Neuropathic pain is a result of dysfunction, either in peripheral nerves or in the central processing within the spinal cord and brain. It is possible to categorize neuropathic pains on the basis of underlying pathology, the region of the nervous system that is affected, and the individual patient’s responses to the pain syndrome. It is common to find alterations in sensation in the sensory territory of damaged nerves or their central projection pathways. Neuropathic pains have many etiologies, including tumors compressing or invading nerves, surgical trauma of nerves, inflammation of nerves, neurotoxins, endocrinological disorders affecting nerve function, vascular compromise of peripheral (PNS) or central (CNS) nervous system structures, and viral infection of the nervous system. Neuropathic pains are often characterized by the paradoxical combination of sensory loss, perversions of sensation, and pain in a defined region of the body. Common causes of neuropathic pain in the cancer patient include compression or infiltration of nerves by tumor, nerve trauma secondary to diagnostic or surgical procedures, and nervous system (including spinal cord) injury following treatments such as chemotherapy or radiation.1
Neuropathic pain is characterized by both positive and negative symptoms.2 Positive symptoms include spontaneous pain, paresthesia, dysesthesia, after-sensations, and abnormal temporal and spatial summation, as well as a pain evoked by normally innocuous stimuli (allodynia) and an exaggerated or prolonged pain to noxious stimuli (hyperalgesia or hyperpathia). The negative symptoms reflect either the loss of sensation due to axonal or neuronal death or, alternatively, central inhibition. The positive symptoms reflect abnormal excitability within the nervous system. Neuropathic pain may be reported as burning or lancinating. These abnormal sensory phenomena can be further characterized as elicited by static or dynamic stimuli. A distinction should be made between stimulusevoked pain and spontaneous (stimulus-independent) pain, which may have different underlying mechanisms. Spontaneous pain can be either constant or intermittent (even paroxysmal), and most patients describe having both (eg, constant “burning” pain plus intermittent pain that is “shooting” or “electric shock-like”). In addition, spontaneous paresthesias and dysesthesias may manifest as abnormal sensations, including crawling, numbness, itching, and tingling.
Patients may have sensory deficits with one modality, such as pinprick sensitivity, and hyperalgesia to another, such as light touch, both in the same nerve distribution.3 Dynamic mechanical allodynia can be elicited by lightly rubbing or brushing the skin with a cotton swab or brush; static mechanical allodynia can be provoked by blunt pressure with a finger; and thermal allodynia can be assessed with a warm or cool tuning fork. An increased sensation of pain in response to a normally painful stimulus is termed hyperalgesia, which can be assessed using painful thermal (cold or heat) or punctate (eg, pinprick) stimuli. Painful summation and wind-up to repeated stimuli, especially when the initial sensation is reduced, is important evidence of abnormal sensory processing. Diagnosing neuropathic pain can be difficult, as it may occur in conjunction with pains of other etiology, as seen in the patient with low back and leg pain secondary to spondylolisthesis. Furthermore, there may be a significant neuropathic component from nerve root injury, but mechanical instability or secondary myofascial pain can mask this component.
The majority of research into neuropathic pain mechanisms has concentrated on changes in the peripheral nerve or spinal cord after peripheral nerve injury and, therefore, most available evidence relates to changes in these parts of the nervous system.4 Nevertheless, it is important to recognize that alterations in the brain have also been demonstrated following peripheral nerve injury, but much less is known about the significance of these changes. For example, phantom limb pain has been shown to be associated with reorganization of the cortex of humans.5 Also, lesions exclusively in the CNS, such as a stroke involving the lateral thalamus, can produce a neuropathic pain syndrome.
Nerve fibers can develop abnormal ectopic excitability at or near a site of injury. The mechanisms include unusual distributions of Na+ channels, as well as abnormal responses to endogenous algogenic substances and cytokines such as tumor necrosis factor α (TNF-α).6 Injury anywhere in a peripheral nerve produces changes in the associated dorsal root ganglion cells and the dorsal horn neurons which the peripheral axons project upon. The spread of pathophysiology includes upregulation of nitric oxide synthase in axotomized neurons, deafferentation hypersensitivity of spinal neurons following afferent cell death, long-term potentiation of spinal synaptic transmission, and attenuation of central pain inhibitory mechanisms. Repeated or prolonged noxious stimulation and the persistent abnormal input following nerve injury activate a number of intracellular second messenger systems. Although these processes of increasing nervous system excitability may be considered a strategy to compensate for functional deficits following nerve injury, the result is widespread nervous system sensitization resulting in pain and hyperalgesia.
