and Karl Reinhard Aigner3
(1)
Department of Surgery, The University of Sydney, Mosman, NSW, Australia
(2)
The Royal Prince Alfred and Sydney Hospitals, Mosman, NSW, Australia
(3)
Department of Surgical Oncology, Medias Clinic Surgical Oncology, Burghausen, Germany
In this chapter you will learn about:
Osteosarcoma
Osteoclastoma (central giant cell tumour of bone)
Ewing’s tumour
Chondrosarcoma
21.1 Osteosarcoma
Osteosarcoma in young people usually first develops as a painful lump near the end of a long bone.
A malignant tumour of bone-forming cells is called an osteosarcoma. This is a highly malignant cancer and tends to affect children and young adults, with the highest incidence between 10 and 25 years. The cause of osteosarcoma in young people is not known although it does occur most often in the growing parts of the bone near the bone ends while the patient is still growing and developing.
A rare and virtually incurable osteosarcoma sometimes develops in old people, but in these people, the sarcoma has almost always occurred in a bone with a long-standing bone disease called osteitis deformans or Paget’s disease of bone.
21.1.1 Presentation
Osteosarcoma in young people usually first develops as a painful lump near the end of a long bone. There may be an obvious swelling occasionally with overlying redness and sometimes a fever. The swelling may be tender and may at first look like an acute infection in the bone. This sarcoma tends to metastasise to lungs early in its course so that best results are achieved if it is diagnosed and treated very early.
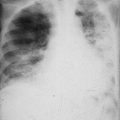
21.1.2 Investigations
Bone X-rays showing a diseased area with “sunray” appearance is typical of osteosarcoma. There is evidence of bone destruction and irregular new bone formation in the same area of the bone. More precise information can be learned from CT studies or MRI studies. PET scans if available may give even more information about the tumour. However, the ultimate deciding test is a biopsy in which a small piece of the tumour is taken for microscopic examination. Chest X-rays will also be taken to look for evidence of spread to the lungs although there is commonly micro-metastatic spread to the lungs before becoming visible in chest X-rays.
21.1.3 Treatment
The outlook has been greatly improved with modern chemotherapy given before and after surgery.
In the pre-chemotherapy days, osteosarcoma could rarely be cured. Treatment was by early amputation of an affected limb, sometimes in combination with radiotherapy, but death usually resulted due to development of lung metastases.
The outlook has been greatly improved with modern chemotherapy given before and after surgery (Sect. 8.3.4.8).
At first, amputation was commonly used to eradicate the primary sarcoma, and chemotherapy was used to eradicate any small microscopic metastases in the lungs before they could grow into larger incurable metastases. From almost no cures previously, the cure rate was improved to about 50 %, but in virtually all cured patients, a limb was amputated.
The use of chemotherapy has now been taken even further. Rather than amputation of the limb, induction chemotherapy is given first. Chemotherapy will affect the primary sarcoma in the bone, making it smaller and less aggressive. At the same time, the circulating chemotherapy helps eradicate any micro-metastatic deposits of sarcoma in lungs or elsewhere. In some specialised treatment centres, the primary cancer can be exposed to an even greater concentration of chemotherapy if given by intra-arterial infusion. Having passed through the limb, the chemotherapeutic agent then flows into the general circulation as systemic chemotherapy and affects micro-metastatic deposits in lung or elsewhere. Although attractive as a potentially more effective method of exposing the primary cancer to more concentrated chemotherapy, the technique requires close nursing attention and expert management, and as yet, studies have not been carried out to determine whether the advantage gained justifies the more complex and more expensive technique.
Reports of cures without amputation in 80 % of cases in which intra-arterial chemotherapy was given first as induction treatment have now been matched by reports of equally successful results with treatment by intense high–dose chemotherapy given systemically pre-operatively. In both cases, post-operative systemic “adjuvant” chemotherapy is given to deal with any residual cancer cells wherever they might be, most likely in the lungs.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


