(T) Primary Tumor | Adapted from 7th edition AJCC Staging Forms. | |
TNM | Definitions | |
TX | Primary tumor cannot be assessed | |
T0 | No evidence of primary tumor | |
Tis | Carcinoma in situ | |
Maxillary Sinus | ||
T1 | Tumor limited to maxillary sinus mucosa with no erosion or destruction of bone | |
T2 | Tumor causing bone erosion or destruction including extension into hard palate &/or middle nasal meatus, except extension to posterior wall of maxillary sinus and pterygoid plates | |
T3 | Tumor invades any of the following: Bone of posterior wall of maxillary sinus, subcutaneous tissues, floor or medial wall of orbit, pterygoid fossa, ethmoid sinuses | |
T4a | Moderately advanced local disease: Tumor invades anterior orbital contents, skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid or frontal sinuses | |
T4b | Very advanced local disease: Tumor invades any of the following: Orbital apex, dura, brain, middle cranial fossa, cranial nerves other than maxillary division of trigeminal nerve (V2), nasopharynx, or clivus | |
Nasal Cavity and Ethmoid Sinus | ||
T1 | Tumor restricted to any 1 subsite, ± bony invasion | |
T2 | Tumor invading 2 subsites in a single region or extending to involve an adjacent region within nasoethmoidal complex, with or without bony invasion | |
T3 | Tumor extends to invade medial wall or floor of orbit, maxillary sinus, palate, or cribriform plate | |
T4a | Moderately advanced local disease: Tumor invades any of the following: Anterior orbital contents, skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid or frontal sinuses | |
T4b | Very advanced local disease: Tumor invades any of the following: Orbital apex, dura, brain, middle cranial fossa, cranial nerves other than (V2), nasopharynx, or clivus | |
(N) Regional Lymph Nodes | ||
NX | Regional lymph nodes cannot be assessed | |
N0 | No regional lymph node metastasis | |
N1 | Metastasis in a single ipsilateral lymph node, ≤ 3 cm in greatest dimension | |
N2 | Metastasis in a single ipsilateral lymph node, > 3 cm but ≤ 6 cm in greatest dimension, or in multiple ipsilateral lymph nodes, none > 6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, none > 6 cm in greatest dimension | |
N2a | Metastasis in a single ipsilateral lymph node, > 3 cm but ≤ 6 cm in greatest dimension | |
N2b | Metastasis in multiple ipsilateral lymph nodes, none > 6 cm in greatest dimension | |
N2c | Metastasis in bilateral or contralateral lymph nodes, none > 6 cm in greatest dimension | |
N3 | Metastasis in a lymph node, > 6 cm in greatest dimension | |
(M) Distant Metastasis | ||
M0 | No distant metastasis | |
M1 | Distant metastasis | |
(G) Histologic Grade | Adapted from 7th edition AJCC Staging Forms. | |
