Fig. 9.1
18F-FACBC positive bone metastases in high-risk prostate cancer at staging evaluation. A 71-year-old patient diagnosed with high-risk prostate cancer (PSA 6.8 ng/ml; cT2; GS 4 + 4) underwent the standard staging flow chart and was scheduled for radical surgery. He was enrolled in a prospective study for staging lymph nodes with 18F-FACBC PET/CT. The experimental compound showed increased focal uptake in a single osteosclerotic lesion in the right iliac bone in keeping with bone metastasis. The detection of distant secondary lesions leads to an exclusion from surgery procedure and a change in treatment management. Project granted by “Programma di ricerca Regione-Università 2013, Regione Emilia Romagna, Area 1- Bando Giovani ricercatori Alessandro Liberati”
Recently, Nanni et al. compared the accuracy of 18F-FACBC and 11C-choline PET/CT in 89 pts, consecutively and prospectively enrolled, with BCR after RP, 11C-choline and 18F-FACBC PET/CT performed within 1 week and off ADT at the time of the scans. PET positivity criterion was the presence of abnormal focal areas of uptake, more intense than background, and a semiquantitative SUV ratio (SUVmax in the lesion/SUVmean in surrounding background) ≥1.5 was used to aid the visual analysis. Different from the Emory group, they considered as background not the marrow but the healthy tissues surrounding the focal pathological uptake, wherever it was. Considering only the bone region analysis, overall seven patients resulted positive with at least one of the two tracers. Four patients were equally positive (TP) at the two tracers (lesion appearances in corresponding low-dose CT images were no evidence of bone remodelling in 2 pts, degenerative-like in one patient, multiple small osteosclerotic in one patient). Two patients were positive at choline (1FP, 1TP) but negative at FACBC (1TN, 1FN) in osteosclerotic lesions (Fig. 9.2).
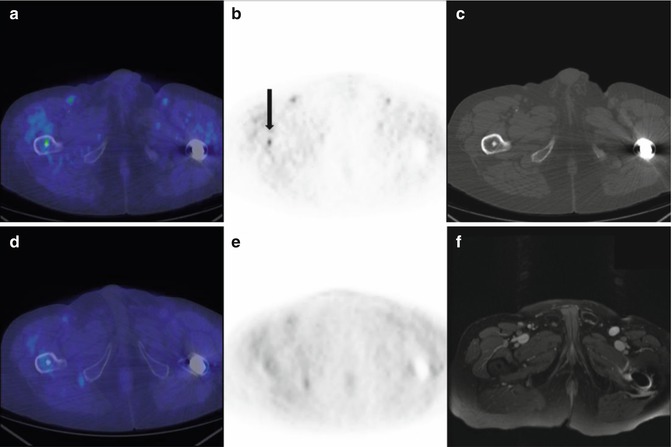
Fig. 9.2
False-positive 11C-choline and true-negative 18F-FACBC benign bone island, confirmed by MRI. A 74-year-old-patient radically treated for prostate cancer presenting with biochemical recurrence (PSA 1.57 ng/ml, PSA doubling time (dt) 16.4 months, PSA velocity 0.7 ng/ml/year). 11C-choline PET/CT showed focal increased uptake in the right femur (a axial fused choline PET/CT; b axial choline PET; see black arrow), corresponding with a subcentimetric osteosclerotic lesion in low-dose CT images (c). The bone finding resulted non-avid with 18F-FACBC, performed within 1 week (d axial fused FACBC PET/CT; e axial FACBC PET). A dedicated MRI (f axial T2 fatsat) and the subsequent clinical follow-up excluded bone relapse defining the lesion as benign bone island. Project granted by “Programma di ricerca Regione-Università 2010–2012, Regione Emilia Romagna, Bando Giovani Ricercatori”
One patient was negative at choline (FN) but positive at FACBC (TP) in a lesion that could be misinterpreted for its degenerative-like aspect. Standard of reference was clinical evaluation and imaging in all cases (i.e. bone scan, MRI, follow-up 11C-choline PET/CT). Among the 82 patients who presented a concordant negative test with both compounds, at least four turned out FN at clinical evaluation and imaging (two CT images, one follow-up 11C-choline PET/CT, one bone scan + MRI both depicting a lesion in the tibia outside the PET field of view). At least 32 pts turned out disease-free for bone involvement (TN); reference standard was PSA drop after target treatment on prostate bed or lymph nodes (i.e. RT prostate bed and/or ln; lymphadenectomy) or imaging (negative for bone metastases but positive for local relapse or nodal involvement or other site dissemination) in most cases and a clinical evaluation in two cases. The remaining 46 were actually indeterminate TN or FN because of insufficient evidences at follow-up data [1, 16, 17].
