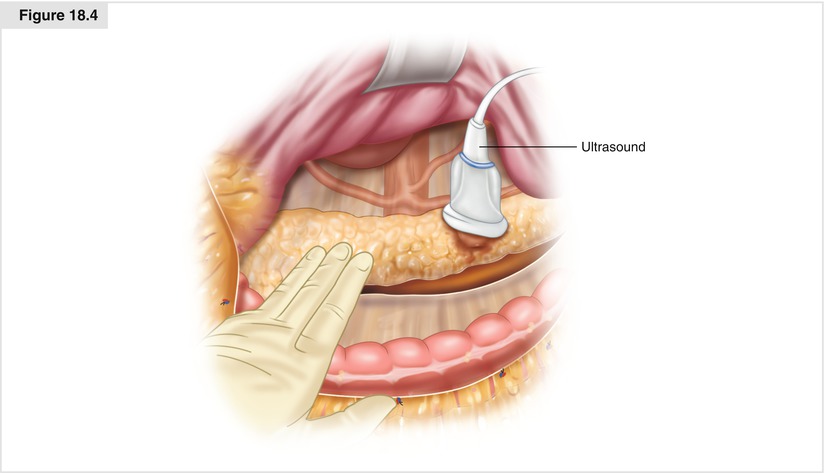
Figure 18.4
Intraoperative ultrasound imaging of the pancreas
18.5.1.5 Enucleation of Pancreatic Tumor
To proceed with enucleation of a deep lesion, the pancreatic parenchyma overlying the tumor should be carefully opened, with small vessels being ligated with fine sutures or cauterized (Fig. 18.5). Most lesions that are amenable to enucleation are on or close to the surface of the pancreas. A combination of sharp and blunt dissection is used to shell the tumor out of the pancreatic parenchyma. Small vessels are controlled with a combination of fine sutures, clips, or an energy device. Dissection is begun at the edges of the lesion and continues with care being taken to stay close to but not entering the tumor.
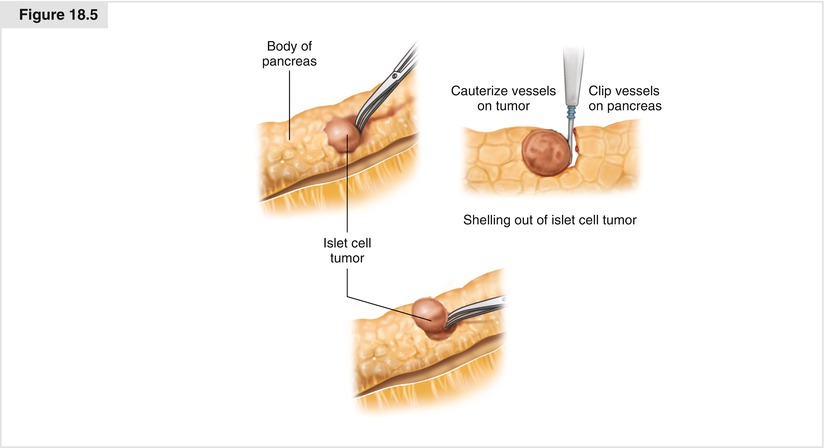
Figure18.5
Shelling out an islet cell tumor from the pancreatic parenchyma
Once the tumor is excised, the bed of the tumor should be carefully examined for any evidence of a major pancreatic duct injury. A closed suction drain should be left near the resection bed.
18.5.2 Laparoscopic Pancreatic Enucleation
18.5.2.1 Positioning and Port Placement
Tumors located in the body or tail of the pancreas or the anterior head of the pancreas may be considered for a laparoscopic approach. For lesions in the head, uncinate, or neck of the pancreas, the patient is positioned supine. For lesions located in the body or tail of the pancreas, the patient is placed in a semilateral (30°–45°) position with the left side up. The surgeon and the camera operator stand on the patient’s right side; the first assistant and the scrub nurse stand on the patient’s left side.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