Another sequel of nerve injury or disease such as virus attack is apoptosis of neurons in the PNS and CNS. Apoptosis appears to induce neuronal sensitization and loss of inhibitory systems, and these potentially irreversible processes might underlie both nervous system damage by brain trauma or ischemia as well as neuropathic pain.6 Factors contributing to central sensitization and disinhibition of pain pathways (and thus, central pain) include gain in neuronal excitability, loss of inhibition, and increased facilitation.7 Activated microglia (usually as a consequence of an inflammatory process) appear to maintain neuronal hyperexcitability in the spinal cord dorsal horn through an extracellular signal-regulated kinase-regulated PGE2 signaling mechanism.8
The CNS adapts to both PNS and CNS injury, sometimes in beneficial ways, but also with reorganization that can be maladaptive.9 Advances in functional imaging techniques have resulted in significant improvements in our knowledge of brain function. Modern neuroimaging methods include positron-emission tomography (PET), functional magnetic resonance imaging (fMRI) and magnetoencephalography (MEG). The primary use of MEG is the measurement of time courses of activity of neuronal function and to pinpoint sources in primary auditory, somatosensory, and motor areas in creating functional maps. PET and fMRI have been used to determine whether different neuropathic pain symptoms involve similar brain structures and whether these structures are related to the physiological “pain matrix.”10 PET can be used as a measure of local brain activity by using radionuclides to produce maps representing changes in cerebral blood flow. PET has been applied to investigate the neural substrates involved in pain processing and perception in human subjects.11
PET studies have suggested that spontaneous neuropathic pain is associated principally with changes in thalamic activity and the medial pain system, which is preferentially involved in the emotional dimension of pain.12 Also, in patients with neuropathic pain, PET imaging of regional blood flow demonstrated that activity in the cortical network involved in the sensory-discriminative processing of nociceptive pain is increased in neuropathic pain, whereas decreased activity occurs in the orbitofrontal and insular cortices.13 fMRI has demonstrated new regions of the brain involved in pain processing such as the nucleus of the solitary tract.14 In patients with neuropathic pain, fMRI was used to determine different brain regions involved in response to allodynic stimuli.15 Both PET and fMRI have been used to investigate the basis of allodynia. The results obtained have been very variable, probably reflecting the heterogeneity of patients in terms of etiology, lesion topography, symptoms and stimulation procedures. Functional neuroimaging may someday play a role in the diagnosis and evaluation of chronic pain. Today, they are used more in research than in our clinical practice.
The neuropathic pain scale (NPS) was developed to assess distinct qualities associated with neuropathic pain and is sensitive to measuring outcomes for a variety of therapeutic interventions.16 The NPS is valid and reliable in the assessment of central pain associated with multiple sclerosis17 and is currently considered the most valid as a measure of therapeutic outcome of eight available tools used in the assessment of neuropathic pain.18 The NPS appears to be able to discriminate between neuropathic and nonneuropathic pain,19 although some authors question this ability.20 The Pain Quality Assessment Scale is a tool that includes the NPS items and may prove to be even more useful in the assessment of neuropathic pain because it includes pain descriptors common to people with neuropathic and other chronic pain conditions not included on the NPS.18Appendix M lists the Neuropathic Pain Scale.
Bedside examination of the patient should include quantification and mapping of motor, sensory, and autonomic abnormalities, if present. Touch (Aβ fibers) may be assessed using cotton wool and a tuning fork may be used for vibration sense (Aβ fibers). A wooden cocktail stick may be used for assessment of pinprick and sharp pain (Aδ fibers). Thermal sense (C fibers) may be evaluated by metal thermorollers or by using a tuning fork that can be heated or cooled using tap water. Quantitative sensory testing (QST) is helpful to quantify the effects of treatments on allodynia and hyperalgesia and may reveal a differential efficacy of treatments on different pain components. However, QST is time consuming and difficult to use in clinical practice. Standard neurophysiologic responses to electrical stimuli, such as nerve conduction studies and somatosensory-evoked potentials, are useful to demonstrate, locate, and quantify damage along the peripheral or central sensory pathways. These measures do not assess function of nociceptive pathways and have no bearing upon the presence or absence of pain.
The following common cancer pain syndromes present with a major neuropathic component.
NEUROPATHIC PAIN SECONDARY TO CRANIAL NEUROPATHIES
Painful cranial neuralgias can arise from base of skull metastases, leptomeningeal metastases, or head and neck cancers.21 Several well-described pain syndromes are seen with skull base metastases22 and most often occur with primary tumors of the breast, lung, and prostate. Constant aching pain in the region of the bone destruction and progressive cranial nerve palsies are the principal manifestations.
The cavernous sinus consists of a venous plexus, the carotid artery, cranial nerves, and sympathetic axons. Cavernous sinus syndrome (CSS) is caused by multiple etiologies, and MRI is the most sensitive tool for diagnosis.23 The syndrome is characterized by multiple cranial neuropathies. The clinical presentation includes impairment of ocular motor nerves, Horner syndrome, and sensory loss of the 1st or 2nd divisions of the trigeminal nerve in various combinations. The pupil may be involved or spared. Various degrees of pain including painful opthalmoplegia may occur dependent on the particular cranial nerve involved. Tumors are a frequent cause of CSS and include pituitary adenomas, meningiomas, nasopharyngeal carcinoma, lymphoma, and metastases. CSS typically involves cranial nerves III, IV, V (V1, V2), and VI. Patients may complain of periocular pain, paresthesia, and diplopia.
