Highlights
- •
Active surveillance is a valid and safe option for the management of small renal masses.
- •
Clinical factors influencing decision for intervention include age, growth rate, intial size and initial biopsy.
- •
Rapidly growing small renal masses have higher probability of harboring adverse histology.
Abstract
Introduction
Active surveillance (AS) is a safe strategy for small renal masses (SRM) suspicious of renal cell carcinoma. In this study we analyze real world outcomes of active surveillance SRM from 5 tertiary Spanish centers, assessing clinical, radiological, and pathological characteristics, as well as therapeutic options.
Methods
A multicenter retrospective review was conducted including patients on AS from January 2012 to September 2024. We analyzed the indication for AS, initial lesion size, growth rate (GR), and progression on active surveillance. Cox regression analysis was performed to identify predictor of deferred intervention (DI).
Results
A total of 384 patients with renal tumors were included in AS, with an initial mean tumor size of 20.5mm. With a mean follow-up period of 43 months, the average GR across the cohort was 1.4 mm/y. About 15% of patients ( n = 59) received active treatment (partial nephrectomy 56%, radical nephrectomy 16%, and radiofrequency 28%). Age, tumor size and tumor growth were factors correlated with delayed intervention, and only initial tumor size was correlated with GR. Pathological analysis after active treatment showed high grade clear cell carcinoma in 43.5% of cases with a GR of > 5 mm/y, as compared to 19.4% of oncocytomas in slow growing lesions. No disease progression nor cancer-specific deaths were observed in our series.
Conclusions
In our multicenter cohort, AS is a valid option for SRMs without affecting oncological outcomes, with clinical factors such as age, tumor size, GR and initial biopsy influencing decisions on intervention.
1
Introduction
The management of small renal mass has been evolving in the last decades with the advent of novel diagnostic techniques as well as the development of novel therapeutic approaches. Increase of the availability of different imaging techniques have led to a surge in the incidental diagnosis of small renal masses [ ]. Nowadays, the natural history of small renal masses has been understood more thoroughly [ ], yet not to the extent of using precision medicine in this field. Small renal masses have less intratumoral heterogeneity [ , ] and have a very low potential of metastatic disease. Moreover, 20% of treated masses under 4cm are benign [ ].
Current management of SRM involves surgery with partial nephrectomy as the standard approach, in addition to ablative therapy such as cryoablation or radiofrequency [ ]. On the other hand, active surveillance (AS) offers a noninterventional approach with the option to delayed treatment in case of progression [ ]. Over the past decade, more data from prospective registries have emerged showing the safety and feasibility of AS in this field [ ]. Moreover, these registries had a robust follow up and therefore provided a granular analysis of progression patterns during surveillance. However, no standardized protocol is established regarding inclusion criteria, role of biopsy, follow-up, and triggers for treatment.
In this study, we provide a descriptive analysis of real-world outcomes from a multicentric active surveillance cohort, with special emphasis on the current trend in management of SRM and factors that trigger delayed intervention (DI).
2
Patients and methods
A retrospective study from 2012 to 2024 was conducted at 5 Spanish high volume centers including patients who presented with an incidental renal mass diagnosed by contrast imaging and underwent active surveillance. Institutional review board (IRB) approval was obtained from each center prior to the initiation of data collection.
Patients with hereditary syndrome were excluded from the study. Baseline characteristics were recorded, including cardiovascular morbidities and Charlson score index. Tumor features were also collected, based on the initial characterization by computed tomography (CT) or magnetic resonance image (MRI). The use of initial renal mass biopsy upon inclusion in AS was based on shared decision making between patients and providers and each center´s protocol. All lesions included in the study were contrast enhancing masses.
All patients included in this study were offered and accepted active surveillance. Inclusion criteria was categorized based on initial tumor size (< 2cm lesions), presence of comorbidities, performance status, chronic kidney disease, patient´s preference. Follow up was done alternating ultrasound imaging with CT or MRI contrasted imaging. Initial and subsequent tumor sizes were recorded using the maximal tumor diameter (MTD). Growth rate (GR) was calculated based on linear change of tumor size over follow up time. Patients were counseled for active treatment if GR overcomes 5mm per year, tumor size more than 4cm or per patient´s personal decision. Progression was defined either by GR greater than 5 mm/y, tumor size over 3 cm, development of metastasis, and patient´s personal preference to undergo definitive treatment. Patients were counseled for active treatment, either for partial or radical nephrectomy or ablative therapy.
Primary outcome was the analysis of progression rate on AS. Patient´s baseline characteristics and radio-pathologic features were analyzed and compared among patients who continued active surveillance and those who progressed. Secondary outcome included the GR which was examined as continuous and categorical variable, where it is classified as fast-growing or with significant growth if increase in MTD is greater than 5 mm/y or slow growing lesions if it is less than 5 mm/y. Baseline features and outcomes were compared based on growth kinetics and age. A cutoff age of 70 years was considered for this analysis. Follow up time was defined as time from diagnosis till active treatment or last imaging test in case of continuing surveillance. Other secondary outcomes included histopathologic assessment in DI group.
3
Statistical analysis
Means and standard deviations are reported for descriptive statistics. Descriptive statistics and frequency tables were used to summarize the data. Pearson’s chi-square tests (or Fisher’s exact test) were used for categorical variables. Student-t or ANOVA tests were performed for continuous variables. Multivariate Cox proportional hazard regression analysis was performed to identify predictors of DI. Statistical analyses were performed using SPSS version 29. A P -value < 0.05 indicated statistical significance.
