Fig. 6.1
Trocar locations for laparoscopic gastrectomy
- (b)
A monitor is located over the patient’s head, and the surgeon sits between patient’s legs for the procedure. First, the greater omentum is cut under a laparoscopic view. The right gastroepiploic vessels were clipped and cut, and the inflapyloric lymph nodes (No. 6) were dissected. The ligament of spleen and stomach was cut, and the No. 4 lymph nodes were dissected. After lymph node dissection, the duodenum is cut with a laparoscopic linear stapler.
- (c)
The lesser omentum is then cut, the right crus of the diaphragm is exposed, and the inflapyloric lymph nodes are dissected. The lymph nodes beside the proper hepatic artery (No. 8) are dissected. The left gastric artery, common hepatic artery, and the splenic artery are exposed. The left gastric vein is clipped and cut. The left gastric artery is divided after double clipping (Fig. 6.2). The lymph nodes along these vessels (No. 7, No. 8, and No. 9) are confirmed under excellent surgical view and then removed. Finally, the stomach is cut by the laparoscopic linear stapler.
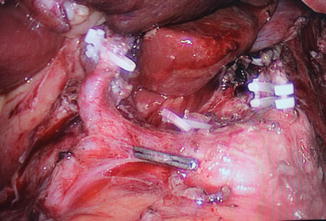
Fig. 6.2
The left gastric artery is divided after double clipping
Safe and effective digestive tract reconstruction is a crucial goal for laparoscopic radical gastrectomy. The basic principles for proper digestive tract reconstruction after laparoscopic gastric surgery include:
To improve the quality of life for patients with gastric cancer
To maintain the continuity of the digestive tract while simultaneously preserving its physiological function
To have reduced surgical complications
To allow for safe, quick, and easy operating procedures
At present, digestive tract reconstruction procedures for laparoscopic gastrectomy are divided into three types: total laparoscopic surgery, laparoscopic-assisted surgery, and hand-assisted laparoscopic surgery.
Laparoscopic distal gastrectomy for digestive tract reconstructive methods includes Billroth I, Billroth II, and Roux-en-Y anastomosis. Billroth I anastomosis is close to the normal physiological state: food goes through the duodenal, where mixing of duodenal juice, bile, and pancreatic juice occurs, and there is a reduction or complete avoidance of bile and/or pancreatic juice reflux into the gastric remnant. This approach reduces the occurrence of inflammation and/or cancer of the gastric remnant. On the other hand, Billroth I anastomosis can effectively stimulate cholecystokinin secretion as well as reduce the incidence of postoperative cholecystitis and cholelithiasis. Therefore, Billroth I anastomosis is the recommended method for the reconstruction of digestive tract after laparoscopic distal gastrectomy [9]. However, if the tumor is involved in the duodenum, Billroth II or Roux-en-Y anastomosis should be performed in order to ensure the radical resection of the tumor.
According to the current literature, the gastric digestive tract reconstruction after total gastrectomy amounts to more than 70 methods [10]. Despite this vast amount of work, the best way for digestive tract reconstruction is still unclear. However, according to the principle of “simple, safe, and effective,” more and more scholars recommend no pouch esophageal jejunal Roux-en-Y anastomosis after total gastrectomy [11–14]. Common laparoscopic anastomosis techniques for this approach include end-end esophago-jejunal anastomosis using an EST device and termino-lateral esophago-jejunal anastomosis using an OrVil device (Fig. 6.3). To this end, a continuous single-layer hand-sewn esophago-jejunal anastomosis (3.0 Vycril intracorporeal) could be performed.
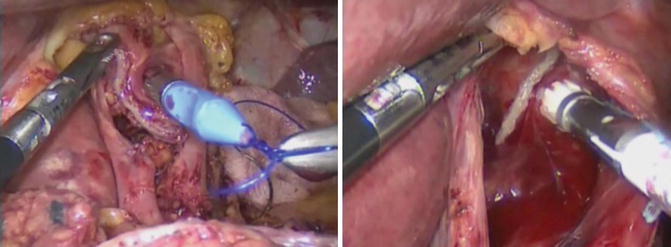
Fig. 6.3
(Left) End-end esophago-jejunal anastomosis using an EST device. (Right) End-lateral esophago-jejunal anastomosis using an OrVil device
6.1.4 Laparoscopic Surgery Outcomes
Laparoscopic surgery has been a known technique for more than 40 years. Within the past 20 years, laparoscopic surgery has revolutionized the field of gastric cancer surgery. It has shown to have significant advantages when compared to more traditional approaches, including lower trauma, reduced blood loss, quicker gut function recovery, shorter hospital stay length, and reduced incisional hernia rates [15–17].