The middle cranial fossa syndrome is characterized by facial numbness, paresthesias, or dysesthetic neuropathic pain in the distribution of the second or third divisions of the trigeminal nerve, and by associated motor deficits such as weakness in the masseter or temporalis muscles or abducens palsy.
Glossopharyngeal neuralgia may be the presenting symptom of the jugular foramen syndrome.22 Pain is perceived over the ear or the mastoid region and may radiate into the neck or shoulder. Neurologic deficits can include a Horner-syndrome as well as paresis of the palate, vocal cords, sternocleidomastoid muscle, or trapezius muscle. Syncopal attacks have also been reported.24 This syndrome has also been ascribed to leptomeningeal metastases25 and to local extension of head and neck malignancies.26 It is sometimes associated with syncope.
Tumors in the middle or posterior fossa rarely can produce a syndrome which resembles classical trigeminal neuralgia.27, 28, 29, 30 Leptomeningeal metastases in the posterior fossa can also generate this type of pain.31 A small fraction (between 1% and 6%) of patients with pain in the trigeminal distribution is discovered to have tumors affecting the trigeminal nerve.27, 28,30 The most common tumors are meningiomas, acoustic neuromas, and epidermoid tumors. Other tumors that have been reported to cause facial pain include trigeminal schwannomas, carcinomas of the cranial base, brainstem gliomas, arachnoid cysts, and lymphomas.32 Tumors affecting the trigeminal nerve root are typically associated with trigeminal neuralgia or tic douloureux, whereas tumors involving either the trigeminal ganglion or divisions are more likely to cause painful trigeminal neuropathy (atypical facial pain).27 New onset of trigeminal neuralgia in a patient with cancer should lead to careful imaging of the base of skull with computed tomography (CT) or MRI.28 Trigeminal neuralgia that is secondary to tumor usually presents as a constant, dull, well-localized pain related to the underlying pathology involving bone and other somatic structures, associated with paroxysmal episodes of lancinating or throbbing pain.33
Perineural spread of head and neck tumors may also be associated with significant pain. Squamous cell carcinomas of the face commonly extend by perineural spread, and are an important cause of facial pain syndromes.34 Other head and neck cancers spreading perineurally may also cause pain in a trigeminal distribution.35 Perineural spread, when present, typically involves cranial nerves V and VII because of their extensive subcutaneous distributions.36 Glossopharyngeal neuralgia usually is caused by local nerve infiltration in the neck or base of skull. It typically produces throat and neck pain, radiating to the ear and mastoid, and may be aggravated by swallowing. Occasionally, syncope accompanies severe pain.37, 38 Malignant mental neuropathy is a neurologic manifestation of cancer characterized by numbness in the region innervated by the mental nerve (skin of the chin, oral mucosa, and lower lip). Distally, mandibular bone tumors, with direct nerve infiltration, were the most frequent original neoplasm, being found in 50% of cases. Proximally, the most frequent were tumors located at the base of the skull; these lesions may cause bone destruction or infiltration of the leptomeninges close to the gasserian ganglion region.39 Although the lesion can be painful, it is relatively infrequent. The syndrome may be associated with breast cancer, lymphomas, prostate cancer, and leukemia. The appearance of the syndrome may be a warning sign of a systemic cancer or of its recurrence.
TUMOR-RELATED MONONEUROPATHY
Intercostal nerve injury secondary to rib metastases with local extension is the most commonly described tumorrelated painful mononeuropathy. Patients with tumor invasion of the sciatic notch may present with symptoms resembling sciatica. Other nerves may be involved as well, but this is not a common clinical issue.
