Male Breast Lesions
NORMAL HISTOLOGY
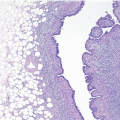
The adult male breast, like the female breast, is composed of glandular epithelial elements embedded in a stroma composed of varying amounts of fibrous tissue and adipose tissue. However, in contrast to the female breast, the epithelial components of the male breast consist primarily of branching ducts and terminal ductules with minimal, if any, acinar formation (Fig. 16.1, e-Fig. 16.1). Lobular development has been reported in males with Klinefelter syndrome and in other conditions associated with high serum estrogen.
GYNECOMASTIA
Gynecomastia is the most common lesion of the male breast. Although this is sometimes seen in association with known endocrine abnormalities and the use of certain drugs (including digitalis, spironolactone, tricyclic antidepressants, and marijuana) or topical agents (such as lavender and possibly tea tree oils), in most cases the etiology is unknown. Gynecomastia occurs most often around the age of puberty or in old age. The process may be either localized or generalized and can be unilateral or bilateral. Gynecomastia is also very common in male newborns as a result of in utero exposure to maternal estrogens.
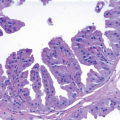
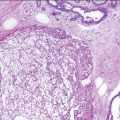
The histologic appearance varies with the duration of the condition. In all stages, the number of ducts is increased, and there may be duct dilatation. Early in the disease, the periductal stroma is loose, vascular, and cellular and contains varying numbers of lymphocytes and plasma cells. The duct epithelium may show hyperplasia with a characteristic pattern of tapering tufts protruding into the lumen, a pattern similar to that sometimes seen in benign epithelial hyperplasia in women and in the epithelial component of many juvenile fibroadenomas (Fig. 16.2, e-Fig. 16.2). In the later stage, there is progressive periductal fibrosis and stromal hyalinization (Fig. 16.3), and the epithelium undergoes atrophy (Table 16.1).1 Apocrine metaplasia may be seen in either early or later stages. Squamous metaplasia is most common in the early phase. Pseudoangiomatous stromal hyperplasia may be seen in any phase and may be prominent (Fig. 16.4).2 Lobule formation may be seen, and the lobules may even show lactational-like changes (Fig. 16.5).
