Everybody gets so much information all day long that they lose their common sense.
—Gertrude Stein, American writer (1874-1946)
Primary Care Physicians Are the Cornerstone for Diabetes Care in the United States
Management of the patient with diabetes mellitus—a chronic, progressive, and potentially disabling illness—epitomizes the spirit of primary care medicine. Although specialists are often asked to evaluate and treat patients who have advanced complications or require complex treatment regimens, 90% of patients with diabetes can successfully be managed in a primary care setting.1,2 Primary care physicians (PCPs) can screen high-risk patients for diabetes, initiate treatment to reduce hyperglycemia, monitor and fine-tune pharmacologic therapies, as well as detect and manage microvascular and macrovascular complications. Family physicians also provide a portal for important life-altering information to their patients, such as access to certified diabetes educators (CDEs) and registered dietitians (RDs).
We are our patients’ first line of defense for ensuring that their pregnancies have favorable outcomes, when we begin to discuss preconception planning with adolescents with diabetes. Armed with the knowledge that eating disorders are frequently encountered in adolescent patients with type 1 diabetes mellitus (T1DM), we are able to elicit a history of the “danger signs” that are suggestive of this dangerous behavior pattern. Athletes seek our advice on how to manage their medication therapy when they are training for a marathon or seeking to join the high school football team. We are on the front lines for patients complaining of sleep disorders.
As specialists in the management of chronic disease states, we understand the frustrations that our patients express in wanting to “eliminate” medications on each visit because their metabolic targets may actually be improving. Unfortunately, modifying a disease state does not translate into a cure. Diabetes is a chronic progressive disease often coexisting with hypertension, hyperlipidemia, atherosclerosis, major depression, sleep disorders, obesity, painful neuropathy, and sexual dysfunction. Some fortunate individuals actually manage to navigate through the “mine fields of glycemic burden” unscathed and develop no long-term microvascular or macrovascular complications. Others may start as role models for other patients by maintaining near normal metabolic control for years, only to develop neuropathy, cancer, Parkinson disease, or hearing loss later in life.
Because PCPs monitor every aspect of their patient’s metabolic history, we should not hesitate to share this information openly with other specialists. Imagine the appreciation an ophthalmologist would likely show if a patient arrived at his or her office complete with an updated medical history, A1C level, and lipid panel. Most specialists are forced to provide patient care without having access to this information, which may delay the integration of certain therapies into the patient’s treatment regimen. For example, how could a nephrologist offer any advice to a patient who says only, “My doctor sent me to you because he thinks my kidneys are failing. But honestly, I feel just fine!” Where is the patient’s estimated glomerular filtration rate (eGFR), hemoglobin, A1C level, serum calcium, intact parathyroid hormone level, or test for urinary albumin excretion? What medications is the patient taking? Is there a family history of chronic kidney disease? Does the patient have hypertension or hyperlipidemia? Is the patient smoking? Timely and comprehensive communication with specialists not only enhances coordination of care, but minimizes the liklihood of subjecting patients to redundant or costly testing procedures..