RADICULAR PAIN/RADICULOPATHY
Radicular pain is described as corresponding to the dermatomal territory innervated by the dorsal spinal roots. Cancer-related radiculopathy may be unilateral or bilateral, but it tends to be unilateral in the cervical and lumbosacral regions and bilateral in the thorax. Radiculopathy in cancer patients typically is caused by epidural tumor mass or leptomeningeal metastases. Coughing, sneezing, positional change, and physical strain exacerbate the pain, which often has dysesthetic qualities. Leptomeningeal metastases are also capable of generating radicular pain and are characterized by multifocal neurological signs and symptoms at a variety of levels, including cranial neuralgias. Generalized headache with radicular pain in the low back and buttocks is a common presentation of this disease.40
LEPTOMENINGEAL METASTASES
Leptomeningeal metastasis has been described as the detection of tumor cells in the leptomeninges or cerebrospinal fluid (CSF) remote from the site of a primary tumor. Synonyms include carcinomatous meningitis, neoplastic meningitis, neoplastic meningosis, leukemic meningitis (for leukemia), lymphomatous meningitis (for lymphoma), and meningeal carcinomatosis (for carcinoma). Oncologists and neurologists have increasingly reported diffuse leptomeningeal metastases of extracranial malignant tumors, most commonly with adenocarcinoma of the lung and breast, lymphomas, and melanomas.40, 41, 42
Leptomeningeal spread has been reported in 5% to 8% of solid tumors, 5% to 29% of non-Hodgkin lymphomas (NHL), and 11% to 70% of leukemias.43 Although the incidence of metastatic lesions in the brain is high in patients with small-cell lung carcinoma (SCLC), clinical problems from metastases to the spinal cord or leptomeninges have been rare.44 Meningeal involvement was once a common complication of acute lymphoblastic leukemia before the advent of CNS prophylaxis, but it now occurs in fewer than 5% of patients. Leptomeningeal metastases develop in 1% to 8% of patients with systemic cancer45; median survival is 3 to 6 months.46 Without treatment, the prognosis is dismal: survival averages 6 weeks.47
Several mechanisms may be responsible for leptomeningeal spread, including hematogenous, direct extension, (transport through the valveless venous plexus, extension along nerves, perineural/perivascular lymphatics, escape from choroid plexus or subependymal metastases, and from surgical manipulation. Leptomeningeal tumors can encase spinal and cranial nerves or directly invade them and lead to demyelination and axon destruction. Dissemination, once tumor cells reach the leptomeninges, is by exfoliation into the CSF space. Leptomeningeal metastases can cause symptoms by direct compression of brain structures (by meningeal nodules causing focal symptoms), irritation of adjacent brain (seizures), blocking of CSF pathways (leading to hydrocephalus and increased intracranial pressure), ischemia, or stroke (by constriction of pial arteries), cranial and peripheral nerve palsies (by direct nerve involvement), metabolic derangements (by decreasing available glucose for brain by rapidly growing tumor cells), and by causing meningeal fibrosis.
The characteristic clinical presentation of leptomeningeal metastases is the simultaneous occurrence of symptoms and signs related to more than one area of the neuraxis. The clinical presentation of leptomeningeal metastasis is pleomorphic and commonly affects the cerebral hemispheres, cranial nerves, or spinal cord and its roots. Symptoms are usually multifocal and more diffuse than one discrete lesion could present. They include headache, back and radicular pain, multiple cranial and spinal nerve involvement, and alterations in mental status. Pain is present in 30% to 76% of cases.40,48Table 10.1 lists the frequency of spinal cord symptoms and signs in patients with leptomeningeal metastases. Pain is by far the most common symptom (80%); 25% of patients report diffuse headache; and pain in a spinal, radicular, or meningeal pattern is reported by 50%. Focal neurologic findings include cranial neuropathies, mononeuritis, radiculopathy, urinary incontinence, and visual disturbance.
The diagnosis is dependent upon identifying malignant cells with CSF examination or upon characteristic gadolinium-enhanced MRI findings. T1-weighted gadolinium-enhanced sequence of the entire neuraxis (brain and spine) plays an important role in supporting the diagnosis, demonstrating the involved sites and guiding treatment (Fig. 10.1). MRI images typically show enhancing nodular lesions. The combination of CSF studies and neuroimaging is the optimal diagnostic strategy. Neurologic examination will reveal multifocal involvement of the CNS, cranial nerves, and spinal roots, which are the clinical hallmark of this disease. Although CSF analysis is almost always abnormal, only a positive CSF cytology or demonstration of intrathecal synthesis of tumor markers is pathognomonic.
TABLE 10.1 FREQUENCY OF SPINAL CORD SYMPTOMS AND SIGNS IN PATIENTS WITH CARCINOMATOUS MENINGITIS
Symptoms or Signs
Percentage
Weakness
33
Paresthesia
31
Back pain
25
Radicular pain
19
Bowel/bladder dysfunction
13
Reflex asymmetry
67
Weakness
4
Cauda equina syndrome
33
Sensory loss
31
Positive straight leg raise
13
Decreased tone of anal sphincter
12
Nuchal rigidity
11
(With permission from Zachariah B, Zachariah SB, Varghese R, et al. Carcinomatous meningitis: Clinical manifestations and management. Int J Clin Pharmacol Ther. 1995;33:7-12. Copyright 1995, Drusti Verlag, Publisher.)
FIGURE 10.1 A 60-year-old woman with metastatic breast cancer who presented with increasing confusion and unsteadiness with walking. Sagittal lumbar spine MRI (T1, fat suppressed, postgadolinium) shows leptomeningeal enhancement in the thoracolumbar canal (arrows) with nodular meningeal enhancement in the lower lumbar region (arrow head). MRI, Magnetic resonance imaging.