TNM | Definitions | |
GX | Grade cannot be assessed | |
G1 | Well differentiated | |
G2 | Moderately differentiated | |
G3 | Poorly differentiated | |
G4 | Undifferentiated | |
AJCC Stages/Prognostic Groups | Adapted from 7th edition AJCC Staging Forms. | ||
Stage | T | N | M |
0 | Tis | N0 | M0 |
I | T1 | N0 | M0 |
II | T2 | N0 | M0 |
III | T3 | N0 | M0 |
T1 | N1 | M0 | |
T2 | N1 | M0 | |
T3 | N1 | M0 | |
IVA | T4a | N0 | M0 |
T4a | N1 | M0 | |
T1 | N2 | M0 | |
T2 | N2 | M0 | |
T3 | N2 | M0 | |
T4a | N2 | M0 | |
IVB | T4b | Any N | M0 |
Any T | N3 | M0 | |
IVC | Any T | Any N | M1 |
Kadish Staging System for Esthesioneuroblastoma | |
Group A | Tumor localized to nasal cavity |
Group B | Tumor localized to nasal cavity and sinuses |
Group C | Tumor extends beyond nasal cavity and sinuses to skull base, anterior cranial fossa, orbit, or neck nodes, with or without distant metastases |
Hyams Histologic Grading System for Esthesioneuroblastoma | ||||
Microscopic Features | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
Architecture | Lobular | Lobular | ± lobular | ± lobular |
Pleomorphism | Absent to slight | Present | Prominent | Marked |
Neurofibrillary matrix | Prominent | Present | May be present | Absent |
Rosettes | Present1 | Present1 | May be present2 | May be present2 |
Mitoses | Absent | Present | Prominent | Marked |
Necrosis | Absent | Absent | Present | Prominent |
Glands | May be present | May be present | May be present | May be present |
Calcification | Variable | Variable | Absent | Absent |
Adapted from Barnes L et al: World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press, 2005. 1 Homer Wright rosettes (pseudorosettes). | ||||
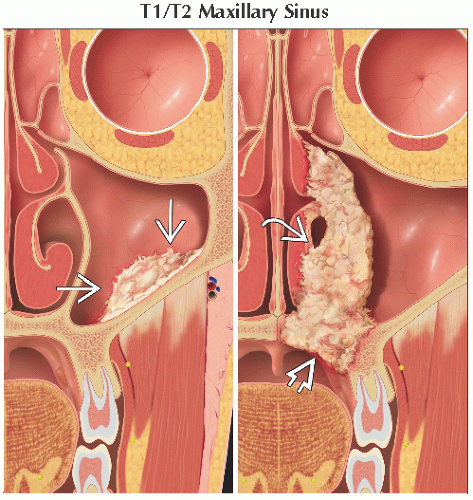 Coronal graphic shows a small T1 tumor  confined to the maxillary mucosa without bone destruction. On the right, there is a larger tumor that destroys bone and also extends to the hard palate confined to the maxillary mucosa without bone destruction. On the right, there is a larger tumor that destroys bone and also extends to the hard palate  and middle meatus and middle meatus  . Any of these features designate this as a T2 tumor. . Any of these features designate this as a T2 tumor. |
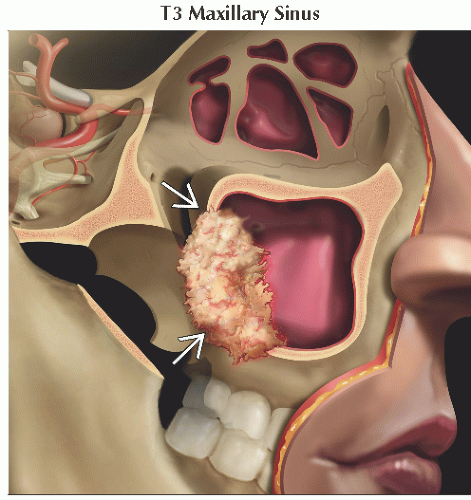 Graphic shows a T3 carcinoma invading the posterior bony wall of the maxillary sinus  . T3 disease is also determined by invasion of the floor or medial wall of the orbit &/or involvement of the ethmoid sinus, pterygoid fossa, or subcutaneous tissues. . T3 disease is also determined by invasion of the floor or medial wall of the orbit &/or involvement of the ethmoid sinus, pterygoid fossa, or subcutaneous tissues. |
