Geriatric services have developed rapidly since the inception of the specialty in the 1950s. They have different forms, depending on local resources, experts, and enthusiasts. Every district will offer different services, each with a different spectrum of options. There are some broader national differences within the UK; services in Scotland and Northern Ireland lean more towards rehabilitation and long-term care than those in England and Wales. The following is intended as a generic guide to utilizing geriatric services in the UK. Diversity will limit applicability.
Services for acute problems
Urgent assessment of the acutely unwell patient, where the disease process is new and severe (eg acute MI, stroke) or the deterioration is rapid (eg delirium).
Choosing which is most appropriate will depend on patient characteristics (eg if unstable, then an ambulance to an ED is appropriate; if no change is expected over a few days then urgent outpatient assessment may be used) and local service characteristics (availability of urgent clinic slots etc).
Services for sub-acute problems
Assessment of a patient with a progressive disease process (eg increasing falls, worsening Parkinson’s in a frail patient) or unexplained potentially serious problems (eg iron deficiency anaemia, weight loss) or for diagnosis and management plan (eg cardiac failure).
Again, choice of service will depend on patient factors. Single organ problems can be referred to specialist clinics, less well-defined medical problems to a geriatric outpatients, and problems suggesting the need of multidisciplinary input to the day hospital. Local availability, waiting times and consultant interests will also affect choice—while most cardiologists have chest pain clinics, not all will run heart failure services, which may be provided by general physicians or geriatricians.
Services for chronic problems
This includes active, elective management of slowly progressive conditions by GPs, community teams, specialist nurses, and secondary care physicians (see ‘Chronic disease management’, p.44) and the provision of care for established need.
Allocation of these usually long-term services is generally after an assessment of need and financial status by a care manager.
Most patients will pass through many aspects of this care spectrum with time, and a flexible, reactive service with good communication between providers is essential. The flow diagram (Fig. 2.1) schematically represents possible patient flows through the system.
Fig. 2.1 An example of a comprehensive geriatric service.
Acute services for older people
Since older people present atypically, and are at high risk of serious sequelae of illness, high-quality acute services that fully meet their needs are essential. In any setting, older people have special needs. Their needs, and the consequences of not meeting them, are amplified in the setting of acute illness. Specific areas meriting attention include pressure area care, prevention and treatment of delirium, and optimal nutrition and hydration. Accurate early and comprehensive diagnosis(es) is essential.
An acutely unwell older person may present to one of several services depending on:
Local service provision
The individual’s understanding of the system
Advice from others (eg relatives, health professionals, NHS Direct)
Any service aiming to diagnose acute illness in older people must have access to immediate plain radiography, electrocardiography (ECG), and ‘basic’ blood tests (including prompt results). Specialist clinical assessment (geriatrician, urologist, neurologist, etc.) and more advanced diagnostics (eg ultrasound, computed tomography (CT), magnetic resonance imaging (MRI)) must be available on a prompt referral basis, although may be on another site.
Emergency department (accident and emergency)
Older people present commonly to the ED with falls, fractures, fits, and faints, as well as a broad range of acute surgical and medical problems traditionally referred directly by GPs to surgical or medical teams. Direct referrals of such patients to ED are increasing, as a result of changes in GP out-of-hours services, advice by agencies such as NHS Direct, and changing public behaviour.
▶The ED is potentially inhospitable and dangerous for older people. The environment may be cold, uncomfortable, disorientating, and lacking dignity and privacy. There is a risk of pressure sores developing due to long waits on hard chairs and trolleys. Provision and administration of food and fluid may be neglected, or inappropriately prohibited on medical grounds. A medical model of care may presume serious illness, prioritizing immobility, invasive monitoring and treatments, at the expense of a more holistic approach that appreciates the downside of these interventions. Staff may be experts in emergency medical management, but their expertise in geriatric medicine and nursing is variable. Deadlines and targets that minimize time spent in ED on trolleys (eg the 4hr wait rule) may well benefit older ED users.
