Screen for secondary causes of low bone mineral density.
Correct vitamin D deficiency and insufficiency prior to initiating other treatments for osteoporosis.
As the population in the United States ages, we can expect practitioners to encounter an increasing number of patients with metabolic bone disease and associated low bone mass. These disorders are usually divided into primary and secondary causes of low bone mass (see Table 23.1). The most common types of metabolic bone disease—including (i) osteoporosis; (ii) osteomalacia; (iii) primary hyperparathyroidism; and (iv) renal osteodystrophy—will be discussed in this chapter. Recognizing the presence of these bone disorders is a major challenge for physicians. These abnormalities of the bone and calcium/phosphorus metabolism are usually silent until well advanced and present with complications of the disease, most commonly, fracture. Therefore, a high level of suspicion and a clear plan for the screening of high-risk patients can have a significant impact on quality of life and society’s health care costs.
OSTEOPOROSIS
Osteoporosis is defined as a skeletal disorder characterized by low bone density and poor bone quality that lead to an increased risk of fragility fractures. Primary or involutional osteoporosis refers to the normal bone loss that occurs with aging. This can be further subdivided into type I or II osteoporosis syndromes. Type I is characterized by the rapid bone loss observed in the first 15 to 20 years after menopause, with a disproportionate trabecular over cortical bone loss. During this accelerated rate of bone loss, women may lose as much as 20% to 30% of trabecular bone and 5% to 10% of cortical bone and are at increased risk of Colles fractures and vertebral compression fractures. Type II or senile involutional osteoporosis refers to the slow phase of age-related bone loss and leads to equal losses of cortical and trabecular bones. This type of osteoporosis affects the entire population and is progressive throughout aging. This results in an increase in fracture risk in people at the lower end of the age-specific distribution for bone mineral density (BMD). Clinically, this type of osteoporosis presents with predominantly proximal femur and vertebral fractures, but fractures at other sites with a combination of cortical and trabecular bones can also be seen.
Type I osteoporosis has been widely believed to be a result of low estrogen concentration in menopause. While this is certainly a primary factor, estrogen deficiency leads to an increase in certain cytokines such as interleukin-6 and tumor necrosis factor as well as an increase in urinary calcium excretion. It is probably the genetically determined susceptibility to these factors in the bone and kidney that determines, to a great extent, the degree of observed bone loss. On the other hand, type II osteoporosis is believed to be the result of a combination of secondary hyperparathyroidism and decreased bone formation rates, and both processes are a consequence of lower estrogen concentration in aging women and men.
TABLE 23.1 SECONDARY CAUSES OF LOW BONE MASS
Endocrine Disorders
Hematopoietic Disorders
Hyperparathyroidism (252.00)
Multiple myeloma (203.00)
Vitamin D insufficiency or deficiency (268.9)
Sickle cell disease (282.60)
Hyperthyroidism (242.90)
Thalassemia (282.49)
Cushing syndrome (255.0)
Metastatic carcinoma
Hyperprolactinemia (253.1)
Systemic mastocytosis (202.60)
Hypogonadism—female (256.39) male (257.2)
AIDS/HIV (042)/(V08)
Pregnancy and lactation
Leukemia and lymphoma 10.60/202.80
Nutritional and Gastrointestinal Disorders
Lipidoses: Gaucher disease (272.7)
Malabsorptive syndromes (579.9)
Drug-Induced
Bariatric surgery
Alcohol
Total parenteral nutrition
Glucocorticoids
Gastrectomy
Anticonvulsants
Hepatobiliary disease
Heparin
Renal Disorders
Lithium
Renal osteodystrophy (588.0)
Cyclosporine
Renal tubular acidosis (588.89)
Gonadotropin-releasing hormone agonists
Hypercalciuria (275.40)
Aluminum
Connective Tissue Disorders
Smoking
Rheumatoid arthritis (714.00)
Miscellaneous
Osteogenesis imperfecta (756.51)
Immobilization
Ehlers-Danlos syndrome (756.83)
Reflex sympathetic dystrophy (337.20)
Homocystinuria (270.4)
Weight loss (783.21)
Lysinuria (270.9)
Multiple sclerosis (340)
Ankylosing spondylitis (720.0)
Porphyria (277.1)
Marfan syndrome (759.82)
AIDS, acquired immunodeficiency syndrome; HIV, human immunodeficiency virus.
