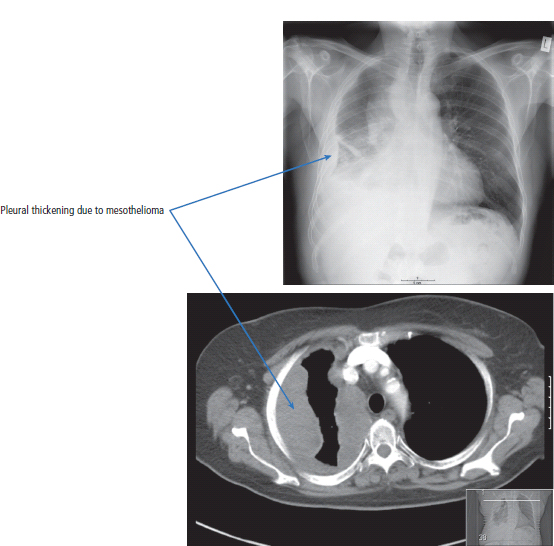
27 Stephen Jay Gould was an evolutionary paleontologist at Harvard University and a prolific essayist. In 1982, he was diagnosed with peritoneal mesothelioma, which had a quoted median survival of 8 months. In response to this information he wrote an essay entitled “The median is not the message”, which wisely and humanely explains the statistics of cancer survival. We urge students and patients to read it. Gould survived a further 20 years, dying in 2002 of a second primary lung cancer. In 2011, 2540 people were diagnosed and 2310 died of mesothelioma in the United Kingdom (Table 27.1). Three quarters of all mesotheliomas are pleural in origin and the remainder are peritoneal or pericardial. This tumour was originally described by occupational health doctors working in the asbestos factories in the East End of London around the time of the end of the First World War. It would appear, however, that this information was suppressed, and it was not until the 1960s that the association between mesothelioma and asbestos exposure was clearly publicized. The incidence of mesothelioma rose markedly in the last quarter of the 20th century and appears to mirror asbestos exposure rates 20–30 years previously. In the 1970s, after the risk of exposure was recognized, rigorous controls on the handling of asbestos were introduced in the United Kingdom. For this reason the rate of rise of mesothelioma is expected to peak in 2015 and decline thereafter. But this is a global problem and touches countries all over the world from North Korea to South Africa. The development of mesothelioma is generally related to asbestos exposure, but this may not always be the case. The risk of mesothelioma is not related to the amount of exposure. It may not only occur in the asbestos workers but also in family members exposed to the fibres of asbestos brought home in their spouse’s, father’s or mother’s clothes. There are no specific chromosomal changes associated with the development of mesothelioma, but there are a host of abnormalities that may occur, which are entirely non-specific. Different asbestos fibres have different properties and carcinogenicity. The most carcinogenic fibres tend to be the needle-shaped blue (crocidolite) and brown (amosite) asbestos rather than the commoner corkscrew-shaped white asbestos (chrysotile) (Table 27.2). Mesothelial tumours take their origins in the pleura or peritoneum.Patients with mesothelioma characteristically present with pleural effusions or ascites. Table 27.1 UK registrations for mesothelioma cancer 2010 The diagnosis of mesothelioma may be suspected from a chest X-ray (Figure 27.1), where a patient may have pleural plaques and an effusion. CT scanning will show the extent of the pleural or peritoneal tumour. The next step in the investigatory process is to carry out a pleural or peritoneal biopsy. Multiple biopsies are frequently needed to make the diagnosis, and video-assisted thoracoscopy (VATS) may be required. A further complication of invasive diagnostic procedures for mesothelioma is the risk of seeding the tumour along the biopsy site resulting in chest wall recurrences. This risk can be reduced by prophylactic radiotherapy to the biopsy track or scar. Recurrent effusions are a dramatic problem for patients, and the intervention of a thoracic surgeon may be required to strip the pleura and provide an effective pleurodesis. Possibly the most important aspect of the care of patients with mesothelioma is to ensure that the appropriate compensatory mechanisms are put in place. In the United Kingdom, industrial compensation is usually arranged for patients by their union officers and involves an examination of the tumour by a pathology panel. It is enormously important for the patient and his or her family that the clinician signposts this process. In the United Kingdom, two possible benefits are available: compensation from an employer linked to exposure to asbestos and industrial injuries disablement benefit from the Department of Works and Pensions. Unfortunately, the majority of patients with mesothelioma present with incurable disease. Treatment options are limited. Chemotherapy is generally ineffective, with response rates in the order of less than 10%, although newer combinations of cisplatinum and permetrexed (a dihydrofolate reductase inhibitor) offer promise. Radiation therapy may be helpful in controlling pain. Multiple pleurodeses are often required, with installation into the pleural cavities of materials such as talc, and VATS pleurodesis is the most effective at palliating pleural effusions. For operable patients, some clinicians advocate a trimodality approach incorporating radical surgery with extrapleural pneumonectomy (en bloc removal of both the parietal and visceral pleura, involved lung, mediastinal lymph nodes, diaphragm and pericardium with mesh reconstruction), coupled with neoadjuvant systemic chemotherapy and adjuvant hemithorax intensity modulated radiotherapy (IMRT). Nevertheless, disease progression rates are high and in one series the rate was 77% at 1 year. There is no randomized data to support this aggressive approach and most of the few patients who have been treated in this way experience severe side effects. One potential approach is chemoprevention for people at risk of mesothelioma as a consequence of asbestos exposure. Currently there are no clinical studies of chemoprevention, although celecoxib, the COX2 selective non-steroidal anti-inflammatory drug (NSAID), has shown promise in laboratory models. Table 27.2 Types of asbestos and cancer risk Figure 27.1 This chest X-ray and CT scan of a retired boiler-maker show diffuse circumferential pleural thickening of the right hemithorax, extending to the mediastinal pleura. In addition, there is substantial volume loss of the right hemithorax. The appearances are due to mesothelioma. Unfortunately, the outlook for patients with mesothelioma is poor, with survival for patients with advanced disease ranging between 6 and 18 months. Three histological subtypes of mesothelioma exist: epithelial (55%), mixed (35%) and sarcomatoid (10%). The prognosis for these three subtypes is bad (epithelial), worse (mixed) and even worse (sarcomatoid). Case Study: The builder who could not climb his ladder.
Mesothelioma
Epidemiology
Pathogenesis
Presentation
Percentage of all cancer registration
Rank of registration
Lifetime risk of cancer
Change in ASR (2000–2010)
5–year overall survival
Female
Male
Female
Male
Female
Male
Female
Male
Female
Male
Mesothelioma
<1
1
>20th
17th
1 in 773
1 in 150
+24%
+4%
<10%
<10%
Investigations
Treatment
Type
Colour
Morphology
Usage
Cancer risk
Location of mining
Crocidolite
Blue
Amphibole needles
10%
+++
South Africa, Australia
Amosite
Brown
Amphibole needles
5%
++
South Africa
Chrysotile
White
Serpentine corkscrew
85%
+
Canada
Prognosis
 ONLINE RESOURCE
ONLINE RESOURCE
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