PCPs have a unique opportunity to evaluate, predict, and prevent many of the devastating long-term complications associated with diabetes. Simply identifying patients at high risk for diabetes developing based on their family history, ethnicity, history of gestational diabetes, or body-fat distribution should warrant the introduction of lifestyle and behavioral interventions that could delay or prevent the onset of diabetes. Intensive and customized management designed to normalize hyperglycemia and other metabolic anomalies early in the course of the disease can improve outcomes.3,4,5
• The Diabetes Pandemic
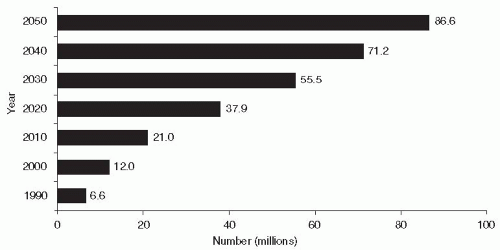
Twenty-six million Americans have diabetes and an additional 79 million Americans are estimated to have prediabetes. Approximately 5% to 10% have T1DM, 90% to 95% have type 2 diabetes mellitus (T2DM), and 1% to 5% are diagnosed with disorders such as gestational diabetes, monogenetic diabetes (MODY), or secondary causes of diabetes such as cystic fibrosis. With increasing numbers of the obese, the elderly, and members of higher-risk minority groups in the population, prevalence is increasing.6 Twenty-seven percent of all patients with diabetes, and 7 million Americans with prediabetes are unaware that they are afflicted with the disorder.6 Projections from the CDC indicate that the prevalence of diabetes is likely to increase fourfold within the next 40 years. By 2030, 55.5 million adults aged 18 to 79 years will have diabetes with the prevalence rising to 86.6 million adults by 2050. Assuming an adult population of 306 million and an undiagnosed diabetic population of 13.7 million in 2050, as many as one in three adults in the United States will have diabetes by midcentury (Fig. 1-1).7
A study conducted by the Institute for Alternative Futures (IAF) identified California, Texas, Florida, New York, Ohio, Illinois, Georgia, Pennsylvania, North Carolina, and Michigan as “diabetes hot spots,” where the burden of diabetes will be greatest within the next 15 years.8 The IAF diabetes model estimates that the overall number of people in the United States living with diabetes will increase 64% by 2025 to 53.1 million. This equates to one in seven Americans. The resulting medical and societal cost of diabetes will be almost $514 billion—a 72% increase from 2010 and comparable to the total budget for Medicare in 2010.9
Currently, the 10 states identified as diabetes hot spots shoulder nearly 60% of the cost from diabetes or approximately $176 billion of the total $299 billion. In 15 years, the aggregate direct cost of diabetes care to these 10 states is projected to jump to $297 billion, nearly exceeding the entire cost of diabetes care within the entire United States today.8 (The prevalence and cost of diabetes for each of the 50 states plus 13 major metropolitan areas for the years 2000, 2010, 2015, and 2025 may be found at www.altfutures.org/diabetes2025.)
These projections provide further insight into the growing threat of diabetes toward public health. The burden for preventing, screening, and managing diabetes will lie within the primary care domain. Cost may best be mitigated by preventing costly long-term complications. This will require cost-effective disease prevention programs targeting high-risk populations. High-risk patients will require customized programs designed to encourage the adaptation of healthy lifestyle changes into one’s daily routine. Lifestyle intervention is the least expensive of all diabetes intervention programs, yet the most difficult to initiate and maintain over time. For clinicians who believe changing behaviors should be second nature, try brushing your teeth with your opposite hand. Not so easy to do. Right?
Figure 1-1 • Estimated Prevalence of Diagnosed Type 2 Diabetes in the United States from 1990 to 2050 From 2010 through 2050 the prevalence of T2DM in the United States will increase fourfold with one in every three adults becoming diagnosed with the disorder. (An increase in diabetes prevalence rates of 165%.) Reference: Boyle JP, Thompson TJ, Gregg EW, et al. Projection of the year 2050 burden of diabetes in the U.S. adult population: dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul Health Metr. 2010;8:29; National Diabetes Information Clearinghouse: http://diabetes.niddk.nih.gov/dm/pubs/overview/#scope. Accessed October 20, 2011.
Rates of diabetes are increasing worldwide. At least 171 million people currently have diabetes, and this figure is likely to more than double to 366 million by 2030. The top ten countries, in numbers of people with diabetes, are currently India, China, the United States, Indonesia, Japan, Pakistan, Russia, Brazil, Italy, and Bangladesh. The greatest percentage increase in rates of diabetes will occur in Africa over the next 20 years. At least 80% of people in Africa with diabetes are undiagnosed, and many in their 30s to 60s will die from diabetes in that continent.10
The prevalence of T2DM varies widely among various racial and ethnic groups. T2DM is more prevalent among Hispanics, Native Americans, African Americans, and Asians/Pacific Islanders than in non-Hispanic whites. Indeed, the disease is becoming virtually pandemic in some groups of Native Americans and Hispanic people. T2DM is less common in non-Western countries where the diet contains fewer calories and daily caloric expenditure is higher. However, as people in these countries adopt Western lifestyles, weight gain and T2DM are becoming virtually epidemic.
