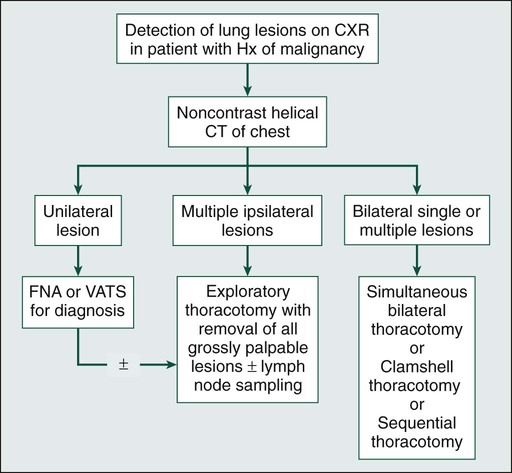
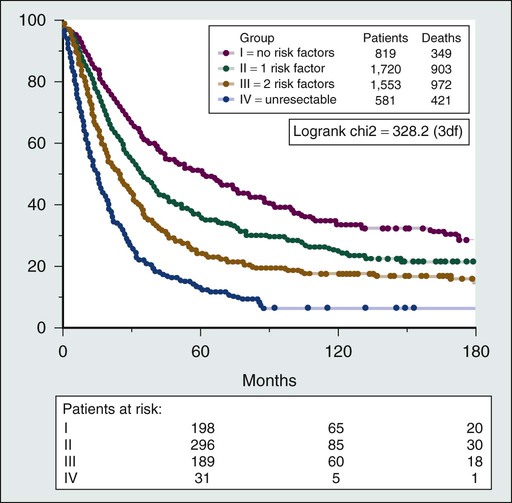
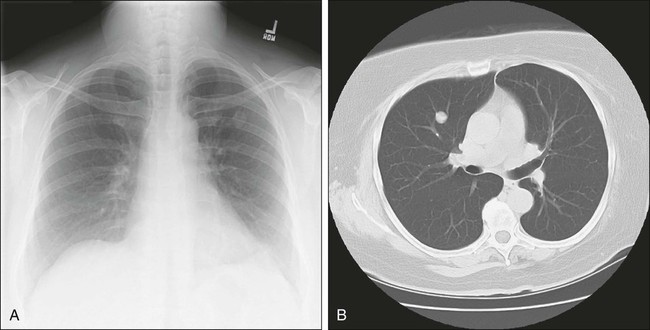
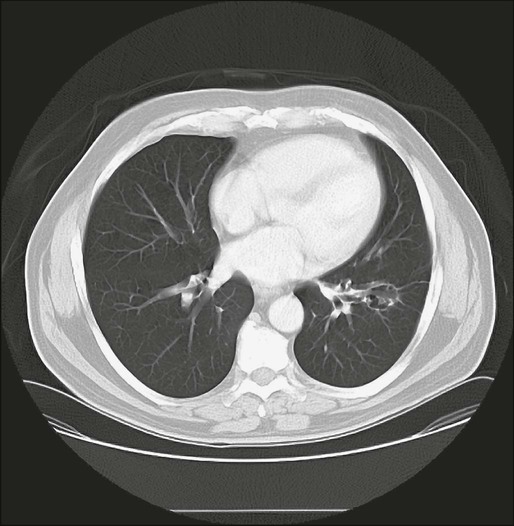
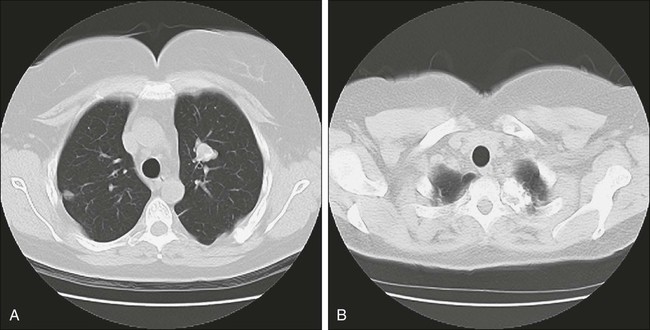
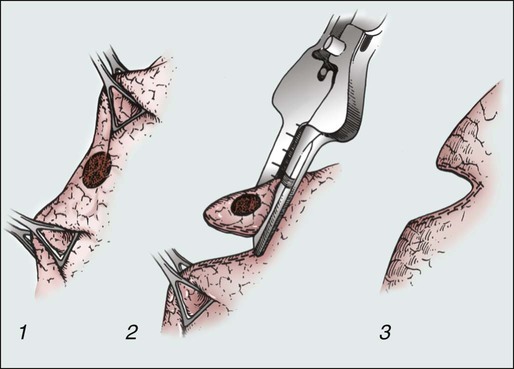
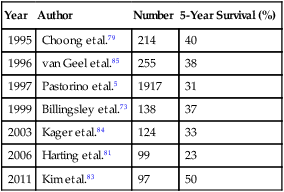
R. Taylor Ripley and Valerie W. Rusch • Lungs are the second most common site of metastases. • Lungs are the sole site of metastasis in 80% of patients with sarcoma and in 2% to 10% of patients with carcinoma. • Lung metastases occur via hematogenous spread. • Lymphangitic spread in carcinomas can occur early or late in the natural progression of all cancers. • It is not well understood why lung metastases take several years to develop. • Few lung metastases are symptomatic; only 15% to 20% of patients report having a cough or pain. All patients with isolated pulmonary metastasis from an extrathoracic malignancy should be evaluated for the possibility of resection. • Initial imaging studies should consist of a computed tomographic (CT) examination to predict resectability. Integrated fluorine-18 fluorodeoxyglucose positron emission tomography–CT may be substituted for CT alone. Magnetic resonance imaging has a limited role. • CT is unable to distinguish reliably between malignant and benign lesions. • CT differs from the final pathology report in 42% of cases. • CT underestimates the number of malignant lesions in 25% to 35% of cases. • The accuracy of radiologic imaging is only 37%, underestimating the number of lesions by 39% and overestimating them by 25%, for patients undergoing bilateral exploration. • Prognostic factors include number of metastases, disease-free interval, and histology/organ site of the primary tumor. Pulmonary Metastasis for Specific Tumor Types • From 10% to 25% of patients with primary colorectal tumors have detectable metastases at the time of primary tumor diagnosis. • Metastatic disease develops in 25% to 70% of patients with localized bone and soft tissue sarcoma; 10% will present with metastasis at the time of primary tumor diagnosis. • Patients with metastatic melanoma have an especially poor prognosis, with isolated lung metastasis occurring in 2% to 11% of patients. • In 50% of patients who have a radical nephroureterectomy, pulmonary metastases later develop; however, only 16% have metastatic disease confined to the lung. • Head and neck tumors, especially squamous cell cancers, tend to metastasize to the lung; however, 10% to 40% of lung nodules in these patients are actually second cancers manifesting as primary lung tumors. • Pulmonary metastasis upon presentation occurs in approximately 50% of patients with retroperitoneal germ cell tumors. • The first case of pulmonary metastasectomy was described by Weinlechner in 1882. • Alexander and Haight described the first series of patients; 12 patients remained disease free for 1 to 12 years. • The following general guidelines should be met before undertaking a resection: • The location of metastases determined the extent and type of resection: • All grossly palpable tumors must be resected with clear margins. • More radical resection (e.g., a lobectomy or pneumonectomy) does not increase survival rates. • Bilateral metastases and recurrence of pulmonary metastases are not contraindications to resection and should not deter resection in lesion(s) that can be removed completely. Two therapeutic options are emerging as potentially effective alternatives to resection: stereotactic body radiation therapy and radiofrequency ablation. The first described case of pulmonary metastasectomy was reported in 1882 by a German surgeon named Weinlechner, who removed two incidental pulmonary nodules during a chest wall resection for sarcoma.1 In 1938 Barry and Churchill2 reported the first long-term survivor from pulmonary metastasectomy, a patient with metastatic renal cell cancer. Their patient survived 23 years after surgery. Subsequently, Alexander and Haight described the first series of patients undergoing pulmonary metastasectomy and its correlation to survival.3 Twelve patients in their study remained free of disease for 1 to 12 years. Most important, from this early study came the first generally accepted criteria for pulmonary metastasectomy: 1. The primary tumor should be completely removed. 2. There should be no evidence of extrapulmonary disease. 