Kairemo et al. in a cohort of 26 patients concluded that 18F-FACBC may play a role for restaging prostate cancer, especially in patients with a fast PSAdt. In particular, 26 (44.8 %) metabolically active lesions were reported in the skeleton [18]. Data about staging primary prostate cancer come from a Japanese multicenter phase IIb clinical trial with NMK36, trans-1-amino-318F-FACBC, by Suzuki et al. In their population (radical prostatectomy cohort, 42 patients; hormone therapy cohort, 24 patients), the concordance rate and k coefficient for diagnosis of bone metastasis by NMK36-PET/CT and combined conventional exams (bone scan and whole-body contrast-enhanced CT) were 83.3 % and 0.557, respectively. These results showed moderate concordance, and seven subjects were positive only with NMK36-PET/CT suggesting that the experimental compound might visualise early stage of bone metastases [19].
Few limitations should be considered when approaching 18F-FACBC in this limited topic: the low intrinsic spatial resolution makes PET not suitable for the detection of bone micrometastases; the majority of population investigated so far are often small, clinically heterogeneous and with a limited number of positive findings; the reference standard is mainly based on a longitudinal follow-up because bone biopsy is rarely feasible; treatment decisions are often undertaken without a matching imaging or reliable biopsy, which makes it difficult to determine if and where exactly the metastases were present; and of the absence of validation for most of negative PET scans (TN or FN actually remains indeterminate) [17].
9.3 Role of 68GA-PSMA PET/CT for Detecting of Bone Metastases in Prostate Cancer
A new molecular probe targeting PSMA has been recently developed [20]. PSMA is a membrane-bound enzyme with significantly elevated expression in prostate cancer cells in comparison to benign prostatic tissue [21]. The localisation of the catalytic site of PSMA in the extracellular domain allowed for the development of small specific inhibitors that are internalised after ligand binding [21]. Preliminary studies demonstrated that 68Ga-PSMA (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBED-CC)]), an extracellular PSMA inhibitor for PET/CT imaging, is characterised by a significantly higher accuracy in the detection of early recurrence as compared to 18F-choline PET/CT [2, 22]. These investigations also reported a higher tumour-to-background ratio for 68Ga-PSMA PET/CT for the detection of suspected prostate cancer metastases when compared to 18F-choline PET/CT [22] and very promising performances also at very low PSA levels [2, 23]. In Fig. 9.3, an example of a patient with bone metastasis at 68Ga-PSMA and 11C-choline PET/CT is reported.
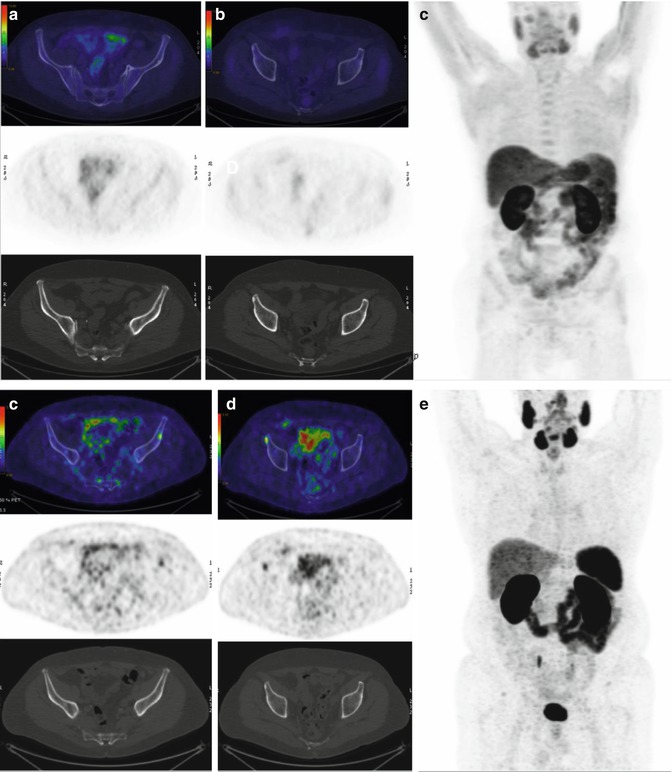
Fig. 9.3
F.P. is a 68-year-old patient treated with RP for PCa, GS 4 + 3, T2cN0(0/22)MxR0 in 20/7/2012. No adjuvant therapies have been performed after RP. In February 2015, the patient was addressed to salvage radiotherapy on the prostatic bed for biochemical relapse. PSA nadir after salvage therapy was 0.01 ng/mL. On June 2015, patient experienced a biochemical failure with PSA = 0.24 ng/mL and was referred in March 2016 to choline PET/CT which resulted negative (a–c) (PSA = 0.73 ng/mL). As a consequence, the patient was investigated with 68Ga-PSMA PET/CT that showed the presence of two bone osteoblastic lesions. According to 68Ga-PSMA PET/CT results, the patient was addressed to androgen deprivation therapy