Diabetes Prevalence is Increasing in Children and Adolescents
PCPs are observing an increase in the incidence of T2DM within their adolescent patient population, particularly in high-risk racial and ethnic groups. New onset T2DM now accounts for 8% to 45% of all pediatric diabetes cases.11 In the years 2002 to 2005, among children and adolescents aged 10 to 19 years, the estimated rate of new cases of T1DM was 18.6 per 100,000 per year, compared with the estimated rate of new cases of T2DM of 8.5 per 100,000 per year.12
Not infrequently, adolescents who are diagnosed with T2DM have evidence of islet autoimmunity (see Table 1-1). Obese adolescents with T2DM who are autoantibody positive have severe insulin deficiency and pancreatic β-cell failure as opposed to those who test antibody negative.13 The presence or absence of autoantibodies in children or adolescents will distinguish whether the patient has T1DM or T2DM. Any patient with clinical evidence of diabetes who tests autoantibody negative should be diagnosed as having T2DM (Table 1-1).14
Obesity in adolescents is the environmental trigger that ignites the fuse of the overworked and overstressed pancreatic β-cells. The body may respond in one of two ways to this growth-induced physiologic stress. As in adults, individuals with “super β-cell” are able to produce enough insulin to maintain euglycemia for a prolonged period of time. Those patients who progress to clinical diabetes fall victim to the “accelerator hypothesis,” which contends that β-cell function and mass are genetically programmed to fail over time. Patients who develop diabetes are simply unable to maintain normal β-cell function over time. Those individuals who elicit an autoimmune response within their islets will progress more rapidly toward chronic hyperglycemia and become ketosis prone against a background of obesity and insulin resistance. Exogenous physiologic insulin replacement therapy will be needed in these patients15
TABLE 1-1. Differentiating T1DM and T2DM in Young Patients
Diagnostic Characteristic
T1DM
T2DM
Weight
20% may be overweight.
Virtually all BMI > 85th percentile for age
Typical clinical course
Usually rapid onset
35%-40% present with diabetic ketoacidosis.
Slow onset
Ketonuria at diagnosis = 33%
Mild DKA at diagnosis = 5%-25%
Other presenting symptoms include blurry vision, monilial vaginitis, polyuria, and polydipsia.
Hyperglycemic, hyperosmolar, nonketotic state may be life threatening.
Genetic predisposition
5% with T1DM
Up to 30% may have with T2DM.
A family history of T2DM increases risk of T1DM two- to threefold.
Adapted from Tfayli H, Bacha F, Gungor N, et al. Phenotypic type 2 diabetes in obese youth: insulin sensitivity and secretion in islet cell antibody-negative versus -positive patients. Diabetes. 2009;58:738-744.
Lifestyle modification remains the treatment of choice for adolescents with T2DM. Long-term outcome studies evaluating the safety and efficacy of intensive dietary and exercise therapies versus pharmacotherapies have not been performed in the adolescent population. However, few could argue that some weight reduction with guidance provided by a certified diabetic educator or a registered dietitian is undesirable. PCPs should insist that patients eliminate sugary drinks and highcaloric foods from their daily diets. Meal skipping may become a precursor to disordered eating behaviors. Daily exercise should be encouraged. Determining the true benefits of adapting healthy lifestyle changes is problematic as approximately 65% of adolescent patients with T2DM treated with lifestyle intervention alone are lost to follow-up.16
Currently, metformin is the only FDA-approved oral agent for the management of T2DM in children and adolescents.17 In a randomized placebo-controlled trial of metformin in adolescents with new-onset T2DM, metformin treatment resulted in a significantly lower A1C after 16 weeks compared with placebo (7.5% vs. 8.6%).18 Metabolic surgery may be considered for patients with T2DM having a BMI greater than 35 kg per m2 in association with serious comorbidities (sleep apnea, heart disease, and hypertension, which is discussed in detail in Chapter 10).
Comorbid hyperlipidemia in adolescent patients with T2DM must also be managed aggressively. The accepted targeted goals include an LDL-C of less than 100 mg/dL, triglycerides less than 150 mg/dL, and HDL-C greater than 35 mg/dL. Pharmacotherapy for LDL with a statin should be considered when the LDL-C is greater than 160 mg/dL. Statin therapy has been shown to be safe and effective in adolescent patients. Triglyceride levels greater than 1,000 mg/dL should be treated with a fibric acid to reduce the risk of pancreatitis.19
The differences in response to treatment and prevention of long-term complications between obese adolescent patients with either T1DM or T2DM have yet to be clearly determined.