While the clinical hallmark of osteoporosis is the presence of low-trauma fractures, this precludes diagnosis in individuals who may be at high risk for fracture and in whom fracture prevention should be the standard of care. Therefore, in 1994, the World Health Organization (WHO) offered a definition of osteoporosis on the basis of bone density measurements and history of fracture (see Table 23.2). These criteria designate osteoporosis as a BMD equal to or <2.5 standard deviations (SDs) below a young mean adult value. On the basis of the WHO criteria, 20% to 30% of postmenopausal women in the United States have osteoporosis, and 1.3 million fractures a year are attributable to this disease. The WHO criteria were originally developed to describe fracture risk in white postmenopausal women. Whether the same criteria can be applied to other populations, particularly in men, is still an area of much controversy. Nonetheless, in recent years, the International Society for Clinical Densitometry (ISCD), in association with an expert panel, determined that it is appropriate to apply the same criteria to men while using a gender-specific database for BMD. Using these established cutoffs, it is estimated that 1 to 2 million men have osteoporosis and 8 to 13 million have osteopenia. The respective age-adjusted prevalence figures are 6% and 47%. If one uses fracture as a clear endpoint, then the estimated lifetime risk is 13% to 25%. Either way, this is a significant health problem for both aging women and men.
Morbidity and mortality following a vertebral or hip fracture are high. Vertebral fractures lead to a progressive decrease in physical activity, kyphotic deformity, height loss, and chronic back pain, all of which, in turn, cause increasing social isolation, depression, and low self-esteem. The 5-year age-matched survival after a vertebral fracture is 72% for men and 84% for women. Similarly, a hip fracture leads to significant disability. One year after a hip fracture, 40% of patients are unable to walk independently and 60% require assistance with activities of daily living. Hip fracture mortality is higher in men than in women. Approximately 8% of men and 3% of women over age 50 die during their initial hospitalization for hip fracture. One year after a hip fracture, the mortality is 36% for men and 21% for women. Therefore, the challenge is to recognize individuals who are at high risk for osteoporotic fractures before the first fracture occurs. While it is recognized that for every 1 SD decrease in BMD there is an associated two- to threefold increase in fracture risk, 50% of patients who suffer a fragility fracture have a BMD above the osteoporosis threshold as defined by the WHO criteria. Case-finding strategies should therefore incorporate the known risk factors for fracture, and treatment decisions should be based not only on the BMD scores but also on risk factor assessment.
TABLE 23.2 DEFINING OSTEOPOROSIS BY BONE MINERAL DENSITY ON THE BASIS OF THE WORLD HEALTH ORGANIZATION CRITERIA
Category
Definition by BMD
Normal
BMD is within 1 SD from a young healthy adult (T-score greater than or equal to −1.0)
Osteopenia
BMD is between 1 and 2.5 SD below that of a young healthy adult (T-score between −1 and −2.5)
Osteoporosis
BMD is 2.5 SD or more below that of a young healthy adult (T-score at or below −2.5)
Severe osteoporosis (established)
BMD >2.5 SD below that of a young adult mean in the presence of one or more fragility fractures
BMD, bone mineral density; SD, standard deviation.
World Health Organization 1994.
Workup/Keys to Diagnosis
The first step in assessing fracture risk is a thorough assessment of clinical risk factors (see Table 23.3). The most important, readily recognized factor is probably age. It is well known that for any given BMD, the fracture risk increases with aging. For example, the risk of hip fracture increases 30-fold between the ages of 50 and 80, while one would predict a fourfold increase solely on the basis of the average BMD. Other significant risk factors for fracture that capture aspects of risk beyond that assessed by BMD include previous fragility fracture, glucocorticoid therapy, family history of fragility fracture, and low body weight, among others. Utilizing this risk factor assessment, one can therefore identify a subgroup of patients for whom the risk of a future fracture is high enough to warrant therapy, regardless of the baseline BMD. In these patients, BMD may still be utilized to monitor their response to therapy. On the other hand, individuals with a paucity of risk factors may not warrant BMD testing because their fracture risk is low, regardless of bone density measurements. Therefore, the National Osteoporosis Foundation (NOF) has provided a set of guidelines to aid practitioners in identifying patients for whom BMD testing is appropriate (see Table 23.4). These and similar guidelines issued by Medicare and the ISCD are not all encompassing and, therefore, should be used in the context of a patient’s particular situation.