Strategies to optimize care for older people in ED might include:
Close liaison with geriatric medical and nursing specialists
Medical and nursing rotation between ED and geriatric medical wards
Focus on optimizing food and fluid provision and pressure care
Provision of alternative modes of admission and assessment, eg Rapid Access Clinic, direct admission to geriatric ward
Provision of specialist geriatric assessment unit
Occupational therapist, physiotherapist, and social worker with expertise in older people based in ED
The older patient in intensive care
With the aging population and a reduction in overt and covert ageism, a greater proportion of intensive care unit (ITU) and high dependence units (HDU) beds are occupied by older patients. However, they remain a rarity with <3% of most ITU admissions in the UK for patients aged >85.
▶Age alone is a weak predictor of outcome and should not be used as the sole reason to deny ITU/HDU care. Frailty scores provide more accurate prognostic information. Patients with multiorgan failure especially in the context of frailty will not do well on ITU.
Older patients with the following should be considered for ITU/HDU:
Postoperative
Septicaemia
Post cardiac arrest/life-threatening arrhythmia
Acute drug effects or overdose
Intensive monitoring eg acute MI or stroke thrombolysis
Ventilatory support, eg pneumonia or pulmonary oedema
If in doubt discuss your case with ITU physicians. Even where patients are unsuitable for admission to ITU, the intensive care specialists and their outreach team may be able to offer advice. The use of early warning scores (EWS) (which are designed to detect patients in pre or periarrest situations) in parallel with escalation/trigger systems (to prompt timely management decisions) is growing. This trend may well increase the involvement of intensivists in the management of critically unwell frail elderly people.
▶Remember that older, frailer patients are more likely to refuse intensive treatment so always enquire, from the patient if possible, or the relatives about any advanced refusal of intensive treatment (see ‘Advance directives’, p.664).
The great integration debate
There has been a longstanding debate among UK geriatricians about the best model of care for older people in hospital. Historically, age-related care grew out of workhouse facilities and the advent of care provided in mainstream institutions was a major step against ageism. The provision of age-related services on the same site and with equal facilities to facilities developed. This defied the label of ageism and professed other advantages. Traditionally care has been divided into either ‘age-related’ or ‘integrated’ but there are many shades of grey in between these two extremes, usually developing locally in response to manpower restraints, ward availability, and the enthusiasm of individuals. The two ‘pure’ systems may be described as follows:
Age-related care. A separate team of admitting doctors to deal with all patients over a certain age (varies—commonly around 75 years) who then care for these patients on designated geriatric wards
Integrated care, In truly integrated care, specialists will all maintain additional generalist skills. These generalists will admit all medical patients regardless of age and continue looking after them on general medical wards, in parallel with specialist clinical commitments
(See Table 2.1 for advantages and disadvantages of each system.)
The debate has never been fuelled by any evidence (there are no studies comparing systems) and it has become less fevered recently as the reduction in junior doctors’ working hours has made it impractical in many hospitals to run two entirely separate teams. As a result various hybrid systems have grown up, managing patients pragmatically and sampling the best aspects of both the systems.
A common compromise is that there is integrated acute assessment, with a single admitting team, but rapid dispersal to the most appropriate service—gastroenterology for a patient with acute gastrointestinal bleed, cardiology for acute MI, and acute geriatric medicine for a confused elderly patient etc. This dispersal may be done at a variety of levels and times, again depending on local service strengths and constraints. Models include triage of need (‘needs’ or ‘function’ related segregation) by an appropriate person immediately after admission (admitting specialist registrar (SpR), experienced nurse, bed-manager, etc.), dispersal by a ward allocation system after removal from the admitting ward or over a period of a few days (by inter-speciality referral) as the special needs become apparent.
As individual systems evolve, the debate recedes and energies are invested into providing the best possible care for all patients through innovation and flexibility within a certain hospital structure, rather than in drawing boundaries and maintaining rigid definitions. Vigilance against ageism in these evolving systems remains essential.