CERVICAL PLEXOPATHY
Pain syndromes can arise from infiltration of the cervical plexus.49 The upper four cervical ventral rami join to form the cervical plexus, which lies adjacent to C1-C4 vertebrae. The four cutaneous branches can be found at the posterior border of the sternocleidomastoid muscle as they enter the posterior triangle of the neck. Nociceptive referral patterns from the face and neck overlap because sensory afferents from the cervical plexus terminate in the spinal tract of the trigeminal along with the sensory afferents from cranial nerves V, VII, IX, and X. Local pain accompanied by lancinating or dysesthetic components referred to the retroauricular and nuchal areas (lesser and greater auricular nerves), preauricular area (greater auricular nerve), anterior neck and shoulder (transverse cutaneous and supraclavicular nerves), and the jaw (marginomandibular nerve) characterize cervical plexopathy.21 Ipsilateral Horner syndrome or hemidiaphragmatic paralysis may also occur. CT or MRI evaluation may be necessary to determine the location of the tumor in soft tissues or within the epidural space. Local extension of a head and neck tumor or cervical lymph node metastasis is the common predisposing diagnosis. In patients with head and neck tumors who have previously had radical neck dissection and radiation therapy, new onset or worsening pain includes a differential diagnosis of post-radical neck dissection syndrome or tumor recurrence. Infections often complicate and exacerbate pain in this region.
BRACHIAL PLEXOPATHY
Lung or breast cancers are the most likely to invade the brachial plexus (Fig. 10.2). The lower plexus is usually the first portion to be involved. Tumor infiltration of the brachial plexus commonly stems from lymph node metastases from breast carcinoma or lymphoma, or by direct extension from lung carcinoma (ie, Pancoast tumor). The designation of “Pancoast” tumor is described in “Neoplastic Processes and Pain, Lung Cancer.” Both compression of the plexus or invasion of the nerves of the plexus by tumor cells can lead to severe, neuropathic pain.
Brachial plexopathy commences with pain in 85% of patients. Neurologic deficits usually develop well after the pain has become an issue.50, 51 The pain is then associated with numbness, paresthesias, allodynia, and hyperesthesias in the entire upper extremity (Fig. 10.3). Typically, the pain begins in the shoulder girdle, where it is often described as pressure or aching, and radiates to the elbow, medial forearm, and fourth and fifth fingers. This is related to the observation that initially the lower plexus is more likely to be involved than the upper portion. The triceps reflex is often absent. Eventually, the patient is likely to report a burning quality to the pain. Hyperesthesia along the ulnar aspect of the forearm and the hand is a frequent finding. Both motor and sensory changes usually imply C7, C8, and T1 involvement.51
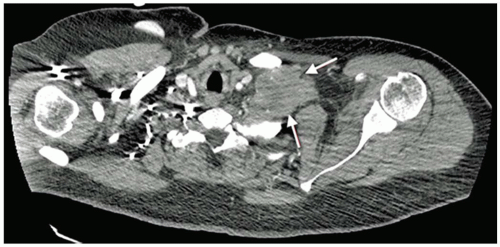
FIGURE 10.2 Chest CT scan of 53-year-old woman with inflammatory breast cancer. Patient had moderate-to-severe intensity pain in the left upper extremity and in the left upper posterior chest wall area. CT shows extensive left supraclavicular fossa mass involving the first rib and brachial plexus (arrows). CT, Computed tomography.
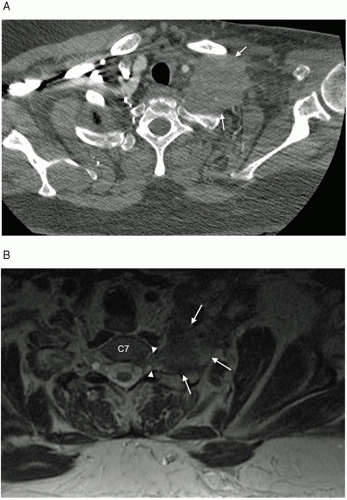
FIGURE 10.3 A 54-year-old woman with metastatic breast cancer to the left supra- and infraclavicular fossa involving the brachial plexus. Patient had severe pain, predominantly in the left shoulder region. Her left upper extremity was not functional, with evidence of diffuse lymphedema. Axial CT scan (A) shows an extensive mass below the clavicle (arrows). Axial MRI (B) shows a large mass in the left supraclavicular region (arrows) with abnormal contrast enhancement extending into the left C7-T1 neural foramen (arrow heads). The mass diffusely invades the brachial plexus. No mass is identified within the spinal canal. CT, Computed tomography; MRI, magnetic resonance imaging.
Upper plexus (C5, C6) involvement frequently leads to pain in the shoulder girdle, with burning pain in the tips of both the index finger and thumb. Upper plexus involvement usually progresses into panplexopathy. Lung tumors can present with pain in the distribution of the intercostobrachial nerve (axilla and upper chest wall).52
Horner syndrome and tumor invasion of adjacent vertebrae may accompany plexus invasion; there is a high risk of concurrent epidural extension.48,53 We advise that when a patient with tumor-based brachial plexopathy is imaged (usually with an MRI), the adjacent epidural space be included in the imaging. With this information, the radiation oncologist can plan the treatment field so as to include the entire tumor. Clinical examination findings can also imply tumor extension into the spinal foramina. A Spurling maneuver can help to identify the spinal canal as the site of pathology.54 The Spurling maneuver requires the examiner to produce oblique extension of the neck on the affected side with axial compression to the head. By narrowing the affected foramen, pain may be produced in the upper extremity. Any patient with paraspinal or foraminal disease should be suspected to harbor epidural extension of tumor.