3. The patient should be able to tolerate the planned operation from the standpoint of his or her overall medical condition. Subsequently these criteria were modified by other authors to reflect our improved understanding of the management of pulmonary metastases. Current additional criteria include:4 1. Control of the primary tumor, or ability to resect the primary tumor completely simultaneous with resection of metastasis 2. Ability to resect metastatic disease completely 3. Ability of the patient to tolerate the extent of pulmonary resection required to remove all gross tumor 4. Absence of extrathoracic metastasis Several prognostic factors that are not universal across all tumor histologies have been reported to affect outcome after pulmonary metastasectomy (Box 52-1). The largest series of pulmonary metastasectomy reported to date is from the International Registry of Lung Metastasis, which analyzed 5206 cases.5 The overall 5-year survival after pulmonary metastasectomy without stratifying for tumor type was 36%. Factors associated with better prognosis included a long disease-free interval (DFI), complete resection, and a small number of lung nodules. A staging system based on these prognostic factors was proposed (Fig. 52-1). The role of surgery in the treatment of pulmonary metastases will continue to evolve as better systemic therapies become available. Currently, only a minority of patients with metastatic disease from any source are candidates for pulmonary metastasectomy; however, improved imaging studies and the widespread use of computed tomography (CT) might detect more patients who have small-volume pulmonary metastases and are therefore candidates for metastasectomy. Recently, the European Society of Thoracic Surgeons formed the Lung Metastasectomy Working Group to review the evidence and produce guidelines.6 They concluded that the level of evidence is relatively low and randomized controlled trials are absent in this field. Despite these limitations, long-term survival does exist for patients with multiple histologies who rarely have long-term survival with systemic therapy alone. A current perspective of the evaluation and treatment of patients with isolated lung metastases is presented in this chapter. Few patients with pulmonary metastasis are symptomatic. It is estimated that only 15% to 20% of patients present with a cough or nonspecific chest pain and even fewer still with hemoptysis. Traditionally, a chest radiograph has been the most commonly used and cost-effective modality for screening patients for metastasis from extrathoracic malignancy, but CT scans have rapidly replaced the chest radiograph as the most useful tool. The most frequent radiographic appearance of a pulmonary metastasis is a peripherally located, well-circumscribed nodule (Fig. 52-2).7,8 Several less common radiographic characteristics have also been described. Cavitating lesions are associated with a differential diagnosis that includes benign, infectious, and malignant causes (Fig. 52-3). When cavitary lesions are malignant, they are usually squamous cell carcinomas. The frequency of cavitation in metastatic nodules is approximately 4%; however, squamous cell malignancy is responsible for 69% of these lesions. Spontaneous pneumothorax also can occur with metastatic lung lesions and is thought to be caused by cavitation and erosion into a bronchiole wall. Spontaneous pneumothorax is most frequently seen in patients with sarcoma. It is said that a spontaneous pneumothorax in a patient with a history of sarcoma should prompt an evaluation for possible occult metastatic lung lesions. Calcification of pulmonary nodules is usually related to a benign process such as a hamartoma; however, metastatic lesions of many types (especially osteogenic sarcoma) are known to produce calcification (Fig. 52-4).7,8 Calcification in metastatic lesions is thought to be produced by several processes in different tumor types, including bone formation in osteogenic sarcoma, mucinous calcification of adenocarcinomas, or dystrophic calcification of lesions such as synovial sarcoma or giant cell tumors of the bone.7 Hemorrhage around lung nodules is also seen more frequently in benign lung lesions (e.g., fungal or mycobacterial infections) and is visualized as a halo around the lung nodule. This appearance can also be seen in metastatic lesions and should raise the suspicion for metastasis in patients with a prior history of malignancy. The use of CT has supplanted chest radiography as the