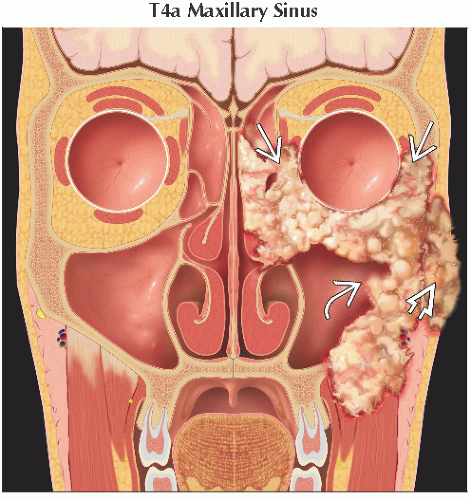 Coronal graphic shows a T4a maxillary sinus carcinoma  , which is invading the anterior orbit , which is invading the anterior orbit  as well as extending out to the skin of the cheek as well as extending out to the skin of the cheek  . T4a disease is also determined by invasion of pterygoid plates, infratemporal fossa, cribriform plate, and sphenoid or frontal sinuses. . T4a disease is also determined by invasion of pterygoid plates, infratemporal fossa, cribriform plate, and sphenoid or frontal sinuses. |
 Graphic demonstrates very advanced local disease with maxillary sinus tumor  invading posteriorly and superiorly to the orbital apex invading posteriorly and superiorly to the orbital apex  . T4b disease is also designated when there is invasion of dura, brain, middle cranial fossa, nasopharynx, clivus, or cranial nerves other than maxillary division of trigeminal nerve. . T4b disease is also designated when there is invasion of dura, brain, middle cranial fossa, nasopharynx, clivus, or cranial nerves other than maxillary division of trigeminal nerve. |
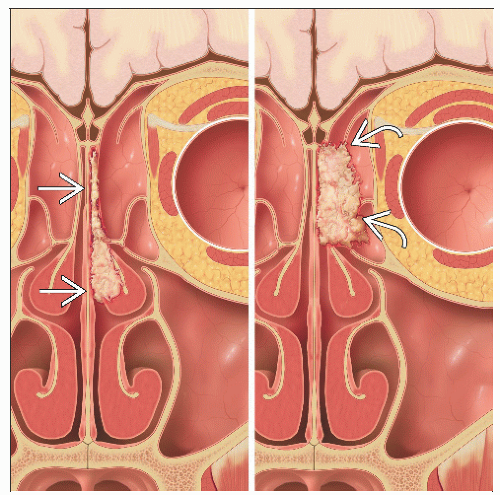
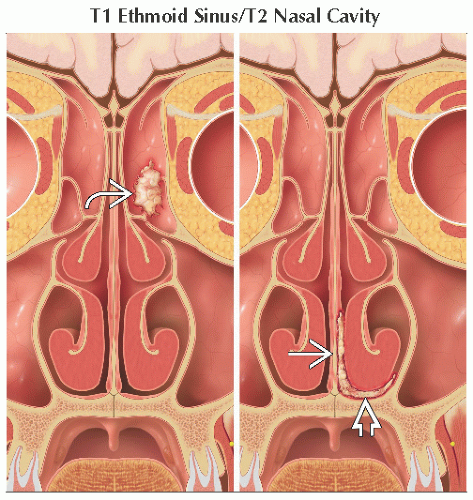 Coronal graphic (left) shows a small tumor confined to the left ethmoid air cells  , which is a T1 tumor. On the right, there is a small tumor involving the nasal septum , which is a T1 tumor. On the right, there is a small tumor involving the nasal septum  and nasal floor and nasal floor  . Involvement of two subsites in the nasal cavity makes this a T2 tumor. . Involvement of two subsites in the nasal cavity makes this a T2 tumor. |
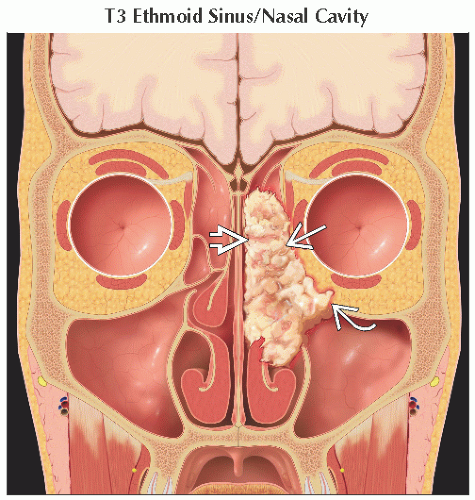 Coronal graphic shows an ethmoid tumor  , which extends to the medial orbital wall , which extends to the medial orbital wall  and orbital floor and orbital floor  . Maxillary sinus, palate, or cribriform plate invasion also constitute T3 disease. . Maxillary sinus, palate, or cribriform plate invasion also constitute T3 disease. |
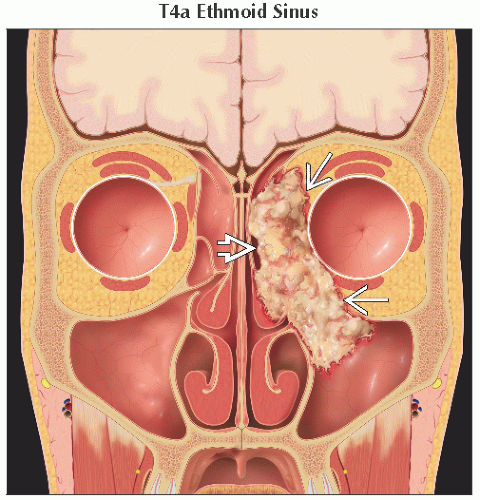 Coronal graphic illustrates a T4a ethmoid sinus carcinoma  invading the anterior orbit invading the anterior orbit  . T4a disease is also determined by invasion of the skin of the nose or cheek, minimal extension to the anterior cranial fossa, pterygoid plates, or sphenoid or frontal sinuses. . T4a disease is also determined by invasion of the skin of the nose or cheek, minimal extension to the anterior cranial fossa, pterygoid plates, or sphenoid or frontal sinuses. |
