Mononucleosis and Other Infectious Respiratory Illnesses
Mononucleosis and Other Infectious Respiratory Illnesses
Terrill D. Bravender
KEY WORDS
Community-acquired pneumonia
Epstein Barr Virus
Influenza
Mononucleosis
Mycoplasma pneumonia
Pertussis
INFECTIOUS MONONUCLEOSIS
Infectious mononucleosis (IM) is common in adolescents and young adults (AYAs). Usually, IM is an acute, self-limited, and benign lymphoproliferative disease caused by the Epstein-Barr virus (EBV). Although EBV is responsible for approximately 90% of cases, IM may also be caused by other infectious agents such as cytomegalovirus (CMV), toxoplasmosis, human herpes virus 6, and adenovirus.1
Etiology and Pathophysiology
EBV is a fragile, enveloped DNA herpes virus that cannot survive long outside of a host. Transmission occurs primarily through exposure to oropharyngeal secretions (hence its reputation as “the kissing disease”). EBV initially infects oral epithelial cells, then B lymphocytes, which spread the infection throughout the lymphoreticular system. There is a polyclonal B-cell proliferation with a significant T-cell response. The atypical white blood cells (WBCs) that are frequently seen on peripheral blood smears are mainly CD8 cytotoxic or suppressor cells. The immune response accounts for many of the clinical manifestations of IM such as lymphadenopathy and hepatosplenomegaly. Although a large number of B lymphocytes are infected, these are initially resting memory cells, which do not proliferate and thus have no oncogenic potential. For 3 to 4 months following acute infection, the number of infected cells decreases, but some infected cells continue to circulate indefinitely. Individuals remain infected for life, and 60% to 100% of seropositive, asymptomatic individuals intermittently shed EBV in an unpredictable fashion. EBV is present in the oropharyngeal secretions of up to 20% of asymptomatic adults. Over time, EBV infection of B cells may lead to cell transformation and establishment of lymphoblastoid cell lines. Such transformation occurs rapidly in vitro; in vivo, host immunity plays a critical role in containing the latent infection. Although multiple strains of EBV exist, it appears that a single episode of IM confers lifelong immunity, likely because the majority of patients are infected with multiple strains at the same time.
Epidemiology
Over 90% of adults have serologic evidence of past EBV infection. The highest rates of acute infection in the US are in older AYAs, particularly those living in close proximity to one another, such as in college or the military.
Age
Between 30% and 40% of AYAs who contract EBV will develop the symptoms of IM. About half of children have contracted EBV prior to age 5, when the infection is usually asymptomatic. Over 90% of adults have evidence of past infection. In the US, the annual incidence of IM for those between age 15 and 19 is 345 to 671 cases per 100,000 person-years. In contrast, the incidence for individuals aged 35 and older is only 2 to 4 cases per 100,000 person-years.
Gender
There are no gender differences in prevalence.
Race
In the US, IM is more prevalent among Whites than Blacks, likely reflecting earlier acquisition of EBV in Black children.
Season
There is no seasonal variation.
Household Contacts
An infected individual will transmit EBV to about half of susceptible household contacts. Exposure to an individual with acute infection may induce increased asymptomatic viral shedding in seropositive contacts.
Clinical Manifestations
The majority of EBV infections are either asymptomatic or associated with mild, nonspecific symptoms such as malaise, fever and chills, and anorexia. In those who develop IM, there is an incubation period of 4 to 7 weeks, after which there may be a 3- to 5-day prodrome of malaise, fatigue, headaches, anorexia, and myalgias. The traditional triad of IM includes the following:
Fever, lymphadenopathy, and pharyngitis
Lymphocytosis with atypical lymphocytes
Antibody response demonstrated by the presence of heterophile or EBV-specific antibodies
Signs and Symptoms
The common presentation includes fever, which may persist for several weeks, and sore throat, which can be severe and is associated with an exudative pharyngitis in up to 50% of individuals. Adenopathy is usually significant and is usually symmetrical, with posterior cervical lymph nodes more prominent than anterior. Splenomegaly and hepatomegaly may occur by the second week of the illness. Approximately 10% of individuals have a rash that may take on a number of different appearances—erythematous, maculopapular, morbilliform, urticarial, or erythema multiforme. Signs and symptoms are summarized in Table 29.1. Approximately 90% of patients who receive ampicillin or amoxicillin will develop an erythematous, maculopapular rash that typically appears about one week after starting antibiotics. Although the exact mechanism for the development of this rash is unknown, it appears that a true drug sensitization does occur in these patients. Whether this sensitization persists following resolution of IM is unknown.