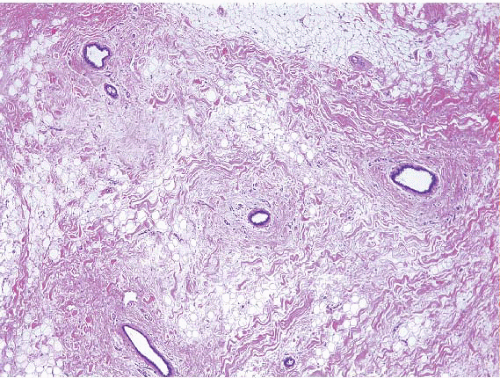 FIGURE 16.1 Normal male breast. There are scattered ducts in a fibroadipose stroma. Note the absence of lobules. |
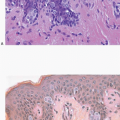
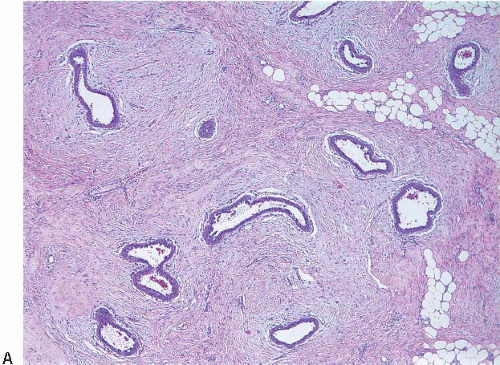 FIGURE 16.2 A: Gynecomastia, early stage, characterized by an increased number of ducts surrounded by a loose periductal stroma. B: A few tapering tufts of epithelium protrude into a duct lumen. |
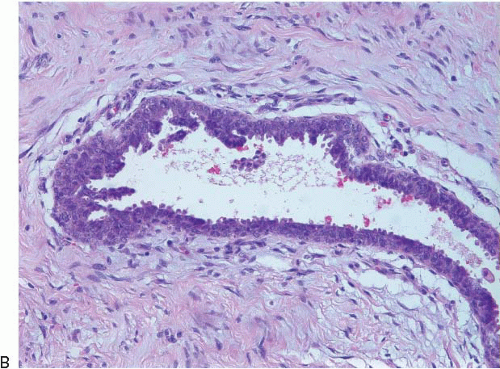 FIGURE 16.2 (Continued) |
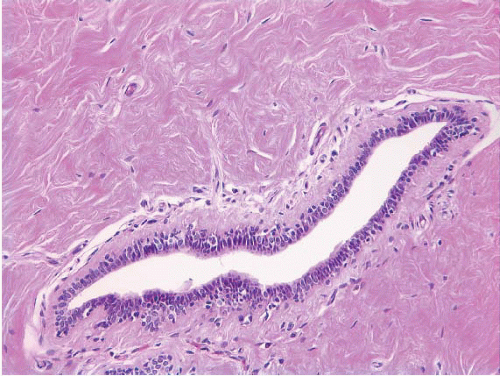 FIGURE 16.3 Gynecomastia, fibrous stage, with periductal fibrosis. |
TABLE 16.1 Key Features of Gynecomastia | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The epithelial hyperplasia seen in the early stages of gynecomastia can be quite florid and may on occasion produce a worrisome appearance with solid, cribriform, or papillary growth patterns. In some cases, the combined architectural and cytologic features may be sufficient to warrant a diagnosis of atypical ductal hyperplasia (Fig. 16.6, e-Fig. 16.3) or to raise the possibility of ductal carcinoma in situ (DCIS). However, the subsequent breast cancer risk associated with such atypical intraductal proliferations in the setting of gynecomastia (and in the male breast in general) is unknown. Therefore, in our view, the threshold for rendering a diagnosis of DCIS in this setting should be high.
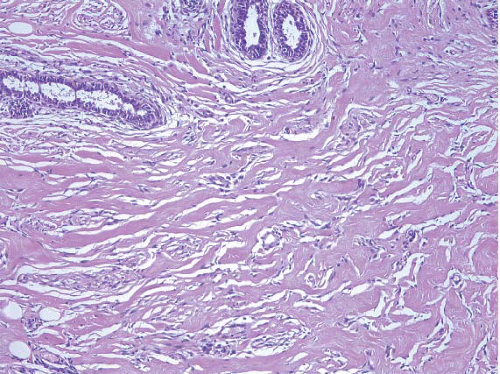 FIGURE 16.4 Pseudoangiomatous stromal hyperplasia in gynecomastia. |
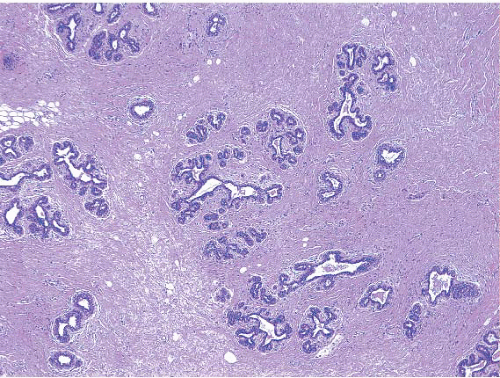 FIGURE 16.5 Abortive lobule formation in gynecomastia. |
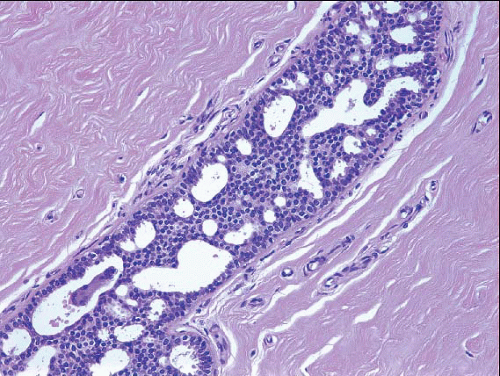 FIGURE 16.6 Atypical ductal hyperplasia in gynecomastia. |
OTHER BENIGN LESIONS
Other benign lesions that have been reported to occur in the male breast include fibroadenoma, phyllodes tumor, intraductal papilloma, duct ectasia, myofibroblastoma, lymphocytic mastopathy/diabetic mastopathy, cavernous hemangioma, and pseudoangiomatous stromal hyperplasia. The histologic appearance of these lesions is similar to that seen in the female breast.
CARCINOMA OF THE MALE BREAST
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