Table 2.1 Comparison of age-related and integrated care
Age-related care
Advantages
Potential drawbacks
All old people seen by doctors with a special interest in their care
Possibility of a two-tier standard of medical care developing, with patients in geriatric medicine settings having lower priority and access to acute investigation and management facilities
All old people looked after on wards where there is a multi-disciplinary team
Less specialist knowledge in those doctors providing day-to-day care
Even apparently straightforward problems in older patients are likely to have social ramifications that are proactively managed
May be stigmatizing for all patients of a certain age to be defined as ‘geriatric’
May be less kudos and respect for geriatric medicine practitioners
Integrated care
Advantages
Potential drawbacks
As the majority of patients coming to the hospital are elderly, it maintains an appropriate skill base and joint responsibility for their care
Many generalists will not be skilled in the management of older patients, so those under their care may not fare as well
There is equal access to all acute investigative and maintenance facilities, as older patients are not labelled as a separate group
Specialist commitments are likely to take priority over the care of older patients
Trainees from all medical specialties will have exposure to and training in geriatric medicine assessment
The multidisciplinary team input is harder to coordinate effectively where the patients are widely dispersed
Sharing of specialist knowledge is more collaborative and informal
Management of the social consequences of disease tends to be reactive (to crisis) rather than proactive
Admission avoidance schemes
Admission avoidance schemes (AAS) are very variable in content and name. Schemes may be divided into those that do and do not offer specialist geriatric assessment (provided by a geriatrician, a GP with a special interest, or a geriatric specialist nurse).
Non-medically based schemes
These may include emergency provision of carers, district nurse, occupational therapy and physiotherapy, delivering, eg, prompt functional assessment and increased care after a fall. As medical assessment is not a part of the scheme, treatable illness may be missed. As a minimum such schemes should incorporate assessments by healthcare professionals who can recognize the need for specialist geriatric assessment and can access such services promptly.
Schemes with a medical assessment
Variously titled Early Assessment, Rapid Assessment, Emergency or Rapid Access clinics
All aim to provide a prompt response to medical need in older people, with acuity falling somewhere between immediate admission and more elective outpatient services
Few schemes aim to provide same-day assessment, most aiming to see patients within 1 week of referral, and at best the next day
There is an assumption that patients are midway between first symptoms and severe disease, and that early intervention may prevent decline, permit less aggressive or invasive treatment, and permit the patient to remain safely at home
Services are best accessed via telephoned, faxed or electronic referral, with prompt assessment of the content of and response to referrals by an experienced professional
▶There is a risk that acutely unwell older people who need emergency assessment or treatment are referred to AAS rather than admitted immediately. If in doubt, admit to the emergency medical/geriatric medicine team. Delirium is an example of a presentation where admission to hospital from home is usually required.
In practice, most AAS do have to admit a modest proportion of patients to hospital directly. In some cases this represents optimal care, but in others it introduces a dangerous delay to a clinical situation
AAS staffing usually includes senior medical staff (± junior support). Experienced nursing assistance is invaluable, perhaps in the form of a nurse practitioner. Nursing roles are variable but may be very extended, to include history taking and physical and mental state examination
Most commonly, AAS are housed in ‘general’ outpatient facilities. Examples of problems managed here include anaemia or breathlessness
A more comprehensive geriatric response (see ‘Comprehensive geriatric assessment’, p.70) is facilitated when AAS is housed in or adjacent to outpatient multidisciplinary services, eg Day Hospital
AAS should have prompt (ideally same day) access to occupational and physiotherapy services, to support the patient at home whilst the effect of medical interventions become apparent. Patients with complex needs are best managed in this environment, eg Parkinson’s disease with on/off periods
Day hospitals
Day hospitals (DHs) provide services that lie somewhere between outpatients and inpatients. Patients stay for half or a full day and the primary aim is to regain or improve independence for a group of frail elderly people with complex needs.