Postoperative complications from laparoscopic surgery are similar to open gastrectomy surgery [16]. Exceptions include pneumoperitoneum-related complications, such as incision infection, intra-abdominal bleeding, duodenal stump leakage, and anastomosis leakage. Of these, the most common are duodenal leakage, anastomosis bleeding, and anastomosis leakage [18].
To evaluate long-term outcomes, a multicenter study comprised of 491 patients in 25 units was performed. Resulting statistical analyses showed that 93% were in Stage IA, 5% were in Stage IB, and 2% were in Stage II of the disease [18]. There were only six cancer recurrences (median follow-up time, 23 months), and the 5-year survival rate was 99.4%. In addition, the 5-year disease-free survival rates were 99.6% for Stage IA and 100% for Stage IB, which were the same as open gastrectomy.
In a separate study, Sato and colleagues studied 332 patients from January 2001 through December 2010 [19]. Of these, 47.6% (158) underwent laparoscopic surgery, while the remaining 52.4% (174) underwent open gastrectomy [19]. When comparing laparoscopic surgery to open gastrectomy with D1 and D1+ lymph node dissection, the mean operation time was significantly longer for the former. The rate of postoperative complications, morbidity, and recurrence was not significantly different between the two methods. However, the mean blood loss was significantly smaller with the laparoscopic surgery, and the average number of lymph nodes was significantly greater. Thus, laparoscopic surgery with D1 and D1+ lymph node dissection is as safe as open gastrectomy. To this end, Lee et al. studied 211 patients, of whom 106 underwent laparoscopic surgery and the remaining 105 underwent open gastrectomy [15]. Their report showed that the rate of postoperative complications with laparoscopic surgery was smaller than that of open gastrectomy. Additionally, postoperative recovery was significantly faster for patients who underwent laparoscopic surgery. To this end, they started a liquid diet sooner, and their postoperative hospital stays were shorter. Concerning long-term outcomes, the 5-year survival rate for laparoscopic surgery versus open gastrectomy was 95.9% and 94.9%, with no significant difference between the two. Collectively, these data suggest that laparoscopic surgery for EGC is feasible and safe. As a result, laparoscopic surgery has been included as one of the standard procedures in the Third edition of the Japanese gastric cancer treatment guidelines for the treatment of Stage I of the disease. Similarly, NCCN guidelines also recommend that patients with early gastric cancer undergo laparoscopic gastrectomy.
To further validate the laparoscopic approach, Korean-funded and Japanese-funded researches (KLASS and JCOG0912, respectively) have performed random control trials (RCTs) at multiple centers to compare the outcomes of laparoscopic and open surgery in early-stage gastric cancer patients [20, 21]. KLASS research demonstrated that there were no significant differences in complication rate and mortality of distal radical operation between the two groups. However, they were unable to draw any conclusions regarding long-term outcomes. Similarly, Korean-funded and Chinese-funded researches (KLASS II and CLASS, respectively) are currently underway to compare the outcomes of laparoscopic and open surgery in advanced gastric cancer patients [22, 23]. We eagerly look forward to the final results when they become available.
6.1.4.1 Limitations of Laparoscopic Surgery
Despite its many advantages, laparoscopic gastrectomy for gastric cancer has some major disadvantages compared with the open gastrectomy. First is the missing haptic perception, which is important in some fields of gastrointestinal surgery. Since neither the liver nor the small bowel can be palpated during laparoscopy without haptic perception. The second disadvantage is the limited field of surgical vision. Some procedures especially in the handling of intraoperative complications (bleeding, hurting small bowel, and so on) are more difficult in laparoscopic surgery when compared to open surgery due to the limited intra-abdominal space [24].
6.1.4.2 Laparoscopic Sentinel Lymph Node Navigation Surgery
Recently, large-scale prospective studies demonstrated that laparoscopic sentinel lymph node mapping and biopsy was safe and beneficial for early-stage gastric cancer patients [25, 26]. The author also performed the sentinel lymph node biopsy in early gastric cancer patients using ICG (Fig. 6.4). This kind of surgery uses either ICG or nanoparticles to assess the lymphatic drainage from lymph channels to sentinel lymph node. The sentinel lymph node navigation surgery (SNNS) diagnostically identifies the sentinel lymph nodes and resects them using a laparoscopic surgical approach. A recent study reported that the detection rate, sensitivity, and accuracy for Stage I gastric cancer was 97.5%, 93%, and 99%, respectively. The false negative rate was only 1% [27].
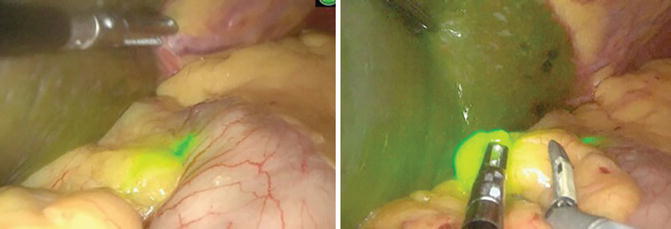
Fig. 6.4
Application of ICG in a gastric cancer patient to assess lymphatic drainage from lymphatic vessels to sentinel lymph nodes (left, ICG accumulated in lymphatic vessels; right, ICG accumulated in sentinel lymph nodes)
However, some studies have reported that the benefits of SLN navigation are limited [28, 29]. These studies reported that laparoscopic lymphadenectomy may not improve the patients’ postoperative quality of life (QOL).
Some researchers have undertaken studies related to sentinel lymph node tracing [25–27]. Although the Japan Clinical Oncology Group trial (JCOG0302) was terminated due to high rates of false negatives, another clinical Phase II trial in Japan initially confirmed the feasibility of sentinel lymph node tracing as applied to gastric cancer [30, 31]. The Korea Phase III SENORITA trial sought to determine the presence of lymph node metastasis by endoscopic injection of 99TCm and subsequent ICG around the tumor [32]. The results of this study will further aid in determining whether sentinel lymph node tracing is applicable for treatment of gastric cancer, thus making surgical resection of early gastric cancer more plausible, accurate, and individualized.
6.2 Robotic Surgery for Gastric Cancer
6.2.1 Introduction
Robotic surgery has rapidly become one of the standard treatments for early-stage gastric cancer. Since robot-assisted gastrectomy was first reported in 2003, many studies have demonstrated its safety, efficacy, and significantly reduced invasiveness when compared to other approaches [33–35]. Robotic gastric cancer surgery including total gastrectomy with D2 lymph node dissection and radical subtotal gastrectomy is technically feasible and safe [35]. The indication for robotic surgery for gastric cancer is similar to that for laparoscopic surgery for Stage I gastric cancer.
6.2.2 Potential Advantages of Robotic Surgery
Robotic surgery for gastric cancer has shown increasing applications in experienced surgical centers [36]. Robotic surgery offers the surgeon the benefit of the freedom of free wrist function, the superior 3D visualization, and the easy control of robotic arms. When compared to laparoscopic surgery, the results of short-term outcomes have been shown to be similar [37]. Due to the technical advantages, the robotic surgical device may facilitate the expansion of minimally invasive surgery over laparoscopy. The potential advantages of robotic surgery include performing an extended lymphadenectomy to the lymph node (itself a difficult dissection) and performing an anastomosis under excellent surgical view [36].
The da Vinci robot-assisted surgical system is the most widely used robotic surgical platform (Fig. 6.5). Its technical advantages include eliminating hand tremor, setting the action scaling, and indexing actions. The high-definition, 3D stereo-images transferred by the system are high resolution and have achieved real three-dimensional depth of field. Three emulated mechanical wrists have different types of free activities, and the range of motion of each joint exceeds 90°, making them more interactive than human hands (Fig. 6.5). Therefore, this system has greatly improved surgical stability, accuracy, and safety. Currently, da Vinci robot-assisted surgery within the realm of gastric cancer operations is still confined to just a few countries.