primary mode of imaging pulmonary metastases. CT is able to visualize more lesions than chest radiographs as noted in several reports.5,9–18 Chang and colleagues12 reported that when compared with conventional radiography, CT was able to visualize nearly twice as many nodules.19 This change has been facilitated by the development of high-speed, multislice scanners. These scanners are available up to 256 slices, but no data exist to indicate that these extremely high-resolution scanners detect more lesions than 5-mm thin-slice scanners.20 CT is not able to distinguish reliably between malignant and benign lesions, however. McCormack and coworkers9 retrospectively studied 144 patients who had both a chest radiograph and a CT scan to identify metastatic lesions. The CT results differed from the final pathology reports in 42% of cases, with CT scans underestimating the number of malignant nodules in 25% of patients. Pastorino and associates5 reported results of imaging on 2988 patients undergoing pulmonary metastasectomy. The overall accuracy of radiologic assessment of the number of metastatic nodules was 61%, underestimating metastasis in 25% of patients. Interestingly, in the patients (1134) who had bilateral exploration, the accuracy of imaging was only 37%, underestimating the number of lesions in 39% and overestimating the number in 25%. Cerfolio and associates21 prospectively assessed the incidence of nonimaged malignant nodules at thoracotomy among patients who had a 64-slice helical CT scan with 5-mm slices.21 Fifty-one patients of 152 (34%) had 57 pulmonary nodules that were not detected preoperatively. Thirty-two of the 57 nodules (56%) were malignant. Ellis and associates22 reported a similar conclusion. Significantly more nodules were palpated at thoracotomy than were detected preoperatively despite using a multidetector helical CT scanner with 5-mm slices (mean 3.24 vs. 2.12). In 19 of 54 thoracotomies for osteosarcoma (35%), Kayton and associates23 reported additional metastatic lesions not imaged by 5-mm CT scanners. The accuracy and sensitivity of CT also depend on the size of the lesions (Table 52-1): the larger the lesion, the greater the sensitivity and accuracy. Munden and colleagues,15 who reported on the clinical significance of pulmonary lesions less than 1 cm in diameter, found malignant pulmonary lesions in 81% of patients with a history of prior malignancy. Multiple authors have described the ability of CT to detect a greater number of pulmonary nodules, while acknowledging a decreasing specificity of identifying malignant nodules with this diagnostic tool.12,16 Therefore not all small pulmonary nodules in patients with a history of cancer can be assumed to represent metastatic disease. Currently no established guidelines exist for routine screening for pulmonary metastases, but CT scanning has become the sole screening tool for identifying pulmonary metastases in recent reports.12,16 Table 52-1 Detection of Pulmonary Metastasis by Computed Tomography Magnetic resonance imaging (MRI) provides the benefits of reduced radiation exposure (of particular interest for cases involving younger patients) and the ability to detect lesions at lung-mediastinal interfaces. MRI has not gained wide acceptance as a screening tool, however, mainly because of its increased time constraints and cost. Further unfavorable technical considerations include motion-related artifacts and an inability to detect calcified lesions. Kersjes and coworkers24 performed a study comparing MRI and helical CT in the detection of pulmonary metastasis and showed that MRI has an overall accuracy of 84%. For lesions smaller than 5 mm, however, the sensitivity of MRI was only 36%. The routine use of MRI is currently not advocated as a screening tool for patients with pulmonary metastasis. Imaging with fluorine-18 fluorodeoxyglucose positron emission tomography (FDG-PET) is being used frequently to assist in the staging of primary tumors. This modality is used most often at the time of diagnosis to rule out distant metastasis, but occasionally it is used to assess response to therapy. Currently FDG-PET is not the standard for identifying pulmonary metastasis, but it is increasingly used in this role.25,26 Pastorino and associates27 report that 19 of 86 patients (21%) were excluded from pulmonary metastasectomy because of multiple histologies on the basis of the results of FDG-PET. Dalrymple-Hay and