4
Results
4.1
Baseline characteristics
A total of 384 patients were included in this study. Mean age was 72.6 years (SD = 11.3), and 58% of patients were males. Mean body mass index (BMI) was 28 kg/m 2 (SD = 5.1). The initial mean tumor size was 20.5 mm (SD = 14). About 11% of patients underwent biopsy upon inclusion into active surveillance program. The biopsies revealed 25% oncocytomas, 18% clear cell renal cell carcinomas (ccRCCs), 11% papillary, 9% chromophobe and 16% nondiagnostic ( Table 1 ). The main cause for inclusion in AS was presence of very small size tumors (less than 2cm) in the 62% of the cases, presence of comorbidities in 30%, and patient´s personal preference in 8%.
| Overall (384) | No delayed intervention (325) | Delayed intervention (59) | P -value | |
|---|---|---|---|---|
| Age at diagnosis | 72.6 (11.3) | 73.5 (11.2) | 67.7 (11.1) | < 0.001 |
| Sex (male%) | 223 (58.1%) | 171 (55.7%) | 39 (66%) | 0.311 |
| BMI | 28.2 (5.1) | 28 (5.8) | 28.9 (5.2) | 0.288 |
| Creatinine | 1.39 (4.07) | 1.4 (4.47) | 1.2 (0.6) | 0.6 |
| GFR | 63.85 (22) | 63.46 (22) | 64.2 (22) | 0.8 |
| Initial size (mm) | 20.5 (14) | 20.1 (10.9) | 22.7 (25) | 0.19 |
| Final size (mm) | 24 (13.7) | 23.14 (13.1) | 28.7 (15.5) | 0.004 |
| Follow-up time (mo.) | 43.8 (30.7) | 45.6 (31) | 33 (24) | 0.002 |
| Growth rate (mm/y) | 1.4 (3.6) | 0.8 (2.8) | 4.4 (5.9) | < 0.001 |
| % growth rate > 5mm | 40 (10.5%) | 17 (5.3%) | 23 (39%) | < 0.001 |
| Initial biopsy | 43 (11%) | 33 (10.5%) | 10 (17.5%) | 0.174 |
| oncocytoma | 11 (25.6%) | 11 (33.3%) | 0 | 0.007 |
| ccRCC | 8 (18.6%) | 5 (15.2%%) | 3 (30%) | |
| Papillary | 5 (11.6%) | 1 (3%) | 4 (40%) | |
| Chromophobe | 4 (9.3%) | 2 (6.1%) | 2 (20%) | |
| Non diagnostic | 7 (16.3%) | 7 (21%) | 0 | |
| Other histology | 8 (18.6%) | 7 (21.2%) | 1 (10%) |
4.2
Outcomes and crossover to intervention
With a mean follow up period of 43 months (SD = 30.7), average GR was 1.4 mm/y (SD = 3.6). 10.5% of patients presented a GR greater than 5 mm/y. About 59 patients (15.3%) required active treatment. The main reasons for DI were significant GR(> 5 mm/y) in 71% of the cohort, patient´s desire in 10%, improvement of performance status in 10%, and tumoral size greater than 3cm in 7%. Partial nephrectomy was the most common treatment (56%) followed by ablation (28%) and radical nephrectomy (16%).
Patients who underwent DI were younger (67 years vs. 73-year-old, P < 0.001) and had higher GR (4.4 mm/y vs. 0.8 mm/y, P < 0.001) compared to those who remained in AS. None of the patients diagnosed with oncocytoma on the initial biopsy cross to DI ( Table 1 ). Mean follow up time was shorter in the DI group (33 months vs. 45 months, P < 0.001). In a multivariate Cox regression, younger age, higher initial tumor size and higher growth rates were independently associated with higher likelihood for crossover to DI ( Supplementary Table 1 ).
During follow up, the overall mortality rate was 11%; none were cancer related.
4.3
Outcome analysis by growth rate and age
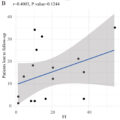
Clinical and radiologic characteristics of the SRM were compared based on the growth kinetics. Age, gender, cardiovascular risk factors were not associated with GR. Moreover, there was no difference in growth according to tumor composition (solid vs. cystic vs. solid-cystic). Only initial tumor size showed a statistically significant correlation with growth, with larger tumors having faster annual growth ( P = 0.015) ( Table 2 ).
Related posts:
 Is primary retroperitoneal lymph node dissection the way forward for patients with testicular seminoma and limited retroperitoneal metastases?
Is primary retroperitoneal lymph node dissection the way forward for patients with testicular seminoma and limited retroperitoneal metastases?
 Critical care therapy and in-hospital mortality after radical nephroureterectomy for nonmetastatic upper urinary tract carcinoma
Critical care therapy and in-hospital mortality after radical nephroureterectomy for nonmetastatic upper urinary tract carcinoma
 The clinical relevance of cut-off percentage for high-grade urothelial carcinoma within low-grade urothelial carcinoma: A determining factor?
The clinical relevance of cut-off percentage for high-grade urothelial carcinoma within low-grade urothelial carcinoma: A determining factor?
 Cumulative smoking exposure impacts oncologic outcomes of upper tract urothelial carcinoma
Cumulative smoking exposure impacts oncologic outcomes of upper tract urothelial carcinoma
 The fragility index of randomized controlled trials in advanced/metastatic renal cell cancer
The fragility index of randomized controlled trials in advanced/metastatic renal cell cancer
 Pathologic prostate cancer grade concordance among high-resolution micro-ultrasound, systematic transrectal ultrasound and MRI fusion biopsy
Pathologic prostate cancer grade concordance among high-resolution micro-ultrasound, systematic transrectal ultrasound and MRI fusion biopsy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


