Chapter 2 NORMAL, HEALTHY AND SUCCESSFUL AGEING
INTRODUCTION
This chapter introduces the concept of normal ageing and contrasts it with healthy ageing and successful ageing. Mental health workers regularly encounter unhealthy ageing, so it is useful to have a clear idea of normal ageing and successful ageing. The concepts of brain reserve and the clinician’s illusion are also described.
NORMAL AGEING
Normative or normal ageing involves adapting to declining physical health, dealing with life transitions and coping with loss and grief. Many older people do this without difficulty. The Australian Institute of Health and Welfare (AIHW) produces regular statistical overviews of the characteristics of older Australians (Australian Institute of Health and Welfare 2007) and many of the statistics in this chapter are derived from this source. Approximately two-thirds (67.3%) of older Australians rate their general health as good or better, whereas one-third (32.7%) rate their health as fair or poor (Australian Institute of Health and Welfare 2007). Despite these optimistic self-ratings, the majority of older Australians do have one or more chronic health problems. These include high blood pressure (71.8%), high cholesterol (61.8%), impaired glucose tolerance (22.1%) and obesity (20.1%). Other big health issues in normal ageing include osteoarthritis, impaired eyesight due to cataracts and macular degeneration, impaired hearing, and poor dental health due to lack of universal access to dental care.
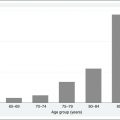
Not surprisingly, older people have more than twice the rate of visits to their general practitioners as younger adults (Australian Institute of Health and Welfare 2007). In 2005–06, this amounted to 8.6 visits per year for people aged 65 years and over compared with about 4 per year for people under 65 years of age. While the majority of older people do not have cognitive impairment or a serious mental health problem, anxiety and depressive symptoms are quite common. In 2004–05, 3.2% of people aged 65 years and over reported very high levels of psychological distress and 7.7% reported high levels of psychological distress on a standardised self-report measure.
Life transitions are common in later life. Some older people are fortunate to be able to continue working beyond the normal retirement age in an occupation that they find enjoyable and fulfilling. More commonly, however, retirement comes at the usual time, if not earlier than expected, due to poor health or prevailing economic conditions. The majority of older people have had children and by the time of their retirement from the paid workforce also have grandchildren. In well-functioning families, grandparents are likely to be happily involved in helping their adult children care for their children. In less fortunate families, grandparents will need to substitute for absent or dysfunctional parents. Some older couples might be able to coordinate their other roles sufficiently to become what are termed ‘grey nomads’ in Australia or ‘snow birds’ in Canada and the United States (Higgs & Quirk 2007). Grey nomads travel around the country, often congregating in camping grounds and caravan parks in picturesque locations. They commonly drive campervans or tow caravans. Some older couples do this for part of the year, whereas others have no permanent residence and travel for the whole year. There is often a preference for warmer climates and outdoor activities.
Loss and grief are normal accompaniments of the human condition, but are more commonly experienced in later life. Among Australians aged 65 years and over, 71.3% of men and 44.6% of women are married, whereas 12.3% of men and 42.1% of women are widowed. Largely as a consequence of spousal bereavement, 29% of older Australians live alone (Australian Institute of Health and Welfare 2007). Spousal bereavement is associated with a temporary rise in symptoms of anxiety and depression, and occasionally with mental health problems requiring treatment.
Regular physical activity is undertaken by 49% of older Australians. Walking is most popular, with 29.1% of those aged 65 years and over walking on a regular basis. Other popular types of physical activity include lawn bowls (5.6%), golf (5.4%), aerobics or similar classes (5.4%), swimming (4.2%) and cycling (1.7%) (Australian Institute of Health and Welfare 2007). Reported physical activity varies by self-rated general health status. Over 60% of older people who rated their health as excellent participate in sport or physical activity, while only about 20% of older people who rate their health as poor do so (Australian Bureau of Statistics 2006).
There is clearly some room for increased participation in regular physical activity by older people. Importantly, there is now evidence that regular physical exercise is not only good for physical health and longevity, but also for cognitive function. Epidemiological evidence indicates that men who walk at least 3 kilometres per day reduce their risk of dementia by almost one-half compared with sedentary men (Abbott et al 2004), and experimental evidence indicates that walking for 50 minutes three times a week significantly improves cognition (Lautenschlager et al 2008). In laboratory studies on rodents, voluntary physical exercise has been found to be associated with increased neurogenesis (production of new brain cells) and it is possible that the same might be true in humans.
The availability of good social support and social networks seems to improve the resilience of older people, just as it does young and middle-aged people. Older people tend to prune their social networks so that they are smaller and more focused on supplying their needs. However, normal older people generally perceive their social networks to be adequate. Perhaps surprisingly, social networks seem also to modify the effect of brain pathology on the risk of cognitive decline (Bennett et al 2006). In other words, older people with good social networks seem somehow able to tolerate more brain pathology before developing clinical signs of cognitive impairment or dementia. Older people are increasingly using the internet to stay in touch with friends and relatives. In 2004–05, 20% of older people used a computer at home, with the majority having internet access. This will rise dramatically over the next few years, as 51% of those aged 55–64 used a computer at home in 2004–05 (Australian Institute of Health and Welfare 2007).
Access to transport is a key requirement in later life. Of older people residing in the major Australian cities in 2006, 84.4% of men and 52.2% of women had access to a motor vehicle they could drive (Australian Institute of Health and Welfare 2007). The proportions were even higher in provincial cities and rural areas. Older people without cognitive impairment and those with insight into mild cognitive impairment generally modify their driving behaviour as their driving skill changes (Pachana & Petriwskyj 2006). For instance, older people often restrict their driving to good conditions and daylight hours. Despite these self-imposed changes in driving behaviour, older people are overrepresented in motor vehicle accident statistics. This may be because many older people tend to drive short distances and most accidents occur close to home.
Two factors that are commonly associated with unhealthy ageing are features of normal ageing for some people. Although modest regular alcohol consumption might be associated with reduced risk for some cardiovascular outcomes, 8.1% of older Australians engage in a risky level of alcohol intake. In addition, 7.9% of older people smoked cigarettes in 2004–05 (Australian Institute of Health and Welfare 2007). Smoking is one of the most important modifiable risk factors for cardiovascular disease, stroke and cancer.
The role of work in later life is coming under greater scrutiny as an increasing proportion of the workforce is over the age of 55 years. These trends are affecting health workers also. In 2006, 20.6% of male health workers and 14.6% of female health workers were aged 55 years or over (Australian Institute of Health and Welfare 2009). In recognition of better health and increased longevity, governments in developed nations around the world are pushing back the conventional retirement age to beyond 65 years. People in jobs that are not physically demanding and in jobs where excellent health is not a requirement may elect to work beyond the conventional retirement age, particularly if the public contribution to pensions declines, as seems inevitable. Workers in physically demanding jobs (e.g. the building trades and underground mining) and workers in jobs that demand excellent health (e.g. airline pilots and professional athletes) may need to seek employment in less physically demanding fields in later life. Unless birth or immigration rates increase dramatically, there will be relatively fewer working-age people to support older people, and one consequence of this is that older people will need to continue working longer.
One issue that is related to healthy and successful ageing is whether employers will be prepared to allow older workers to work reduced hours so that they can manage their transition to retirement in a graduated fashion. In the 2006 Australian census, 48% of full-time workers indicated that they intended to work part time before retiring from the workforce. Interestingly, 24% of employed people indicated that they intended to retire at 70 years or over.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