associates25 reported that 9% of patients who were evaluated for pulmonary metastasectomy for metastatic melanoma were excluded because of FDG-PET results. Unfortunately, the number of patients screened was unclear in this study. Other authors suggest that FDG-PET is not superior to CT in the identification of pulmonary metastasis. Lucas and colleagues28 studied 62 patients with soft tissue sarcoma who had FDG-PET during initial evaluation. The sensitivity of FDG-PET in detecting lung metastasis was 86.7% compared with 100% for CT. FDG-PET may not be superior to conventional imaging techniques in identifying pulmonary metastasis from bone and soft tissue sarcomas.28,29 The value of FDG-PET alone may be an obsolete argument with the increased use of integrated PET-CT. The data regarding this modality are limited, but integrated scanners may optimize the advantages of both studies. In the previously mentioned prospective study by Cerfolio and associates,21 preoperative identification of pulmonary metastasis was performed by helical CT scans, but 132 of 152 patients (87%) had integrated PET-CT. Despite use of this technology, 34% of patients had lesions identified at thoracotomy that were not detected preoperatively. In addition, FDG-PET, whether integrated or not, does not reliably detect subcentimeter lesions. Reinhardt and associates30 report that the false-negative rate for detecting 6 to 10 mm lesions is 41%, and for lesions less than 5 mm, it is 100%. Integrated PET-CT may have a role in detection of unsuspected extrathoracic disease prior to pulmonary metastasectomy, but strong recommendations for this modality cannot be made at this time. The goal of pulmonary metastasectomy is to achieve complete resection of all visible and palpable tumor in the lung. The surgical approach is dictated by the extent and location of disease and by the patient’s performance status. Several approaches are available depending on the size, number, and location of the lesions. The advantages and disadvantages of these approaches are outlined in Table 52-2. Table 52-2 Surgical Approaches to Resection of Pulmonary Metastases Video-assisted thoracoscopy (VATS) for pulmonary metastasectomy has been fairly extensively described during the past 15 years. This approach remains controversial, however.31–35 McCormack and coworkers32 performed a prospective study evaluating the role of VATS to treat pulmonary metastasis. Eighteen patients had preoperative CT followed by VATS resection of all visible and CT-detected lesions. All patients then immediately underwent thoracotomy with resection of any additional lung nodules. Additional malignant lesions were found in 56% of patients after attempted VATS resection. VATS is dependent on preoperative imaging to detect metastatic lesions. Since this study by McCormack and colleagues was reported in 1996, improvements in helical scanning and the expanded role of integrated PET-CT have occurred, as noted in the previous section. Despite these improvements, several authors report similar results of missed lesions based on preoperative imaging.21,22 As mentioned previously, Cerfolio and associates,21 Ellis and colleagues,22 and Kayton and associates23 reported missed lesions by preoperative imaging among patients who underwent modern helical CT scanning with 5-mm slices. Despite these advances in technology, a significant number of metastases are detected by palpation at open thoracotomy that would be missed by VATS resection. Some authors have advocated the use of VATS for patients with a solitary pulmonary metastasis. Mutsaerts and associates31,35 described their experience with 20 patients undergoing either VATS or thoracotomy for resection of a single pulmonary metastasis. The 5-year survival and recurrence rates appeared to be similar to the rates seen with thoracotomy.35 Gossot and colleagues36 reviewed the resection of one or two metastases from sarcoma by comparing 31 patients treated by VATS with 29 patients who underwent thoracotomy but were deemed appropriate for VATS. These investigators concluded that VATS yielded similar survival rates for patients with one or two nodules from sarcoma. Other authors have described localization methods using radiotracer injection to help identify small or deeply located lesions during VATS resections.33,37 Despite clear evidence that additional lesions are discovered at thoracotomy compared with preoperative evaluation, a survival