Can Primary Care Providers Make a Positive Impact on National Trends Related to Diabetes Care?
The National Health Survey Act of 1956 established an effective means by which the continued assessment of the health and welfare of U.S. citizens could be evaluated.20 Since 1959, eight separate surveys, evaluating over 130,000 individuals have been completed under the supervision of the Department of Health and Human Services. Originally, two separate surveys on nutrition and health issues were conducted. In 1970, the National Nutrition Surveillance System and the National Health Examination were combined to form the National Health and Nutrition Examination Survey (NHANES).
NHANES data are collected by “probability sampling.” The country is divided into geographic areas, known as “primary sampling units” (PSUs). The PSUs are then combined to form strata that are divided into a series of neighborhoods. Inhabitants living within these neighborhoods are chosen randomly to determine their eligibility for NHANES participation. In theory, each selected participant represents approximately 50,000 comparable U.S. residents. Eligible participants are referred to local mobile examination centers where they undergo comprehensive historical interviews, physical examinations, and laboratory studies. (The diabetes questionnaire for NHANES 2008 may be accessed at http://www.cdc.gov/nchs/nhanes/nhanes2007-2008/DIQ_E.htm#DIQ190C.)
NHANES provides important insight into many chronic disease states including obesity, diabetes, arthritis, cardiovascular disorders, COPD, cholelithiasis, kidney disorders, osteoporosis, and cancer. Data obtained from NHANES are used by researchers, health care professionals, and public health officials to design a variety of public health initiatives directed at improving the health outcomes of U.S. citizens.
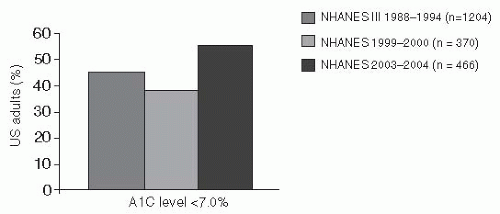
NHANES data have demonstrated that glycemic control in the United States has actually improved substantially from 1999 through 2004. In 1999, only 37% of patients achieved the ADA desired A1C target of less than 7%, whereas in 2004, 55.7% of individuals were successful at attaining an A1C below 7% (Fig. 1-2). This important achievement also proposes that a 0.5% reduction in A1C when maintained over 10 years would produce a 10.7% reduction in diabetes complications while improving all-cause mortality and direct costs attributed to glycemic burden.21
Figure 1-2 • Adults with Previously Diagnosed Diabetes Achieving ADA-recommended A1C Goal ADA, American Diabetes Association; NHANES, National Health and Nutrition Examination Survey. Reference: National Institutes of Health. The National Diabetes Education Program: 10 years of progress 1997-2007. August 2007. Available at: www.ndep.nih.gov/media/ndep_progressrpt07.pdf. Accessed December 22, 2011.
Much of the efforts for improving the outcomes of patients with diabetes are attributed to the efforts of primary care providers who supervise and deliver care to over 90% of all patients with diabetes in the United States. Just as the NHANES data have demonstrated a nearly 19% improvement in the number of patients achieving their ADA recommended A1C target of less than 7%, the U.S. health care system is experiencing critical shortages of primary care clinicians. Those PCPs who remain on the front lines of diabetes care are the target of incessant political debates as to the most cost-effective and rational means by which health care may be delivered equally to all people living in the United States. Physicians have had to invest in electronic medical records, e-prescribing, and software to achieve 25 Meaningful Use objectives. More importantly, what health care delivery systems might prove the most beneficial for society as a whole? Should the responsibility for cost-effective health care delivery be placed in the hands of the private sector or the government? With 60% of the adult population expected to have diabetes by year 2050, implementation of novel health care systems is imperative. PCPs should carefully evaluate the risks and benefits of any fundamental change suggested to their existing practice prior to enrolling in an alternative and untested program. Let us take a look at some of the controversial aspects of health care delivery in the United States today as it relates to diabetes management and primary care.
Patient-centered Medical Homes: Offering Privatization of Medical Care
An estimated 65 million Americans live in officially designated primary care shortage areas. The number of medical students entering adult primary care careers in internal and family medicine is on the decline. The United States spends more on specialist care per capita than any other industrialized country.22 Coordination of patient care between PCPs, specialists, and hospitals is also deficient in many communities. Patients lack the sophistication to optimize their own pharmacologic treatment plans when prescribed medications by multiple providers.