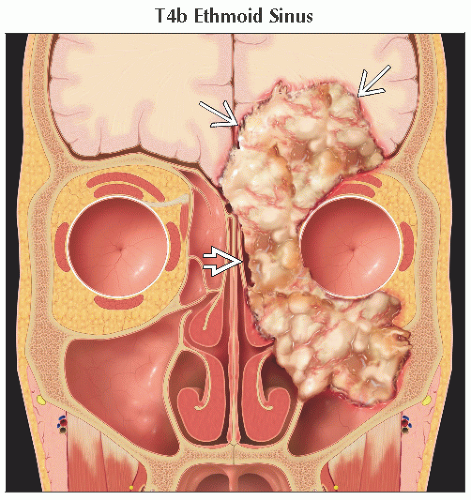 Coronal graphic shows a very advanced local ethmoid tumor  with extensive intracranial invasion with extensive intracranial invasion  in addition to orbital and maxillary sinus invasion. T4b disease is also evident when there is orbital apex, middle cranial fossa, clivus, nasopharynx, or cranial nerve (other than CN V2) involvement. in addition to orbital and maxillary sinus invasion. T4b disease is also evident when there is orbital apex, middle cranial fossa, clivus, nasopharynx, or cranial nerve (other than CN V2) involvement. |
 Coronal graphic (left) demonstrates a small tumor confined to the nasal cavity  , which is Kadish A and the least common form. On the right, there is extension of tumor from the nasal cavity to the paranasal sinuses , which is Kadish A and the least common form. On the right, there is extension of tumor from the nasal cavity to the paranasal sinuses  , which is Kadish B. , which is Kadish B. |
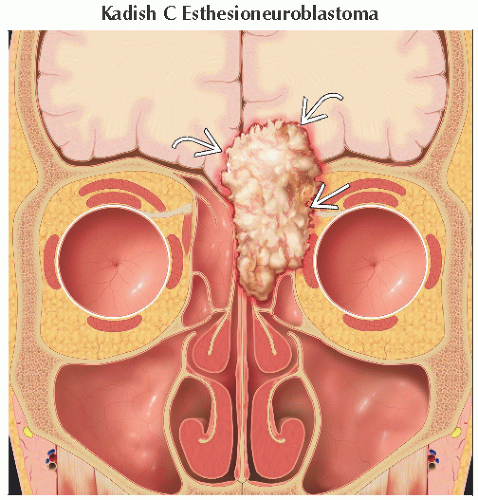 Coronal graphic illustrates a Kadish C tumor with extension beyond the nasal cavity and sinuses, into both the orbit  and anterior cranial fossa and anterior cranial fossa  . Kadish D was not in the original staging system, but indicates nodal &/or distant metastases. . Kadish D was not in the original staging system, but indicates nodal &/or distant metastases. |
Rare malignancies arising from nasal cavity and paranasal sinus
Incidence of 1 per 100,000 or 3% of upper respiratory cancers
Maxillary sinus is the most common site of sinonasal malignancies
60-80% of paranasal sinus tumors arise from maxillary antrum
Squamous cell carcinoma is the most common histology
Adenocarcinomas tend to occur in ethmoid sinuses or upper nasal cavity
Esthesioneuroblastoma (ENB) originates from neuroectoderm; rare (2% of nasal malignancies)
Referred to as olfactory neuroblastoma
Arises from olfactory mucosa of superior 1/3 of nasal septum, cribriform plate, and superior turbinates
Subsites anatomy
Nasal cavity
Nasal vestibule
Nasal fossa: Septum, floor, lateral wall
Paranasal sinuses
Maxillary sinuses
Ethmoid sinuses
Sphenoid sinuses
Frontal sinuses
Late clinical presentation often results in advanced stage of disease
Regional LN spread is relatively uncommon, can occur in advanced T stage tumors
Involvement of nodal sites: Buccinator,
submandibular, upper jugular, and retropharyngeal nodes
Bilateral spread may occur when primary extends beyond midline
Primary malignant tumors (WHO classification)
Carcinomas
Squamous cell carcinomas
Verrucous carcinoma
Papillary squamous cell carcinoma
Basaloid squamous cell carcinoma
Spindle cell carcinoma
Adenosquamous carcinoma
Acantholytic squamous cell carcinoma
Lymphoepithelial carcinoma
Sinonasal undifferentiated carcinoma
Adenocarcinoma
Intestinal-type adenocarcinoma
Non-intestinal-type adenocarcinoma
Neuroendocrine tumors
Typical carcinoid
Atypical carcinoid
Small cell carcinoma, neuroendocrine type
Soft tissue tumors