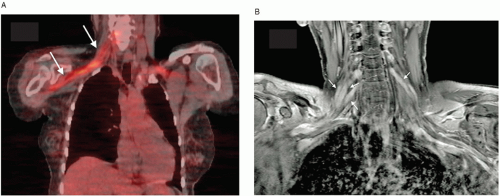
FIGURE 10.4 A 54-year-old woman with B-cell lymphoma. Complaining of diffuse weakness in the right upper extremity. No symptoms in left upper extremity. A: Coronal PET-CT shows FDG uptake extending from neural foramina C5, C6, and C7 extending along the entire brachial plexus (arrows). Coronal T1 MRI of the same patient shows markedly enhanced and enlarged nerve roots and trunks (arrows) on the right side. There is also evidence of enhancement on the left (arrow). PET-CT, Positron-emission tomography-computed tomography; MRI, magnetic resonance imaging.
Neuroradiologic evaluation for brachial plexopathy has been the CT and the MRI. Fluorodeoxyglucose (FDG)-PET scanning is a very useful tool for the assessment of patients with suspected metastatic plexopathy, particularly if other imaging studies are normal (Fig. 10.4).55 FDG-PET can also distinguish radiation-induced from metastatic plexopathy. Another useful tool to make this distinction is electromyography (EMG) (Table 10.2). In patients with metastatic brachial plexopathy, the EMG usually shows fibrillation potentials and positive waves (evidence of denervation) in affected muscles. Radiationinduced brachial plexopathy tends to have slowed nerve conduction velocity in both motor and sensory nerves.
LUMBOSACRAL PLEXOPATHY
The lumbosacral plexus can be damaged by direct tumor infiltration from adjacent soft tissues or lymph nodes or by compression from metastases in the adjacent bony pelvis. Local extension or nodal metastases from colorectal and other pelvic tumors (cervix, uterus, bladder, prostate), sarcomas (Fig. 10.5), and lymphomas are the common causes of lumbosacral plexopathy, but rarer causative neoplasms include metastases from breast or lung cancer or melanoma49 (Table 10.3). The most common neurologic complication in patients with advanced cervical cancer has been lumbosacral plexopathy caused by retroperitoneal lymph node metastases.56
Carcinomatous lumbosacral plexopathy is manifested by severe, aching, pressure-like, unrelenting pain localized varyingly in the pelvis, low back, or hip, or referred into the leg in a radicular or nonradicular pattern.57 The sites of referred pain are dependent upon the components of the plexus that are involved. The pain can be described as burning, cramping, or lancinating. Sensory symptoms of numbness and paresthesias, as well as weakness and leg edema, commonly develop weeks to months later. Lumbosacral plexopathy may lead to “hot and dry foot” syndrome that suggests sympathetic fiber dysfunction.58 Clinical signs of lumbosacral plexopathy are leg weakness (86%), sensory loss (73%), reflex loss (64%), and leg edema (47%). Associated findings commonly include positive straight-leg raising tests and sciatic notch tenderness.59
The specific clinical syndrome produced by tumor invasion of the lumbosacral plexus depends on the levels of nerve involvement. Approximately one third of patients will present with infiltration of the upper plexus and present with pain in the back, lower abdomen, flank, iliac crest, or anterolateral thigh as well as neurological findings suggesting L1-L4 involvement. Involvement of the lower plexus occurs in approximately one half of patients and presents with pain in the buttocks and perineum with referral to the posterolateral leg and thigh. L4-S1 neurological deficits, leg edema, and bowel or bladder dysfunction (Fig. 10.6) frequently accompany the pain. Sacral plexopathy may arise directly from a bony sacral lesion or a presacral mass. Involvement of the lumbosacral trunk is characterized by numbness of the dorsal medial foot and sole with associated weakness of knee flexion, ankle dorsiflexion, and inversion. Sphincter dysfunction and perineal sensory loss are caused by coccygeal plexus invasion. One fifth of patients manifest panplexopathy; their pain may refer anywhere in the territory of the lumbosacral plexus. Associated leg edema frequently accompanies lumbosacral plexopathy.58
Jaeckle et al.57 reported on 85 patients with lumbosacral plexopathy and pelvic tumor documented by CT or biopsy. They described three clinical syndromes: lower (L4-S1), 51%; upper (L1-L4), 31%; and panplexopathy (L1-S3), 18%. Three fourths of the patients reported the insidious onset of pelvic or radicular leg pain, followed by sensory symptoms and weakness that began weeks to months later. The combination of leg pain, weakness, edema, rectal mass, and hydronephrosis suggests plexopathy due to cancer. CT showed pelvic tumor in 96% of such patients. Roughly, one half of such patients will have epidural extension seen on an imaging study.