In today’s economic environment, one is hard pressed to provide cost-effective and efficient care to every patient with diabetes who becomes integrated into one’s practice. Still, several patient-centered primary care-based groups have developed innovative health-care delivery models which have proven to be cost-effective while improving outcomes.
Patient-centered medical homes (PCMHs) provide a health care setting that facilitates partnerships between individual patients, their personal PCP, and a team of medical professionals. Medical homes assure that patients acquire the care that is most appropriate in a timely manner while taking into account one’s individual cultural and linguistic orientation.
TABLE 1-2. Services Provided by Medical Family Homes
•
Primary care advocacy for patients who are members of the medical home
•
Appropriate, timely, and evidence-based interventions for both acute and chronic illnesses
•
Initiation and integration of psychological counseling as well as behavioral interventions for patients with mental illness and chronic diseases, which, in theory, will improve long-term outcomes and adherence to treatment regimens
•
Reproductive care that may be directed by qualified PCPs
•
Integrated care in conjunction with specialists and adjunctive therapists if required
•
Supportive care provided within hospitals, home, community, or nursing homes by PCPs and ancillary staff members
•
Emphasis toward education and support for self-care and preventive care
•
End-of-life support for terminally ill patients and their families
•
Service coordination and referral, the goals of which are to allow patients to attain timely and appropriate consultation
•
No co-pays, co-insurance, or deductibles
•
Unhurried 30- to 60-min office visits
•
Phone consultations and e-mail access to primary care providers
•
Onsite pharmacy
Adapted from Rossner WW, Colwill JM, Kasperski J, et al. Progress of Ontario’s family health team model: a patient-centered medical home. Ann Fam Med. 2011;9:165-171.
The services to patients with diabetes provided by a PCMH are summarized in Table 1-2. The primary corporate objectives of PCMH include the following:
Access to a personal trusting physician who directs a medical team responsible for the patient’s care.
Patient care should maintain “whole-person orientation.” Patients with diabetes would be comanaged with a certified diabetic educator, a pharmacist to make certain the patient is adherent to their pharmacologic regimen, a behavioral interventionist when necessary, and timely specialist referral.
Preventive care is the core benefit provided by PCMH.
Equally important is the desire of the medical home to assure that the patient is satisfied with the care and consultations that are being provided to him or her.
Corporate philosophy of medical homes recognize the value that PCPs add to their patient’s well-being, especially if patients are afflicted with a chronic progressive disease such as diabetes. As such, physicians are compensated based on productivity. Patients within a medical home will pay monthly “membership fees” allowing them 24/7 access to their PCP. The membership fee allows physicians to see fewer patients per day while providing more comprehensive care to each person. Satisfaction for this practice model among patients and staff members is passionate within the medical homes.
Medical homes were initially established in 1967 as a means of caring for chronically ill children. Over the past 7 to 10 years, the medical home movement in association with a flourishing primary care environment has validated a means by which more Americans can access care for both acute and chronic illnesses while reducing overhead medical costs.23
Prior to achieving a designation as an official medical home, a primary care practice must achieve standards at three different levels including 30 separate elements of certification by the National Committee for Quality Assurance (NCQA) (Table 1-3).
TABLE 1-3. NCQA Standards Used to Designate Medical Homes in the United States
Access and communication
Has written standards for patient access and patient communication.
Uses data to show standards for patient access and communication are being met.
Patient tracking and registry
Uses paper or electronic-based charting tools to organize clinical information.
Uses data to identify important diagnoses and conditions in practice.
Care management
Adopts and implements evidence-based guidelines for three conditions.
Patient self-management support
Actively supports patient self-management.
Test tracking
Tracks tests and identifies abnormal results systematically.
Referral tracking
Tracks referrals using a paper-based or electronic system.
Performance reporting and improvement
Measures clinical and service performance by physician or across the practice.
Reports performance across the practice or by physician.