advantage has not been shown. Nakas and associates38 report no difference in actuarial survival among 27 patients undergoing VATS resection compared with open resection of colorectal cancer with a median follow-up of 22 months. Of note, 32% of patients in the VATS group and 37% in the open group had hepatic metastases, and therefore extrathoracic disease may be as responsible for mortality as pulmonary disease. Carballo and associates report a retrospective review of 186 patients, of whom 135 were treated by thoracotomy and 36 by VATS for multiple histologies.194 With a median follow-up of 26 months, they report an insignificant difference in both 5-year actuarial and median survivals. Nakajima and associates37 reported significantly more recurrent nodules after open thoracotomy (27/43, 62.8%) versus VATS (27/79, 34.2%) at 2 years after the operations. In addition, they reported a significantly lower recurrence-free survival after open thoracotomy. The approach to bilateral disease is more variable, but the principles remain the same. A median sternotomy, “clamshell” thoracotomy (i.e., a bilateral anterior thoracotomy with a transverse sternotomy), sequential bilateral thoracotomies, and simultaneous bilateral posterolateral thoracotomies are used as standard surgical approaches to the resection of bilateral metastases.41–41 In general, resection of bilateral metastases is preferably done as a single operation. Sequential thoracotomies are performed only when the anatomic location of a lesion requires a complex or extensive operation or when the patient’s comorbidities dictate a more conservative approach to management. Members of the European Society of Thoracic Surgeons were surveyed by Internullo and associates42 to determine the current clinical practices for pulmonary metastasectomy. Sixty-five percent considered palpation of the lung necessary for adequate metastasectomy. Of those who performed open thoracotomy for bilateral disease, two out of three perform bilateral staged thoracotomies. Median and clamshell sternotomies were performed less frequently. Regardless of the favored approach, the majority of surgeons altered their approaches based on tumor location, lung function, the number of metastases, and the performance status of the patient. In contrast to primary lung cancers, pulmonary metastases require only a local excision with a surrounding rim (1 to 2 cm) of benign lung tissue. The European Society of Thoracic Surgeons Practice Pattern Survey revealed that local excision is performed in 92% of cases.42 This technique is accomplished most frequently by wedge resection performed by precision electrocautery or with a stapling instrument (Fig. 52-5). Segmentectomy, lobectomy, or pneumonectomy are used less commonly. It is important to note that survival after metastasectomy is not increased by a more radical resection such as lobectomy or pneumonectomy. These procedures might be required technically to remove the lesion, however, and should be applied to do so if needed. The most important principle of these techniques is a clear margin of resection. The preoperative evaluation for these patients is similar to that for patients undergoing lung resection for any other cause (Fig. 52-6). Pulmonary function testing should be obtained for all patients to ensure that the volume of lung resection will not compromise overall respiratory function. Thorough evaluation of underlying cardiovascular disease should also be undertaken, with preoperative stress testing as clinically indicated. It is estimated that 10% to 25% of patients with primary colorectal tumors will have detectable metastases at the time of diagnosis.43 Despite advances in adjuvant therapy and surgery, 50% of all patients with colorectal cancer will develop some form of metastasis during their lifetimes.44 In approximately 15% of patients having curative resection of their primary colorectal tumor, distant metastasis will develop, including metastasis to the lung.45 Isolated pulmonary metastases occur in about 2% to 7% of patients with colon cancer and about double that number for patients with rectal cancer.46 Pulmonary metastasis can occur even with favorable primary tumor characteristics. Okumura and associates47 reported that 26% of pulmonary metastectomies were performed in patients with Duke A or B primary colorectal cancer. Since Blalock48 reported the first pulmonary metastasectomy for colorectal cancer