Despite these promising results, the results obtained by 68Ga-PSMA PET/CT in recurrent prostate cancer have not been extensively validated with either histology (namely, biopsy of the suspicious metastatic site) or with lesion-directed imaging provided with high specificity [24]. More specifically literature lacks studies specifically aimed to evaluate the accuracy of PSMA PET/CT for investigating bone metastatic disease. In the largest patient series published so far, however [25], Afshar-Oromieh and colleagues evaluated the role of 68Ga-PSMA PET/CT in a cohort of 319 recurrent prostate cancer patients. Despite inhomogeneous characteristics in the population (mean PSA 161 ng/mL; median PSA 4.59 ng/mL; 28 patients not treated with radical therapies), authors assessed an overall positivity rate of 82.8 %. A total of 901 lesions were assessed by 68Ga-PSMA PET/CT and considered suspicious for malignancy, with a mean per-lesion SUVmax of 13.4 (±14.6). According to the published data, on a per-lesion analysis, bone lesions were observed in the 39.8 % of cases (359 out of 901 lesions observed) with a mean per-lesion SUVmax value of 14.3 (±14.0). This data suggests the good value of this new imaging procedure for evaluating a possible skeletal involvement in recurrent prostate cancer patients. In particular, in this large cohort of patients, a high tumour-to-background ratio (TBR) for 68Ga-PSMA PET/CT allowing a proper visualisation of the suspected lesions was confirmed. Eiber et al. [26] later confirmed these results. In a cohort of 248 recurrent patients, the authors observed an overall positivity rate of 89.5 % for 68Ga-PSMA PET/CT. On a per-patient analysis, bone lesions were documented in the 35.9 % of patients (89 out of 248 patients). In particular, in the data reported by authors, in the 10.1 % of these 89 patients, the bone metastases were exclusively identified with PSMA focal uptake in the bone marrow, without any morphological alterations in CT. Thus, according to these results, in this patient series, with median PSA of 1.99 ng/mL, in the 3.7 % of the overall population, bone marrow metastases were suspected. Recently, Ceci et al. [23] investigated the role of 68Ga-PSMA PET/CT for restaging prostate cancer patients and evaluated which clinical and pathological features were associated with PET/CT positivity rate. In their patient series (mean/median PSA 3.5/1.7 ng/mL), positive bone lesions were observed in the 17.1 % of the overall population (12 out of 70). On a per-lesion analysis, bone lesions were observed in the 14.5 % of the 152 positive lesions analysed with a mean/median SUVmax of 16.1/10.9 (range 4.2–33.7). It is interesting to report that according to data not published in this article (reported as courtesy of the authors), in the 12 patients with positive bone lesions, the mean/median PSA values observed were relatively low (mean/median PSA 4.3/1.3 ng/mL). Furthermore, these patients showed fast PSA kinetics (mean PSA doubling time 3.5 months). This data is in accordance with the statistical analysis presented by the authors, in which PSAdt was a significant predictor of the detection of distant lesions, including bone metastases (p = 0.011).
A prospective comparative study between 18F-fluoromethylcholine (CHO) and 68Ga-PSMA PET/CT (PSMA) was performed on 38 patients in early 2015. The study specifically addressed patients in the low and very low PSA area, also remarking possible changes in clinical management of these patients. The study confirmed a major detection rate for PSMA over CHO regardless of the PSA level. Within this patient cohort, a total of 16 bone lesions were identified by PSMA (Fig. 9.4) (CHO identified 9 lesions; this data was not published in this article and is reported as courtesy of the authors).