More than 100 demonstration projects have already confirmed the effectiveness of the PCMH concept with a variety of approaches and populations. A study comparing claims data from 2010 of noted declines of 35% to 82% in ER visits, hospitalizations, hospitalization days, specialty visits, and surgeries of patients enrolled in a Washington-based medical home (Qliance Medical Group) with that of traditionally managed patients.24
Group Health—a Seattle-based nonprofit health insurance venture—encompasses a clinic of 8 physicians and 9,200 patients. After becoming designated as a medical home, standard visit times were increased from 20 to 30 minutes and staffing levels were expanded for other member services. Within 1 year, clinician work experience and clinical quality of care improved.25 Substantial upfront investments were recouped due to a decline in ER visits, urgent care visit, and acute hospitalizations.25 Group Health estimates a return of investment of $1.50 for every $1 invested in its medical home.22
Pay for performance within medical homes are based on a number of biomatrix standards including the number of patients screened for lipids, A1C levels, albuminuria, colon cancer, diabetic retinopathy, chronic kidney disease, peripheral neuropathy, pap smears, mammograms, osteoporosis, smoking history, and family history of diabetes-related complications. Additional financial incentives are provided to cover the cost of “high-risk patients” including those with mental illness or those who have a history of frequent hospitalizations or nonadherence to pharmacotherapy. Some medical homes are reimbursed for sending reminder cards to patients related to preventive services or appointments.26
Critics might argue that members might be confused about the “philosophy” of being a member of a medical home. This confusion might limit the cost-effectiveness of these ventures. However, unlike Accountable Care Organizations (ACOs), patients of medical homes are fully aware that they are members of that specific medical care service provider. ACO patients may not be informed of their membership and are free to seek medical care through a provider without affiliation to their assigned ACO.
Medical homes that are operated by privately funded PCPs have a tremendous potential for improving access to care and long-term outcomes for patients with all chronic illnesses including diabetes. Successful implementation of the medical home model in the United States will require PCPs to integrate both acute and preventive care for their chronically ill patients who have diabetes. An interdisciplinary team with behavioral medicine, pharmacists, midlevel care providers, and specialists must rely upon an integrated electronic medical record system to track data from point of care visits and long-term outcomes. Finally, providers will need to become “high-level customer service representatives.” Customized, cohesive, and targeted care for patients with diabetes will be supervised by the PCP, some of whom have been trained as thought leaders in the field of diabetes. Patients must accept their providers as their teachers, advocates, and disease coaches rather than just prescription writers for insulin, metformin, and test strips.
The United States faces major shortages of PCPs for care of adults. If the current U.S. primary care practice model continues as it is today, 44,000 additional family physicians and general internists would be needed in 2025 to maintain the current number of visits for each adult as the population increases and ages.27 An additional 3,000 PCPs would be required to begin practicing annually in order to achieve this goal. Adoption of PCMHs could become part of the solution to reduced primary care availability and services. With fewer PCPs to manage the burgeoning diabetes population, one could anticipate that patients will not initiate treatment until their disease state is further advanced and complications less amenable to reversal.
• Accountable Care Organizations: The Government’s Solution to Diabetes Health-Care Delivery
One fundamental flaw of the U.S. health care system is failing to reward health-care providers who work proactively to prevent chronic diseases from occurring or progressing. Instead, compensation favors clinicians who see patients more frequently, request more ancillary services, and perform more costly procedures on patients who have expensive chronic disorders. There is little doubt that the best health-care delivery system in the world is facing major financial hurdles in the next decade. Under current law, Medicare spending, the largest health-care purchaser and largest driver of federal entitlement costs and federal debt, is expected to rise from $523 billion in 2010 to $932 billion in 2020.28 Medicare’s long-term unfunded liabilities—the total cost of benefits promised but not paid for—amount to an incredible $36.8 trillion!29 Facing this unimaginable deficit, Congress decided to come up with a program for managing Medicare health-care delivery that could not lose a dime… at least for the Medicare Trust Fund! Let us now take a look at the Government mandated Accountable Care Organizations. As we do, ask yourselves if ACOs will likely add to the successful management of patients with chronic diseases such as diabetes. Also, if you were a senior patient on Medicare, who would you rather have as your health-care provider: a primary care medical home or an ACO?
ACOs take up only seven pages of the massive 1990-page proposed affordable health act, but has become one of the most befuddling of all provisions. Hospital and provider groups are preparing to form ACOs despite outwardly complaining that this program has created more risks than rewards while imposing onerous reporting requirements.