in 1944, several authors have reported their experience regarding overall survival and prognostic factors. The 5- and 10-year survival rates range from 30% to 68% and 20% to 37%, respectively (Table 52-3).49–55 It is clear from the literature that pulmonary metastasectomy for colorectal cancer is associated with long-term survival, especially when a complete resection is performed. McCormack and colleagues56 reviewed 144 patients who underwent pulmonary metastasectomy for colorectal cancer and showed that survival for patients who underwent complete resection was approximately 40% at 5 years, whereas incomplete resection was associated with a poor prognosis. More recently, Melloni and associates57 reported the same conclusion with a 5-year survival rate of 44% for complete resection versus 0% for incomplete resection. Table 52-3 Survival of Patients Undergoing Pulmonary Metastasectomy for Colorectal Cancer* As for other primary tumors, studies evaluating the DFI, the number of lesions, and the presence of lymph node involvement have shown that these prognostic factors are significant after pulmonary metastasectomy for colorectal cancer.47,49–52,56,58–63 Recently Oniatis and associates54 reported that more than three metastases, DFI less than 1 year, age older than 65 years, and male sex were adverse prognostic factors on multivariate analysis. Colorectal cancer is also unique in that the serum tumor marker carcinoembryonic antigen (CEA), which is used as a marker for follow-up, has been shown to be a prognostic indicator for patients with pulmonary metastases.49–52,55,56,58–62,64,65 Also relatively unique to colorectal cancer is that pulmonary metastasectomy with either synchronous or metachronous resected hepatic metastasis is another reported adverse prognostic factor.66 The presence of bilateral metastases was previously thought to be a contraindication to metastasectomy, but the significant prognostic factor is probably the number of metastases, not the laterality. Several authors have reported that the survival for patients with bilateral lesions is not significantly reduced compared with patients who have multiple ipsilateral lesions.50,59 Although a solitary metastasis might be associated with a better prognosis than multiple metastases (either unilateral or bilateral), the main criteria used to select patients with multiple lesions is whether removal of these lesions is technically feasible and whether removal of the volume of lung parenchyma does not appear to compromise the patient’s lung function to a significant extent. CEA levels are elevated in 40% to 70% of patients prior to pulmonary metastasectomy. Most authors report that elevated CEA levels are an adverse prognostic factor.51,52,60,61,67 The reason for this observation is unclear, although it has been postulated that the presence of CEA may promote adhesion or attachment of tumors cells or could be due to undetected extrathoracic metastasis.68 Although an elevated CEA level is not used currently to exclude patients from resection, it could be useful to consider this value in the context of other known prognostic factors. Multiple studies have reported cutoff values for CEA levels that predict a poor prognosis.55,64,65 Lee and associates64 report 5-year survival rates of 86.9% for patients with normal CEA levels versus 23.4% for patients with CEA levels greater than 5 ng/mL. Saito and associates52 report similar results with a 4-year survival of 42.7% versus 15.1% for patients with less than or greater than 10 ng/mL of CEA, respectively. Kanemitsu and associates65 reported that prethoracotomy CEA levels were one of the strongest prognostic factors for adverse outcomes. CEA displayed the strongest relationship with death at 3 years on multivariate analysis. This relationship is strong enough that increasing CEA was associated with decreased survival in a preoperative nomogram. These data reveal that CEA is an important prognostic factor, but it doesn’t necessarily exclude patients from resection. A useful approach may be to recommend that a patient with a persistently or rapidly increasing CEA after primary resection be treated initially with chemotherapy rather than directly undergoing pulmonary metastasectomy. Hilar or mediastinal lymph node metastases occur in 1% to 49% of patients with colorectal pulmonary metastasis.47,52,54,56,58,59,61 Oniatis and colleagues54 reported that of 378 patients, 175 (46%) had N0 disease, 