TABLE 23.3 RISK FACTORS FOR OSTEOPOROTIC FRACTURES
Major Risk Factors in White Women
Personal history of fracture as an adult
History of fragility fracture in a first-degree relative
Low body weight (<58 kgs)
Current smoking
Use of oral corticosteroid therapy for >3 mo
Additional Risk factors
Premature menopause (<45 y)
Primary or secondary amenorrhea
Primary and secondary hypogonadism in men
Impaired vision
Prolonged immobilization
Dementia
Excessive alcohol consumption (>2 drinks/d)
Low calcium intake
Recent falls
Poor health/frailty
BMD testing remains a cornerstone of osteoporosis diagnosis and assessment of response to treatment. Central dual x-ray absorptiometry (DXA) is the standard for BMD testing. Central DXA has been used extensively in epidemiologic studies and, therefore, its relationship to fracture risk has been best characterized. Fracture prediction at a specific site is most accurate for BMD measurements at that particular site. For instance, BMD at the hip correlates best with hip fracture risk, although a general fracture risk assessment can be estimated from the measurement at any site. Quantitative computed tomography (QCT) of the spine is another central modality for bone density measurement. The greatest advantage of this technology is that it provides a true volumetric assessment of bone density, while DXA only provides an areal density. QCT requires specific software, and it has not been traditionally used in epidemiologic studies or longitudinal studies of treatment effect. Furthermore, QCT results in a high radiation exposure, far in excess of that observed with DXA. This technology may best be used in patients at the extremes of size or weight.
TABLE 23.4 WHO SHOULD BE TESTED
National Osteoporosis Foundation
All women aged 65 and older, regardless of risk factors
Younger postmenopausal women with one or more risk factors (other than being white, postmenopausal, and female)
Postmenopausal women who are considering therapy if BMD testing would facilitate the decision
Postmenopausal women who present with fractures (to confirm the diagnosis and determine the disease severity)
Medicare Coverage for BMD in Individuals Aged 65 and Older—Bone Mass Act
Estrogen-deficient women at clinical risk for osteoporosis
Individuals with vertebral abnormalities
Individuals receiving, or planning to receive, long-term glucocorticoid (steroid) therapy
Individuals with primary hyperparathyroidism
Individuals being monitored to assess the response or efficacy of an approved osteoporosis drug therapy
BMD, bone mineral density.
Peripheral technologies such as pQCT, pDXA, and quantitative ultrasound (QUS) are increasingly being used for screening purposes. The WHO criteria should not be applied to these measurements and, therefore, it is recommended that anyone with a positive study undergoes central DXA measurement. Furthermore, sites traditionally measured by these methods respond poorly to osteoporosis treatment, and it is recommended that central sites be used to assess response to therapy. On the other hand, peripheral BMD does provide an assessment of global fracture risk, as recently demonstrated in two large prospective studies, and may therefore serve as a cost-effective initial screening tool.
While osteoporosis has few diagnostic signs in physical examination, there are a number of findings that can alert the practitioner to the possibility of disease and/or an increased fracture risk. Poor visual acuity and depth perception, decreased proprioception, decreased proximal muscle strength, and an impaired “get up and go” test are all risk factors for fall and fracture and can be easily assessed in the clinic. Furthermore, kyphotic deformities of the spine are late sequelae of vertebral fractures and should prompt the physician to pursue further diagnosis and treatment.
We recommend that all patients diagnosed with osteoporosis undergo basic laboratory testing for secondary causes of osteoporosis. These tests should include, at a minimum, the measurement of calcium, phosphorus, magnesium, creatinine, parathyroid hormone (PTH), and 25(OH) vitamin D levels. The prevalence of vitamin D deficiency in the elderly population is estimated to be between 25% and 54%. This number is probably even higher for institutionalized or debilitated individuals. Vitamin D deficiency may, in turn, lead to secondary hyperparathyroidism and its associated adverse effects on bone. Therefore, vitamin D deficiency should be routinely screened for and aggressively treated. All men should have a serum testosterone measurement because treatment of hypogonadism may result in increased bone mass. In addition, other tests such as serum and urine protein electrophoresis and screening tests for hypercortisolism or malabsorptive syndromes should be obtained in select patients. Finally, whether to measure 24-hour urine excretion for calcium is controversial. There is high variability in calcium urine excretion from day to day and this is at least partly related to dietary variability. This is useful when calcium malabsorption is a significant issue and may result in a therapeutic change. We have also identified a significant number of patients with idiopathic hypercalciuria, which has been associated with secondary hyperparathyroidism and low BMD. Such patients may benefit from treatment with thiazide diuretics to reduce renal calcium excretion.