Malignant tumors
Fibrosarcoma
Malignant fibrous histiocytoma
Leiomyosarcoma
Rhabdomyosarcoma
Angiosarcoma
Malignant peripheral nerve sheath tumor
Tumors with low malignant potential/borderline tumors
Desmoid-type fibromatosis
Inflammatory myofibroblastic tumor
Glomangiopericytoma (sinonasal-type hemangiopericytoma)
Extrapleural solitary fibrous tumor
Tumors of bone and cartilage (malignant subtype)
Chondrosarcoma
Mesenchymal chondrosarcoma
Osteosarcoma
Chordoma
Hematolymphoid tumors
Extranodal NK-/T-cell lymphoma
Diffuse large B-cell lymphoma
Extramedullary plasmacytoma
Extramedullary myeloid sarcoma
Histiocytic sarcoma
Langerhans cell histiocytosis
Neuroectodermal tumors
Ewing sarcoma
Primitive neuroectodermal tumor
Olfactory neuroblastoma (ENB)
Melanotic neuroectodermal tumor of infancy
Mucosal malignant melanoma
Germ cell tumors
Immature teratoma
Teratoma with malignant transformation
Sinonasal yolk sac tumor (endodermal sinus tumor)
Sinonasal teratocarcinosarcoma
Mature teratoma
Dermoid cyst
Mucosal melanoma
Secondary tumors
Comments
Sinonasal carcinoma
Most patients older than 40 years of age
Minor salivary gland tumors and ENB tend to appear before age 20
Early symptoms are vague
Nasal cavity: Unilateral nasal obstruction, epistaxis
Maxillary sinus: Most often do not present early
Advanced stage
Aggressively spreads to adjacent structures, facial pain, intranasal/intraoral mass, ocular symptoms
Sinonasal carcinoma
Generally a relatively rare cancer, although more prevalent in Japan, South Africa
Demographics
Age: 95% of patients > 45 years of age
Gender: M:F =2:1
Approximately 2,000 new cases per year in USA
Approximately 3% of head and neck cancers
European data show incidence < 2 per 100,000 men and 1 per 100,000 women
Risk factors
Tobacco use
Alcohol use
Viruses
Associations with HPV and EBV have been postulated
HPV is especially important in carcinomas arising from inverted papillomas
Occupational exposures (e.g., textile, leather, formaldehyde, and wood dust)
Age
ENB
Age
Broad range: 3-88 years
Bimodal distribution centered in 2nd and 6th decades of life
Gender: Slightly more common in females
Sinonasal carcinoma
Possible link to abnormal expression of p53
ENB
Cytogenetic abnormalities (e.g., translocations)
Sinonasal carcinoma
Polypoid morphology
Papillary or fungating growth
Tan-white or pinkish red color
ENB
Broad-based, pedunculated, lobulated, soft, glistening mass covered in mucosa
Red-gray, red-brown color
H&E
Squamous cell carcinoma
Keratinizing subtype (80%)
Papillary, exophytic, or inverted patterns in architecture
Surface and individual cell keratinization
Dyskeratosis
Poorly to well differentiated
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree