Local Treatment of Early Breast Cancer
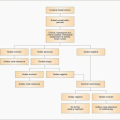
Treatment components (Figures 9.1, 9.2)
|

There are three components of the treatment of breast cancer: (1) local treatment of the cancer in the breast, (2) treatment of the loco-regional draining nodes, principally in the axilla, and (3) systemic treatments to eradicate any disease which may be present outwith the breast and loco-regional nodal basins. Breast cancer is uncommon in men and may present at a more advanced stage because of a smaller volume of breast tissue; however, the principles of management are the same in women and men.
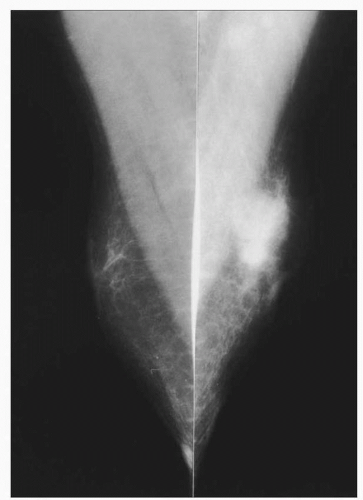 9.1 Mammograms of a male patient showing an irregular opacity on the left due to a breast cancer. |
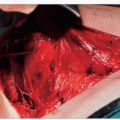
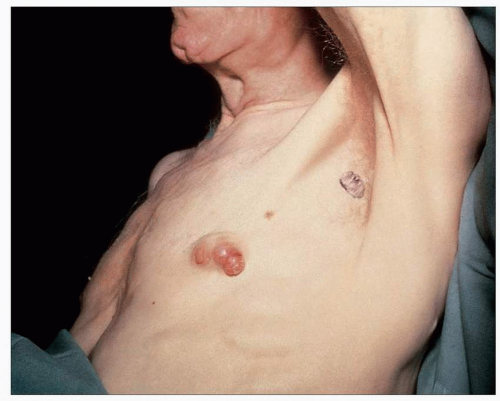 9.2 A locally advanced male breast cancer. |
Early (operable) disease
Initial treatment of the primary breast tumour in an individual with early or operable breast cancer is usually surgical. Some patients with locally advanced breast disease and most with cancers involving underlying muscle are suitable for a primary surgical approach, as long as other features such as inflammatory changes or distant metastatic disease are not present. The primary surgical options for management of the breast are mastectomy and breast conservation. Breast conservation therapy consists of excision of the tumour with a 1 cm macroscopic margin of normal tissue (wide local excision) plus breast radiotherapy. Controversy has surrounded how much extra tissue should be removed and what constitutes an involved or positive margin. Current evidence suggests that microscopic margins of 1 mm or more are adequate and that increasingly wide margins will not reduce local recurrence rates but will adversely affect cosmetic outcomes. Local recurrence rates should be less than 1% per annum following wide excision and radiotherapy.
There are lower levels of psychological morbidity with breast conservation than with mastectomy; it also results in comparatively better body image, freedom of dress, sexuality, and self-esteem. More extensive excisions of a whole quadrant of the breast (quadrantectomy) have worse cosmetic outcomes and do not have a significantly lower local recurrence rate than wide excisions. There is no size limit for breast conservation surgery, but adequate excision of lesions over 4 cm produces a poor cosmetic result in all but women with very large breasts, unless both breasts are reduced or the defect in the breast is filled by oncoplastic techniques. There is no age limit for breast conservation. The approach will depend on the size of the tumour in relation to the size of the breast, multifocality, and patient choice. Reasonable arm mobility is required to receive breast radiotherapy and if arm mobility is limited breast conservation may not be advisable.
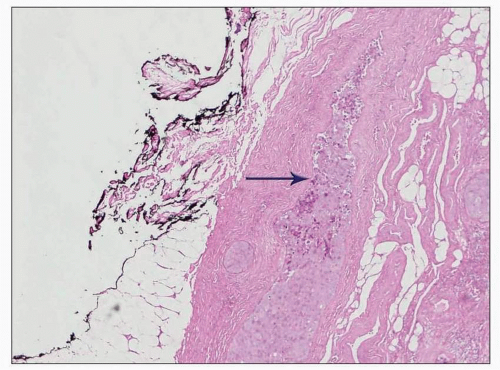
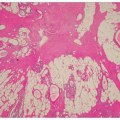
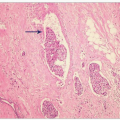
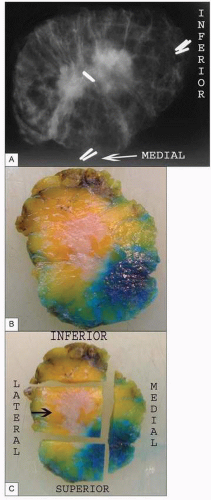 9.3 A: Specimen X-ray showing orientation clips and central tumour shadow; B: wide local excision specimen with corresponding central tumour; C: centre slice cut up showing block selection. Arrow points to tumour area. |
 9.4 Well healed scar following breast conservation therapy with wide excision of the breast cancer and radiotherapy. |
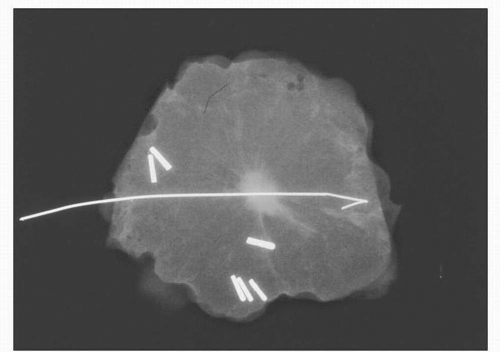 9.5 Specimen X-ray showing satisfactory margins following excision of a screen-detected, impalpable breast cancer. The lesion has been localized using a hooked wire and the specimen has been orientated using clips. |
 |
 9.7 Scar following mastectomy and radiotherapy to the chest wall. |
Mastectomy (Figure 9.7)
Mastectomy involves removal of as much of the breast tissue on the affected side as possible. It is usually performed if the extent of disease is large in relation to the size of the breast, where there is proven multicentric disease, or where a patient prefers mastectomy (Table 9.1). Patients sometimes choose mastectomy for disease suitable for breast conserving surgery because they think mastectomy has a better long-term survival. This is not true and once informed of this many are happy to choose breast conserving surgery.
Mastectomy is usually performed through a low
transverse scar to leave a flat wound with no excess skin to allow easy placement of an external prosthesis. The nipple is usually removed with an ellipse of skin usually incorporating the skin directly over the cancer. It is important to plan incisions to avoid unsightly ‘dog ears’ at the medial and lateral ends of mastectomy wounds. Other options to help avoid this include using a breast reduction-type skin incision (Wise pattern) or ‘fish tailing’ the ends of the wounds. Skin flaps are raised in the plane between the breast and subcutaneous fat down to the chest wall and the breast is then dissected off the chest wall posteriorly, leaving the fascia overlying the pectoral muscle (unless there is invasion of underlying muscle, when sufficient muscle should be excised to completely remove the cancer). Mastectomy flaps can be sutured to the chest wall by a quilting technique which appears to reduce the rate of subsequent seroma. The wound should be closed with an absorbable subcuticular stitch. If reconstruction is being undertaken, more skin (including the nipple in some circumstances) may be preserved (skin-sparing mastectomy). Drains are normally placed following surgery and these are usually left until drainage is less than 50 ml in 24 hours, or are removed routinely after 2-7 days depending on local protocol. Complications include bleeding, infection, and necrosis of the wound edge. Some degree of numbness of the skin flaps is expected and seroma formation is common.
transverse scar to leave a flat wound with no excess skin to allow easy placement of an external prosthesis. The nipple is usually removed with an ellipse of skin usually incorporating the skin directly over the cancer. It is important to plan incisions to avoid unsightly ‘dog ears’ at the medial and lateral ends of mastectomy wounds. Other options to help avoid this include using a breast reduction-type skin incision (Wise pattern) or ‘fish tailing’ the ends of the wounds. Skin flaps are raised in the plane between the breast and subcutaneous fat down to the chest wall and the breast is then dissected off the chest wall posteriorly, leaving the fascia overlying the pectoral muscle (unless there is invasion of underlying muscle, when sufficient muscle should be excised to completely remove the cancer). Mastectomy flaps can be sutured to the chest wall by a quilting technique which appears to reduce the rate of subsequent seroma. The wound should be closed with an absorbable subcuticular stitch. If reconstruction is being undertaken, more skin (including the nipple in some circumstances) may be preserved (skin-sparing mastectomy). Drains are normally placed following surgery and these are usually left until drainage is less than 50 ml in 24 hours, or are removed routinely after 2-7 days depending on local protocol. Complications include bleeding, infection, and necrosis of the wound edge. Some degree of numbness of the skin flaps is expected and seroma formation is common.
Table 9.1 Patients who are best treated by mastectomy | |
|---|---|
|
Breast conservation
If a unifocal breast cancer can be completely excised with a satisfactory margin without significantly deforming the breast, wide excision of the cancer should be considered. In general, around 10% of the breast volume can be excised without deformity although this proportion may be less for tumours in the medial part of the breast. It is not necessary to remove skin over the cancer. The nipple may be excised with the cancer if it lies in close relation or if malignant nipple discharge is present. The skin envelope and tissue within the breast can be mobilized to minimize any defect produced by wide excision.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