TABLE 29.1 Symptoms and Signs of Infectious Mononucleosis
aRisk of rash is higher if exposed to ampicillin or amoxicillin.
Complications
Complications of IM are summarized in Table 29.2. Overall, the complication rate of IM is approximately 1% to 2%. Occasionally, patients will present with a major complication as their only manifestation of the disease. The typical clinical symptoms may not appear until later in the course of the illness.
Specific Complications
Splenic Rupture: Splenic rupture is seen in approximately 0.1% to 0.2% of cases of IM. At least half of cases are spontaneous without any history of trauma or unusual physical exertion. Typically, there is abrupt abdominal pain in the left upper quadrant that radiates to the top of the left shoulder, known as Kehr sign. This is followed by generalized abdominal pain, pleuritic chest pain, and signs and symptoms of hypovolemia. However, the onset may be insidious. Splenic rupture occurs between days 4 and 21 of the illness, with approximately half of cases occurring during the peak of the acute illness. Only about half of cases of splenic rupture have clinically significant splenomegaly noted before the rupture. All patients with IM should be considered at risk for splenic rupture, because clinical severity, laboratory results, and physical examination are not reliable predictors of risk.2
TABLE 29.2 Potential Complications of Infectious Mononucleosis
Complication
Prevalence
Neurological:
<1%
Seizures
Facial or peripheral nerve palsies
Meningoencephalitis
Aseptic meningitis
Optic neuritis
Reye syndrome
Coma
Brachial plexus neuropathy
Transverse myelitis
Guillain-Barré syndrome
Acute psychosis
Acute cerebellar ataxia
“Alice in Wonderland” syndrome
Hematological:
Autoimmune hemolytic anemia (mild)
Thrombocytopenia purpura
Coagulopathy
Aplastic anemia
Hemolytic-uremic syndrome
Eosinophilia
Profound thrombocytopenia
0.5%-3%
Rare
Rare
Rare
Rare
Rare
Rare (Mild thrombocytopenia is common.)
Cardiac:
1.7%-6%
Pericarditis
Myocarditis
Electrocardiogram changes (nonspecific ST and T-wave abnormalities)
Splenic rupture
0.1%-0.2%
Pulmonary:
Airway obstruction
Pneumonitis
Pleural effusions
Pulmonary hemorrhage
Rare (more common in young children)
Rare
Rare
Rare
Gastrointestinal:
Mild elevation of hepatocellular enzymes
Pancreatitis
Hepatitis with liver necrosis
Malabsorption
80%-90%
Rare
Rare
Rare
Dermatological:
3%-10%
Dermatitis
Urticarial rash (may be cold-induced)
Erythema multiforme
Renal:
Glomerulonephritis
Nephrotic syndrome
Mild hematuria or proteinuria
Rare
Rare
Up to 13%
Ophthalmological:
Rare
Conjunctivitis
Episcleritis
uveitis
Other:
Uncommon
Bullous myringitis
Orchitis
Genital ulcerations
Parotitis
Monoarticular arthritis
Airway Obstruction: Airway obstruction is an uncommon but life-threatening complication of IM related to massive lymphoid hyperplasia and mucosal edema. It is more common in younger adolescents and typically occurs approximately 1 week after the initial symptoms begin. Corticosteroids have been used to reduce the edema and hypertrophy of the lymphoid tissue. In more severe cases, acute tonsillectomy may be indicated. In emergency situations, intubation or tracheostomy may be necessary.
Streptococcal Pharyngitis: It was previously thought that EBV infection could potentiate adherence of β -hemolytic streptococci to epithelial cells membranes, with older reports identifying co-infection rates as high as 33%. More recent studies report a co-infection rate of 4%, which is the same as the general population.