The ACOs are being promoted, at least in theory, as a means by which health-care costs may be contained while improving overall quality of care for millions of Americans. From a philosophical, or mythologic, perspective (if you prefer), ACOs will be developed to realign payment incentives by shifting the focus from high patient care to one of value and performance.30 Similar to medical homes, the ACOs want doctors to “voluntarily” see fewer fee-for-service patients, while documenting various quality measures of high performance with each individual.
The Centers for Medicare and Medicaid Services (CMS) define an ACO as “an organization of health-care providers that agrees to be accountable for quality, cost, and overall care of Medicare beneficiaries who are enrolled in the traditional fee-for-service program who are assigned to it.”31 ACOs that succeed in delivering high quality care and reducing health care costs will receive a share of the money the government saves on patients registered to that ACO. The Department of Health and Human Services predicts that ACOs could save Medicare up to $940 million during the first 4 years of its implementation, which is far less than 1% of Medicare’s anticipated spending during that same period!
ACOs will include physicians working in group practices or networks of practices and hospitals. ACOs must have at least 5,000 patient “beneficiaries” as well as the technologic ability to report data on cost and quality for Medicare fee-for-service patients. As in the classic movie “The Dirty Dozen,” every ACO will attempt to unify a large group of providers with a hospital or several hospitals, some of whom are fierce local or regional competitors, for the benefit of all. With so many political adversaries and self-interests involved in local and regional medical politics, many insiders believe that the ACO concept will be doomed to failure.
In Medicare’s traditional fee-for-service payment system, doctors and hospitals are compensated based upon the number of tests and procedures they perform. This incentivizes physicians to order more ancillary services and procedures that will increase their income. Remember, ACOs want doctors to spend MORE quality time with patients, but doctors know that in a fee-for-service enterprise, the winners are those that schedule the most appointments. Perhaps if doctors schedule fewer patients, hospitalizations, and surgery numbers will also decrease and money will be saved.
ACOs would continue the same traditional fee-for-service program, while creating savings incentives that they hope would pay bonuses to frugal doctors over the long term. Savings in health care costs would be derived from groups of physicians who see fewer patients, order fewer tests, keep their patients out of the hospital, and reduce the number of invasive procedures individuals may require.
But wait! Congress was smart when they legislated the ACO program. There could be only one loser in this game and two winners. If costs could NOT be contained, or if performance and savings benchmarks were not met, the ACO would be responsible for all penalties… not the government! After all, Medicare has $36.8 trillion in unfunded liabilities. Why should this entitlement program take on any additional debt when liability can be passed on to a third party? If, by chance, the ACO was profitable, incentive bonuses would be provided to the members. Some rural ACOs may be eligible to receive government start-up costs in advance to help them build the infrastructure necessary for coordinated care. Before any ACO members get excited about these bonuses, the government intends to withhold distribution of any funds for up to 2 years, making certain that all of the patient costs have been appropriated.
The government will begin receiving its initial round of applications for the ACO Shared Savings Program in January 2012, and the first ACOs are expected to launch in April. CMS created a second strategy, called the Pioneer Program, allowing high-performing health systems to potentially recover more of the expected health care savings in exchange for accepting greater financial risk.
Table 1-4 lists the variables and reservations related to ACO development and strategic planning. Prior to contracting with an ACO, providers are strongly encouraged to consider the risks and benefits of working within the confines of these organizations.
Has the ACO concept undergone performance field testing? The “Physicians Group Practice Demonstration” was a directive originally decreed by Congress in 2000 designed to field test a system by which physicians who accepted traditional fee-for-service patients could be rewarded for their high-quality and cost-effective medicine.32 The project was eventually launched after 5 years of bureaucratic delays. Ten of the most respected large multispecialty groups in the country were selected as test sites including the Marshfield Clinic, St. John’s, Geisinger, Park Nicollet, and Billings. Two pilot sites were associated with academic medical centers—the University of Michigan and Dartmouth.
Physician groups in the demo continued to receive their regular Medicare compensation while sharing in any savings generated. Each group had to attain 32 predetermined quality metrics and exceed a savings threshold of 2%. By the 4th year of the demo, all 10 groups met at least 29/32 quality goals and by the 5th year, 7 groups achieved benchmark-level performance on all 32 measures. All PGPs increased their quality scores on diabetes management by at least 9% over 5 years.
Only gold members can continue reading. Log In or Register to continue