Miscellaneous Rare Lesions
A wide variety of reactive, benign, and malignant lesions occurring elsewhere in the body have been described in the breast. This chapter will focus on a few of these rare entities that are well-documented and that must be distinguished from more commonly encountered breast lesions.
AMYLOID TUMOR
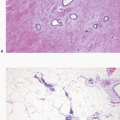
Amyloid deposits may be seen in the breast of patients with predisposing systemic diseases. Primary amyloid tumors limited to the breast are rare.1 Patients present with a painless mass, which is typically 2 to 3 cm in size. Grossly, amyloid tumors are usually single nodules that have a firm, gray or white, shiny cut surface. Microscopic examination reveals the characteristic eosinophilic, homogenous deposits of amyloid in fibroadipose tissue, in vessel walls, and in and around ducts and lobules. The latter is associated with atrophy and obliteration of these glandular elements. Calcifications may be present.1,2 Careful clinical evaluation is required to distinguish between primary and secondary amyloid deposition. Treatment is by excisional biopsy.
WEGENER GRANULOMATOSIS
Wegener granulomatosis presenting in the breast is unusual. Most patients have other evidence of this systemic disease. Within the breast, Wegener granulomatosis usually presents as a tender mass that may involve the overlying skin, which suggests inflammatory carcinoma. If a surgical excision is performed, the typical features of necrotizing vasculitis are seen, along with acute and chronic inflammation of the breast stroma. Areas of infarction may be present with granulomas at the periphery of the infarcted areas.3,4 This lesion must be distinguished from
other more common causes of inflammation and granuloma formation (see Chapter 2).
other more common causes of inflammation and granuloma formation (see Chapter 2).
TUMORS OF LYMPHOID AND HEMATOPOIETIC CELLS
Lymphoma
Lymphomas in the breast may be due to secondary involvement by disseminated lymphoma or may represent a primary lesion. Secondary mammary involvement by lymphoma should be excluded before a diagnosis of primary breast lymphoma is made.
Primary lymphomas of the breast are uncommon, accounting for <1% of all malignant mammary neoplasms. They typically appear grossly as circumscribed masses, with a tan-white, fleshy cut surface. Foci of hemorrhage or necrosis may be present.
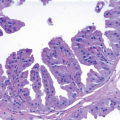
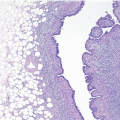
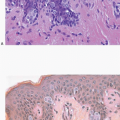
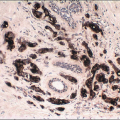
On histologic examination, primary breast lymphomas are almost always of non-Hodgkin type, but Hodgkin disease may rarely involve the breast as well.5,6 Among the non-Hodgkin lymphomas, diffuse large B-cell lymphoma is the most common type.5,7,8 but other categories of lymphomas have also been reported to occur as primary lesions in the breast including Burkitt lymphoma (which may present with massive bilateral breast enlargement),5 extranodal marginal B-cell lymphomas arising from mucosa-associated lymphoid tissue (MALT lymphomas),5,9,10 follicular lymphomas (Fig. 14.1, e-Fig. 14.1), lymphoblastic lymphomas, T-cell lymphomas,11 and most recently implant-associated anaplastic large cell lymphomas (ALCLs; see subsequent text).12, 13, 14, 15 and 16
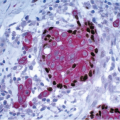
Large cell lymphomas must be distinguished from poorly differentiated carcinomas, including invasive carcinomas with medullary features. In addition, some lymphomas have an appearance reminiscent of the solid variant of invasive lobular carcinoma.17 In cases in which the lymphoma cells are arranged in a linear pattern or cords, the appearance may resemble the classical type of invasive lobular carcinoma. In problematic cases, immunostains for lymphoid and epithelial markers and hormone receptors are valuable adjuncts for arriving at the correct diagnosis. Low-grade lymphomas must be distinguished from chronic inflammatory infiltrates, such as those seen in lymphocytic mastopathy (see Chapter 2) and from intramammary lymph nodes.
Implant-associated ALCL is a recently described primary T-cell lymphoma of the breast occurring in women with prosthetic implants.12, 13, 14, 15 and 16




Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