TABLE 10.2 DIFFERENTIATING FEATURES OF BRACHIAL PLEXOPATHY INDUCED BY TUMOR INFILTRATION, RADIATION FIBROSIS, AND REVERSIBLE RADIATION INJURY
Tumor Infiltration
Radiation Fibrosis
Reversible Radiation Injury
Incidence of pain
89%
18%
40%
Typical location of pain
Shoulder upper arm, elbow, radiating to 4th and 5th fingers
Shoulder wrist, hand
Hand, forearm
Nature of pain
Dull aching in shoulder,
Lancinating pain in elbow and ulnar aspect of hand
Occasional dysesthesias, burning, or freezing sensations
Aching shoulder pain
Paresthesias in C5, C6 distribution in hand
Aching shoulder pain
Paresthesias in hand and forearm
Severity of pain
Moderate to severe (severe in 98% of patients)
Mild to moderate (severe in 35% of patients)
Mild
Course
Progressive neurologic dysfunction; atrophy and weakness with C7-T1 distribution; persistent pain; Horner syndrome
Progressive weakness with C5, C6 distribution; stabilizing pain with appearance of weakness
Transient weakness and atrophy affecting C6-C7, T1; complete resolution of motor findings
CT scan findings
Circumscribed mass with diffuse infiltration of tissue planes
Diffuse infiltration of tissue planes
Normal
EMG findings
Segmental slowing; no myokymia
Myokymia
Segmental slowing; no myokymia
CT, Computed tomography; EMG, electromyography. (Modified from Foley KM. Brachial plexopathy in patients with breast cancer. In: Harris JR, Hellman S, Henderson IC, Kinne DW, eds. Breast diseases. Philadelphia: JB Lippincott Co, 1987:537.)
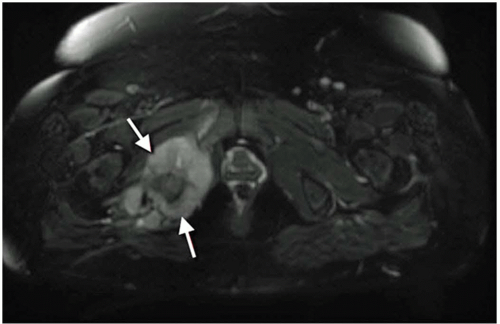
FIGURE 10.5 Axial Fat-suppressed MRI scan of pelvis. Patient is a 34-year-old woman with extensive tumor infiltration from a recurrent high-grade pelvic sarcoma on the right side extending toward the right hip joint and soft tissues adjacent to the right ischial tuberosity and greater and lesser sciatic foramen (arrows). Patient complained of severe right hip and lower extremity pain, necessitating placement of an externalized intrathecal catheter for pain control. MRI, Magnetic resonance imaging.
Patients who have been previously treated with radiation therapy present a difficult distinction between tumor or radiation plexopathy. MRI has been found to be more sensitive than CT for diagnosing cancer-induced lumbosacral plexopathy.60 MRI is, therefore, the best choice for the evaluation of patients with clinical and electrophysiologic evidence of plexopathy who are suspected to have a systemic cancer. Imaging must include the L1 vertebral body through to the true pelvis. The common neurologic findings include leg weakness, sensory loss, reflex asymmetry, focal tenderness to palpation (in the lumbar region in an upper plexopathy, sciatic notch and sacrum in a lower plexopathy, and lumbosacral region in pan-plexopathy), rectal mass, decreased sphincter tone, and positive direct and reverse straight leg raising signs.
TABLE 10.3 COMMON NEOPLASMS CAUSING LUMBOSACRAL PLEXOPATHY
Tumor
% of Lumbosacral Plexopathy
Colorectal
20
Sarcoma
16
Breast
11
Lymphoma
9
Cervix
7
All Others
7
(From Jaeckle KA. Neurological manifestations of neoplastic and radiationinduced plexopathies. Semin Neurol. 2004;24(4):385-393. Reprinted with permission from Thieme, Inc.)
FIGURE 10.6 Coronal T1 MRI showing enlarged left L4 nerve root (arrow). Patient is a 36-year-old man with peripheral nerve sheath tumor. MRI, Magnetic resonance imaging.
TUMOR INFILTRATION OF THE SACRUM AND SACRAL NERVES
Pain over the sacrum is usually the result of the spread of cancer of the bladder, pelvic organs, or colon. Such tumors lead to a dull, aching midline pain as well as burning or throbbing pain in the soft tissues of the rectal and/or perineal region. The pain is exacerbated by sitting or lying. With bilateral involvement, sphincter incontinence and impotence in the male are commonly seen. The sacrum and the sciatic notches may be tender to palpation. Both direct and reverse straight leg raising tests may be positive. Compromise of the S1 and S2 roots can lead to weakness of ankle plantar flexion and the absence of ankle jerk reflexes (Fig. 10.7). There is usually sensory loss in both the perianal and genital regions; pain and sensory loss as well as distortions of sensation are common.