The case mix and interventions vary widely between units but can include:
Medical—new patient assessments, eg for falls, weight loss, anaemia, as well as chronic disease management, eg heart failure, parkinsonism
Nursing—eg pressure sore and leg ulcer treatment
Physiotherapy—eg following stroke, fracture, surgery
Occupational therapy
Diagnostics—facilities for usual blood tests, radiology, et. and also specific therapeutic trials, eg levodopa
A flexible and holistic attitude is required and many DH clients will take advantage of multiple different services in a ‘one-stop-shop’ approach. There is usually a mixture of new patient assessments, rehabilitation, and chronic disease management. Patients may be referred directly from the community or from other outpatient settings or may be booked for a follow-up after an inpatient stay. Some units have designated sessions for specific patient types or services (eg movement disorder clinic, admission avoidance clinic). Multidisciplinary teamwork and comprehensive geriatric assessment (see ‘Comprehensive geriatric assessment’, p.70) and functional goal setting are all important tools.
History and evolution
The first DHs were set up in 1960s. In their heyday many units had collected a huge number of patients who were very frail but had little active intervention and used their visits as social occasions or respite for carers. Unacceptably long waiting lists hindered efficient running in some units. Transport problems often proved to be a weak point, with patients spending lengthy periods of time waiting for, or during transport.
The monitoring/supporting role has now been largely taken over by day centres (see ‘Other services’, p.42) and modern DHs tend to have a high ratio of new:old patients and a rapid turnover. Increasing pressure on acute hospitals has opened up the role of rapid access admission avoidance clinics and early supported discharge schemes. Intermediate services development, following the national service framework (NSF), has sometimes augmented services (eg falls services) and sometimes denuded them (eg where outreach services have taken over).
Cost effectiveness
Pressures to justify the expense of day hospital places led to a flurry of publications looking at effectiveness and cost-effectiveness. While this area remains controversial a systematic review in 2008 found that DH patients did have less functional deterioration, lower rates of institutionalization and hospital admission than control groups receiving no care. However DHs did not prove superior to other comprehensive care services (eg domiciliary rehabilitation). DH care is costly but this may be offset by decreased inpatient bed usage and institutionalization or social care costs. It is very important to ensure this expensive resource is targeted effectively and regularly evaluated to ensure cost-efficiency.
Further reading
Forster A, Young J, Lambley R, Langhorne P. (2008). Medical day hospital care for the elderly versus alternative forms of care. Cochrane Database Systematic Review4: CD001730.
Specialty clinics
Every region will have different resources, but most will have some specialty clinics run by geriatricians, by other specialists, or occasionally combined clinics run by more than one specialty. Examples of clinics are shown in Table 2.2. The advantages of specialty clinics are many:
Usually simple referral protocol
Concentration of expertise
Increased training opportunity for juniors
Often specialist nursing staff
Increased patient education and awareness of the condition—through meeting others with the same diagnosis, through the work of specialist nurses and through the availability of information leaflets
May utilize a rapid access investigation slot on a regular basis (eg carotid Doppler ultrasound in transient ischaemic attack (TIA) clinics)
Increased use of protocols (may improve quality of care)
Often rapid turnover
Where the same clinic is offered by different specialties, or where you are unsure if a referral to a geriatrician or an organ specialist is most appropriate, ask the following:
Is this a new or urgent problem? There are an increasing number of clinics with a protocol-defined maximum waiting time for the urgent assessment of patients. These may prevent admissions and allow rapid outpatient management of many conditions (eg TIA, chest pain, possible malignancy) but are prone to being overwhelmed with referrals thereby rendering them less responsive to the needs of the truly urgent cases. Non-urgent cases should be referred to standard outpatient clinics
Is the diagnosis likely to be clear-cut? A fit patient with cardiac sounding chest pain should go to a cardiology-run clinic, as they will have the fastest access to the appropriate expertise and investigations. If the pain is more nebulous, then waiting for a chest pain clinic appointment only to be given the diagnosis ‘non-cardiac chest pain’ is unhelpful. Such a patient is better seen in a more general (usually geriatric) clinic
Does this patient have a single problem? If so, then they are likely to do well in a clinic run by an organ specialist. If, however, they are frail, with multiple pathologies then a geriatric clinic may be better. Here there is time to for example, undress the patient properly, and assess them fully as the allocation time per new patient is likely to be longer. There is also less likely to be a protocol driven response to a single problem without looking at the wider picture (eg prescription of multiple medications for angina in a patient prone to falls)
Is this patient already attending a geriatric clinic for follow-up? If so, most new problems can be addressed by that team rather than referring to another specialty
Upper gastrointestinal bleeding/query other gastrointestinal malignancy
Gastroenterologist
Breast lump
Breast surgeon
Leg ulcers
Dermatologist
Geriatrician
Falls/syncope
Geriatrician
Memory
Geriatrician
Psychogeriatrician
Neurologist
Intermediate care
There is no universally acknowledged definition of ‘intermediate care’. It is used to describe almost any sort of care which lies between an acute inpatient stay and usual primary care. The term first came into general use in 2001 after the NSF described it as a major strategy for improving healthcare and the UK government promised to invest £900 million over 5 years to implement it. In many instances this led to a re-badging of existing services but there were also an assortment of new and often innovative approaches.