131 (35%) had N1 disease, and 54 (14%) had N2 disease, with only 5% unknown. Saito and associates52 reported that the 5-year survival was 48.5% for the patients without hilar or mediastinal lymph node metastasis versus 6.2% at 4 years for the patients with lymph node metastasis. Welter and colleagues53 reported that 28 of 169 patients undergoing resection of colorectal pulmonary metastases had intrapulmonary, hilar, or mediastinal nodal metastases, with 5-year actuarial survivals at 78, 0, and 0%, respectively. The 5-year survival rates were 42% versus 19% without or with any lymph node involvement, respectively. This study reveals that any lymph node involvement and increasing station of involvement adversely affect overall survival. Okumura and colleagues47 performed systematic lymph node dissection for 100 patients with colorectal pulmonary metastasis. Fifteen of these patients had positive lymph nodes with a 5-year survival of 6.7% compared with a 50% survival rate for patients with negative lymph nodes, indicating that complete lymph node dissection does not increase survival. The routine use of mediastinal lymph node dissection in patients with pulmonary metastases appears to be the exception rather than the norm. The presence of malignant lymph nodes could indicate a group of patients otherwise thought to be disease-free who might benefit from additional adjuvant therapy. We favor mediastinal lymph node sampling or dissection in these patients. Although these procedures might not have a therapeutic effect, they certainly provide important prognostic information. Previously, the presence of both liver and lung metastases from colorectal cancer was thought to be a contraindication to metastasectomy, but during the past decade, authors of several studies have reported long-term survival with combined pulmonary and hepatic metastatsectomy.66,69–71 Synchronous or metachronous lung and liver metastasis occurs in approximately 5% of patients with colorectal cancer. Headrick and coworkers72 reported 5- and 10-year survivals of 30% and 16%, respectively, for 58 patients who underwent resection of both liver and lung metastases from colorectal cancer. Zabaleta and associates66 reported 3- and 5-year survival rates of 50% and 39% after pulmonary metastasectomy among 17 patients who had previously undergone hepatic metastasectomy for colorectal carcinoma. Decreasing morbidity and mortality rates for liver resection now make resection of both lung and liver metastases a viable option in carefully selected patients. Bone and soft tissue sarcomas constitute a histologically diverse group of tumors accounting for 1% of all adult malignancies, with approximately 6600 cases occurring in the United States annually.73,74 Metastasis will occur in 25% to 70% of patients with localized disease, and 10% will present with metastasis upon diagnosis.74 Isolated pulmonary metastases occur in up to 20% of patients with sarcoma during the course of their disease, with the lung being the site of failure after treatment in up to 90% of cases.75,76 Inability to control thoracic disease is the most common cause of death.77 Factors associated with an increased risk of pulmonary metastasis include high tumor grade, primary tumor size greater than 5 cm, lower extremity site, and histologic subtype.75,78 The lack of effective systemic therapy for most soft tissue sarcomas makes surgical resection the best treatment for pulmonary metastases. Several studies have shown that the complete resection of pulmonary metastases is associated with long-term survival.5,73,75,78–83 Billingsley and associates73 reported that the 3-year actuarial survival was 46% in patients who had complete resection compared with 17% (P < .001) for patients with incomplete resection of pulmonary metastasis. Kager and colleagues84 reported similar findings with 5-year actuarial survival of 44% in patients with complete resection versus 0% with incomplete resection. The completeness of surgical resection was one of only two prognostic factors that was significant on multivariate analysis. The cumulative 5-year survival for patients with bone and soft tissue sarcomas after pulmonary metastasectomy ranges from 23% to 50% (Table 52-4).5,73,79,83–87 Table 52-4 Survival of Patients Undergoing Pulmonary Metastasectomy for Bone and Soft Tissue Sarcomas
Lung Metastases
 Some form of metastasis develops in 50% of all patients with colorectal cancer.