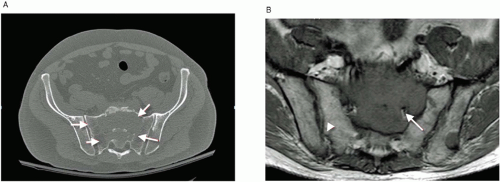
FIGURE 10.7 A: CT of pelvis in 61-year-old man who presented with extensive lytic lesion completely replacing the sacrum (arrows) and involving the sacral foramina from a tumor of unknown origin. B: Axial T1 MRI of sacrum of same patient showing left S2 nerve root encroachment of tumor (arrow). The sacrum is essentially replaced with tumor. Arrow head shows normal bone. CT, Computed tomography; MRI, magnetic resonance imaging.
SPINAL AND RADICULAR PAIN
Radicular pain is reported as radiating into a limb or around the trunk wall. The pain is sharp and lancinating in quality and travels in a restricted zone from central to peripheral. It may be described as episodic, recurrent, or paroxysmal. Although radicular pain may be described by some patients as a deep tissue pain, it almost always has a cutaneous component in proportion to the number of cutaneous afferent fibers that are ectopically activated. Nociceptive pain is induced by activity at the peripheral terminals of Aδ and C fibers, whereas radicular pain is caused by the ectopic firing of axons and does not originate in nerve terminals. Ectopic activation of axons may occur as a result of mechanical deformation of a dorsal root ganglion, mechanical stimulation of previously damaged axons in peripheral nerve or nerve roots, inflammation of a dorsal root ganglion, and possibly by ischemic damage to the dorsal root ganglia. Acute or chronic spine pain may be described as cramping or knifelike, but may also be just dull or aching. Chronic spine pain without a radicular component is generally aching, dull, or burning, or any combination of these three features. Movement or change in position often exacerbates spinal pain.
CENTRAL PAIN CAUSED BY CANCER
Central pain is defined as pain due to disease or dysfunction in the CNS and includes pathology in the spinal cord, brain stem, or cerebral hemispheres. Central pain mechanisms are complex. Gain in neuronal excitability, loss of inhibition, and increased facilitation may contribute to a central sensitization and disinhibition of pain pathways.7 Central pain problems due to spinal cord injury and stroke are well described.61, 62 Damage to spinothalamic sensory pathways, although not the only mechanism, is thought to be important in the pathogenesis of both of these sources of neuropathic pain. In addition, damage to the pain and temperature pathways is an important contributor to the development of central pain in traumatic brain injury patients.63 The occurrence of hyperexcitability and hyperreactivity within the nervous system is also an important mechanism in the pathogenesis of central pain. Clinically, this may be manifested by the presence of allodynia, hyperpathia, and exaggerated wind-up sensations. Electrophysiologic studies and brain scans confirm that deafferented neurons in the thalamus and somatosensory cortex of patients with central pain may undergo plastic changes and become hyperexcitable.64, 65, 66 At a cellular level, the glia play a crucial role in the maintenance of neuronal homeostasis in the CNS.67, 68 Glial cells represent 70% of the cells in the CNS under normal conditions, and microglia represent 5% to 10% of glia.69 Microglia are rapidly activated in the CNS in response to pathological events, including trauma, ischemia, inflammation, hypoxia, neurodegeneration, and viral or bacterial infection, releasing proinflammatory cytokines and causing pathological pain.70 Microglia also repair injured cells by releasing neurotrophic factors and appear to dynamically modulate neuronal function under both normal and pathological conditions.68 Microglial cells secrete a large variety of substances, including growth factors, cytokines, complement components, lipid mediators, extracellular matrix components, enzymes, free radicals, neurotoxins, nitric oxide, and prostaglandins.71 Microglial activation appears to have an important role in neuropathic pain.72
Central pain syndromes are not commonly ascribed to cancer. Gonzales et al.73 reported on the prevalence and characteristics of central pain states in hospitalized patients with cancer. The prevalence of central pain was 4%. Primary and metastatic tumors and their treatment, including surgery, radiation, and chemotherapy, were all potential causes. Furthermore, the occurrence of central pain in patients with primary CNS tumors was higher in patients with spinal tumors compared to patients with brain tumors (P < .0001). Of the 27 patients reported with cancer or cancer treatment-related central pain, nearly all levels of the CNS were involved in central pain, except for the brainstem. Including leptomeningealrelated pain, 78% of patients had a spinal cord site of injury. Seventeen patients had thoracic spinal cord injury pain, two had cervical cord injury pain, and three parietal injury pain. The primary CNS tumor types included spinal cord ependymoma,4 astrocytoma,1 melanocytoma,1 glioblastoma,1 neuroectodermal,1 melanocytoma;1 thalamic oligodendroglioma,1 lymphoma,1
Only gold members can continue reading. Log In or Register to continue