While many geriatricians welcomed the emphasis on non-hospital-based geriatric medicine others have warned against intermediate care being a covert form of ageism which allows rationing of acute hospital medicine in favour of less expensive and often less effective care.
Only gold members can continue reading. Log In or Register to continue
 ‘Primary care’, p.46)
‘Primary care’, p.46) ‘Acute services for older people’, p.16)
‘Acute services for older people’, p.16) ‘Admission avoidance schemes’, p.20)
‘Admission avoidance schemes’, p.20) ‘HOW TO … Do a domiciliary visit’, p.33)
‘HOW TO … Do a domiciliary visit’, p.33) ‘Specialty clinics’, p.24)
‘Specialty clinics’, p.24) ‘Day hospitals’, p.22)
‘Day hospitals’, p.22) ‘Intermediate care’, p.26)
‘Intermediate care’, p.26) ‘HOW TO … Do a domiciliary visit’, p.33)
‘HOW TO … Do a domiciliary visit’, p.33) ‘Chronic disease management’, p.44) and the provision of care for established need.
‘Chronic disease management’, p.44) and the provision of care for established need. ‘Informal carers’, p.40)
‘Informal carers’, p.40) ‘Home care’, p.38)
‘Home care’, p.38) ‘Other services’, p.42)
‘Other services’, p.42) ‘Care homes’, p.34)
‘Care homes’, p.34)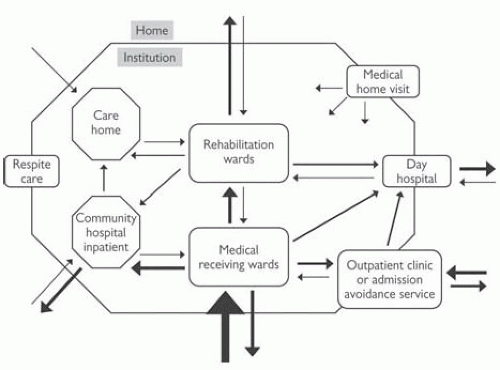
 ‘Advance directives’, p.664).
‘Advance directives’, p.664). ‘Comprehensive geriatric assessment’, p.70) is facilitated when AAS is housed in or adjacent to outpatient multidisciplinary services, eg Day Hospital
‘Comprehensive geriatric assessment’, p.70) is facilitated when AAS is housed in or adjacent to outpatient multidisciplinary services, eg Day Hospital ‘Comprehensive geriatric assessment’, p.70) and functional goal setting are all important tools.
‘Comprehensive geriatric assessment’, p.70) and functional goal setting are all important tools. ‘Other services’, p.42) and modern DHs tend to have a high ratio of new:old patients and a rapid turnover. Increasing pressure on acute hospitals has opened up the role of rapid access admission avoidance clinics and early supported discharge schemes. Intermediate services development, following the national service framework (NSF), has sometimes augmented services (eg falls services) and sometimes denuded them (eg where outreach services have taken over).
‘Other services’, p.42) and modern DHs tend to have a high ratio of new:old patients and a rapid turnover. Increasing pressure on acute hospitals has opened up the role of rapid access admission avoidance clinics and early supported discharge schemes. Intermediate services development, following the national service framework (NSF), has sometimes augmented services (eg falls services) and sometimes denuded them (eg where outreach services have taken over).