Some form of metastasis develops in 50% of all patients with colorectal cancer.
 Isolated lung metastases occur in up to 20% of patients with sarcoma during the course of their disease, with the lung being the sole site of failure after treatment in up to 90% of cases.
Isolated lung metastases occur in up to 20% of patients with sarcoma during the course of their disease, with the lung being the sole site of failure after treatment in up to 90% of cases.
 Control of the primary tumor or ability to resect the primary tumor
Control of the primary tumor or ability to resect the primary tumor
 Ability to resect metastatic disease completely
Ability to resect metastatic disease completely
 Absence of extrathoracic metastasis
Absence of extrathoracic metastasis
 Absence of better alternative treatment
Absence of better alternative treatment
 Peripheral metastases: parenchymal sparing
Peripheral metastases: parenchymal sparing
 Central metastasis: lobectomy or pneumonectomy
Central metastasis: lobectomy or pneumonectomy
 Solitary endobronchial metastasis: lobectomy, sleeve lobectomy, or pneumonectomy
Solitary endobronchial metastasis: lobectomy, sleeve lobectomy, or pneumonectomy
Introduction
Diagnosis
Computed Tomography
Year
Author
No. Nodules
Sensitivity for Small Lesions (%)
Sensitivity for Larger Lesions (%)
1998
Waters et al.*19
144
44 (≤5 mm)
91 (>5 mm)
1999
Diederich et al.10
90
69 (≤6 mm)
95 (>6 mm)
2002
Margaritora et al.†11
188
48 (≤6 mm)
87 (>6 mm)

Magnetic Resonance Imaging
Nuclear Imaging
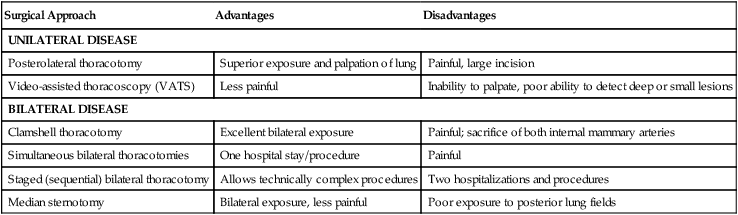
Surgical Approaches to Lung Metastasis
Surgical Approach
Advantages
Disadvantages
UNILATERAL DISEASE
Posterolateral thoracotomy
Superior exposure and palpation of lung
Painful, large incision
Video-assisted thoracoscopy (VATS)
Less painful
Inability to palpate, poor ability to detect deep or small lesions
BILATERAL DISEASE
Clamshell thoracotomy
Excellent bilateral exposure
Painful; sacrifice of both internal mammary arteries
Simultaneous bilateral thoracotomies
One hospital stay/procedure
Painful
Staged (sequential) bilateral thoracotomy
Allows technically complex procedures
Two hospitalizations and procedures
Median sternotomy
Bilateral exposure, less painful
Poor exposure to posterior lung fields
Pulmonary Metastasectomy for Specific Tumor Types
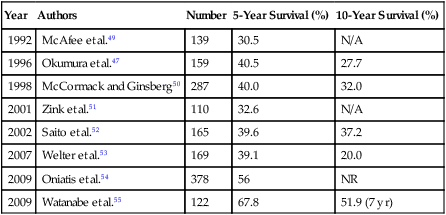
Colorectal Cancer
Year
Authors
Number
5-Year Survival (%)
10-Year Survival (%)
1992
McAfee et al.49
139
30.5
N/A
1996
Okumura et al.47
159
40.5
27.7
1998
McCormack and Ginsberg50
287
40.0
32.0
2001
Zink et al.51
110
32.6
N/A
2002
Saito et al.52
165
39.6
37.2
2007
Welter et al.53
169
39.1
20.0
2009
Oniatis et al.54
378
56
NR
2009
Watanabe et al.55
122
67.8
51.9 (7 yr)
Bone and Soft Tissue Sarcoma
Year
Author
Number
5-Year Survival (%)
1995
Choong et al.79
214
40
1996
van Geel et al.85
255
38
1997
Pastorino et al.5
1917
31
1999
Billingsley et al.73
138
37
2003
Kager et al.84
124
33
2006
Harting et al.81
99
23
2011
Kim et al.83
97
50
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Lung Metastases