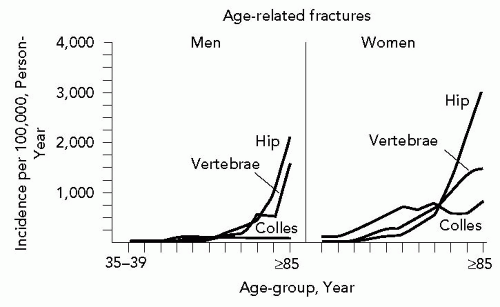
As previously outlined, treatment decisions should be based on a combination of clinical risk factor assessment and BMD measurement. NOF recommends that treatment should be considered in postmenopausal women with a T-score of < − 2.0 or in women with a T-score of < − 1.5 but with other risk factors. These criteria have also been extrapolated to men. However, in the absence of other risk factors, treatment based solely on BMD should be reserved for men older than 65 to 70 years of age, because this is when fracture risk increases in this population (see Fig. 23.1).
Management
The management of osteoporosis is multifactorial and includes a combination of lifestyle modifications, nutritional counseling, and pharmacologic interventions. As described in the preceding text, the first step in osteoporosis management entails screening for secondary causes of osteoporosis and correcting as indicated.
Lifestyle interventions are crucial in the treatment of osteoporosis, but perhaps more importantly, in fracture prevention. All patients should be advised to pursue a combination of weight-bearing exercises and strength training. Exercise serves to decrease osteoporosis and fracture risk in several important ways. Low impact to bone stimulates bone remodeling with the uptake of old, possibly fragile, bone and the deposition of new, stronger bone. In addition, exercise increases balance and muscle strength and, therefore, decreases the risk of falls. Patients with severe mobility impairment should be referred to physical therapy for instruction on appropriate exercises and balance training. All patients should be advised to pursue fall prevention measures at home including (i) proper lighting in all rooms; (ii) removal of area rugs and floor clutter; (iii) use of walking devices as deemed appropriate; and (vi) avoidance of uneven walking surfaces. In addition, patients should be advised against smoking and excessive alcohol use, because both these have been shown to have detrimental effects on bone metabolism.
Figure 23.1 Fracture incidence for men and women with aging. (Reproduced from Cooper C. Epidemiology of osteoporosis. In: Favus M, ed. The Primer on the metabolic bone diseases and disorders of mineral metabolism, 5th ed. Washington, DC: American Society for Bone and Mineral Research; 2003:307-313 with permission of the American Society for Bone and Mineral Research.)
Nutritional counseling plays a central role in the treatment of osteoporosis. Most adult Americans do not consume the currently recommended daily allowances of calcium and vitamin D. It is estimated that <1 in 100 women over the age of 70 and <25% of men in any age-group meet the daily dietary calcium requirements. The numbers are similar for vitamin D consumption. In the clinic, we encounter a large number of patients with superimposed osteomalacia due to vitamin D deficiency and consequent bone mineralization defects. The treatment of vitamin D deficiency will be discussed in more detail in the subsequent text, but, in general, the goal is to maintain a 25(OH) vitamin D concentration of 30 ng per mL or greater. The recommended daily intake of calcium and vitamin D in adults varies greatly worldwide. It is the current consensus that all patients with a diagnosis of osteoporosis should be advised to take 1,500 mg of calcium and 800 to 1,000 IU of vitamin D daily. These daily requirements should be met by a combination of foods high in these nutrients and dietary supplements. In general, calcium is poorly absorbed in the gut. It is therefore important to recognize that not all dietary supplements have been tested for absorption efficiency. Calcium carbonate, the most commonly used supplement, is best absorbed with food. Because the calcium-absorbing capacity of the gastrointestinal tract is limited, not more than 500 mg of calcium should be ingested at one time. It is best to spread calcium and vitamin D supplementation throughout the day. Studies of calcium and vitamin D supplementation have shown a reduction of fractures at all sites, including the hip (Evidence Level A).1,2 In addition, other minerals are known to have both direct and indirect effects on bone. Magnesium deficiency is also a common problem in the US population. Magnesium is important in the regulation of PTH secretion, and, therefore, a goal of the treatment should be to maintain normal magnesium levels.