Laboratory Evaluation
Antibody Testing
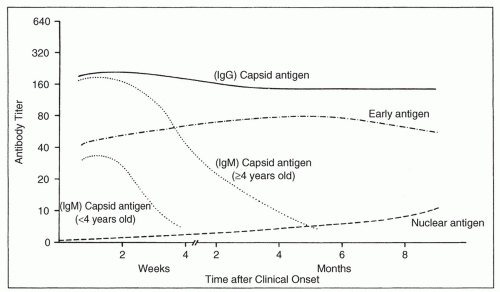
The standard rapid test for EBV-associated IM is the presence of heterophile antibodies. These immunoglobulin M (IgM) antibodies are induced by EBV infection and cross-react with unrelated antigens, typically horse, sheep, or bovine erythrocytes. These rapid test kits have sensitivities of 78% to 84% and specificities of 89% to 100% when compared to EBV-specific serologies, but sensitivity is lower (<50%) in children under 12 years of age. Sensitivity is also lower during the first week of symptoms; heterophile antibody levels peak between weeks two and five of the illness. About 10% of AYAs with EBV will remain heterophile antibody negative, but may be diagnosed by detection of EBV viral capsid antigen (VCA) IgM. Both IgM and immunoglobulin G (IgG) VCA antibodies peak 3 to 4 weeks after symptom onset. IgM levels then decline rapidly and are undetectable by 3 months. Although VCA-IgG levels also decline, they are usually detectable for life. EBV early antigen (EA) antibodies develop early in the infection and usually persist for 1 to 2 months, although as many as 30% of infected individuals will have persistently high levels. Finally, about 2 to 3 months after symptom onset, antibodies against EBV nuclear antigen (EBNA) develop and persist indefinitely.4Figure 29.1 shows the characteristic EBV antibody responses to various EBV antigens. Table 29.3 shows the pattern of serologic results in various EBV stages.
FIGURE 29.1 The evolution of antibodies to various EBV antigens in patients with IM is shown in the figure. The titers are geometric mean values expressed as reciprocals of the serum dilution. IgM and IgG antibody responses to EBV capsid antigen develop during the acute phase, as does an IgG response to EBV EA in most cases. The IgG response lasts for life, but the IgM response is transient and is shortest in very young children. Antibody response to nuclear antigen lasts for life and is typically quite late in onset. (From Sumaya CV. Epstein-Barr serologic testing: diagnostic indications and interpretations. Pediatr Infect Dis 1986;5:337.)
Complete Blood Count
The WBC differential provides the traditional diagnostic criteria for IM >50% lymphocytes and at least 10% of the differential composed of atypical lymphocytes. The total WBC count is often elevated in the range of 10,000 to 20,000/mm3. Other common hematological abnormalities include a mild granulocytopenia and thrombocytopenia (usually in the range of 100,000 to 140,000/mm3) in approximately half of individuals with IM. Anemia is uncommon, although a mild hemolytic anemia may occur in up to 3% of cases.
Hepatic Transaminases
Transaminase levels are elevated in at least 90% of individuals, peaking during the second or third week of symptoms. Mild hepatitis is so common that entirely normal hepatic transaminases should lead the clinician to consider a diagnosis other than EBV infection.
Epstein-Barr Viral Detection
Serum-based EBV DNA nucleic acid amplification tests have been developed, and the magnitude of the viral load has been correlated with severity of illness. However, EBV viral load tests are not readily available for clinical use, and the primary use of these tests has been in immunocompromised patients at risk for EBV-associated malignancy.
Differential Diagnosis
In addition to other causes of EBV-negative mononucleosis such as CMV, toxoplasma gondii, rubella, adenovirus, and acute human immunodeficiency virus (HIV) infection, the differential diagnosis includes group A β-hemolytic streptococcal pharyngitis, nonspecific viral tonsillitis, mycoplasma pneumonia, Vincent angina (necrotizing ulcerative gingivitis), diphtheria, viral hepatitis, and lymphoproliferative disorder or leukemia.
TABLE 29.3 Patterns of EBV Serology
Early Antigen
Types of Infection
Heterophile Antibody
VCA-IgG
VCA-IgM
D-EA
R-EA
EBNA
Susceptible (nonimmune)
–
–
–
–
–
–
Acute primary infection
+
++
+
+
–
–
Remote past infection
–
+
–
–
–
+
Reactivated infection
+/-
+++
–
+
++
+/-
D-EA, diffuse early antigen; EBNA, Epstein-Barr nuclear antigen; Ig, immunoglobulin; R-EA, restricted early antigen; VCA, viral capsid antigen.
Only gold members can continue reading. Log In or Register to continue