Finally, pharmacologic therapy remains the mainstay of therapy for osteoporosis. There are several general classes of medications available for both osteoporosis prevention and treatment. These include hormone therapy (HT); selective estrogen receptor modulators (SERMs); calcitonin; bisphosphonates, and recombinant human PTH (hPTH).
HT: This has been shown to be efficacious in trials of both osteoporosis prevention and treatment, with measured increases in BMD at the spine, hip, and forearm (Evidence Level A). Analysis of these trials by estrogen dose have shown persistent increases in BMD with the use of low-dose estrogen (equivalent to Premarin 0.3 mg), albeit more modest than those observed with high-dose therapy.3 The results of the Women’s Health Initiative showed a 23% reduction in all fractures and a 34% reduction in hip and vertebral fractures after an average of 5.2 years of HT.4 Therefore, HT is currently recommended for osteoporosis prevention in high-risk women who have no known contraindications to HT use. However, given the increasing number of alternative therapies for osteoporosis and the potential side effects of long-term HT, the use of these agents should be approached cautiously with a plan for only short-term use in postmenopausal women.
SERMs: These compounds bind with high affinity to the estrogen receptor and may act as an estrogen agonist or antagonist, depending on the specific type of estrogenresponsive tissue. Tamoxifen has been used for many years for the treatment of estrogen receptor-positive breast cancer. In trials of breast cancer treatment and prevention, tamoxifen was shown to act as an estrogen agonist at the level of the bone, with observed increases in bone density. Raloxifene, as tamoxifen, has been shown to act as an estrogen agonist in bone. Raloxifene has been approved for the treatment and prevention of postmenopausal osteoporosis. The currently approved daily dose of 60 mg has been shown to increase BMD at the spine, hip, and the total body after 2 years of treatment (Evidence Level A).5 There is also an associated decrease in bone-turnover markers, with restoration to premenopausal levels. Most importantly, in the Multiple Outcomes of Raloxifene Evaluation (MORE) trial, a large placebo-controlled trial including 7,705 postmenopausal women, raloxifene was shown to decrease clinical vertebral fractures by 62% after 1 year of treatment.6 On the other hand, there was no significant decrease in the rate of nonvertebral fractures after the original 36-month study or after the 1-year extension. The safety profile of raloxifene is quite favorable. However, in the MORE trial, there was an increased risk of thromboembolic disease similar to that observed with HT. On the other hand, given the low incidence of this complication, the attributable risk is still very low.
Calcitonin: This acts as a hypocalcemic factor by its inhibitory effect on osteoclast resorption. This 32-amino acid peptide is secreted by the C cells of the thyroid, but its exact physiologic role in calcium homeostasis is still unknown. Salmon calcitonin is available in a parenteral and a nasal spray formulation for the treatment of women with osteoporosis for more than 5 years postmenopause. While only very modest increases in BMD of 1% to 2% at the lumbar spine have been shown with the use of nasal calcitonin in postmenopausal women, the Prevent Recurrence of Osteoporotic Fractures trial in women with osteopenia (T < −2.0) of the spine showed a 33% reduction in vertebral risk when compared to placebo (Evidence Level B).7 This effect was only observed with a dose of 200 IU a day but not with the doses of 100 or 400 IU. No increase in BMD or decrease in fracture of the hip or other sites has been demonstrated with the use of any calcitonin preparation. Calcitonin is probably unique among osteoporosis treatments in that it has an analgesic effect on bone pain after an acute vertebral fracture, and it is therefore used at times for this indication. The most common side effect with the use of nasal calcitonin is a higher incidence of rhinitis and/or epistaxis. Injectable calcitonin may cause flushing, nausea, and vomiting. In clinical practice, the use of calcitonin has been reserved for the treatment of patients with acute bone pain or those who are intolerant to other approved osteoporosis therapies.
Only gold members can continue reading. Log In or Register to continue