We should study “the benefits of medical interventions in relation to their hazards and costs.”
—Kerr L. White 1992
KEY WORDS
Clinical epidemiology
Clinical sciences
Population sciences
Epidemiology
Evidence-based medicine
Health services research
Quantitative decision making
Cost-effectiveness analyses
Decision analyses
Social sciences
Biologic sciences
Variables
Independent variable
Dependent variable
Extraneous variables
Covariates
Populations
Sample
Inference
Bias
Selection bias
Measurement bias
Confounding
Chance
Random variation
Internal validity
External validity
Generalizability
Shared decision making
Example
A 51-year-old man asks to see you because of chest pain that he thinks is “indigestion.” He was well until 2 weeks ago, when he noticed tightness in the center of his chest after a large meal and while walking uphill. The tightness stopped after 2 to 3 minutes of rest. A similar discomfort has occurred several times since then, sometimes during exercise and sometimes at rest. He gave up smoking one pack of cigarettes per day 3 years ago and has been told that his blood pressure is “a little high.” He is otherwise well and takes no medications, but he is worried about his health, particularly about heart disease. He lost his job 6 months ago and has no health insurance. A complete physical examination and resting electrocardiogram are normal except for a blood pressure of 150/96 mm Hg.
This patient is likely to have many questions. Am I sick? How sure are you? If I am sick, what is causing my illness? How will it affect me? What can be done about it? How much will it cost?
As the clinician caring for this patient, you have the same kinds of questions, although yours reflect greater understanding of the possibilities. Is the probability of serious, treatable disease high enough to proceed immediately beyond simple explanation and reassurance to diagnostic tests? How well do various tests distinguish among the possible causes of chest pain: angina pectoris, esophageal spasm, muscle strain, anxiety, and the like. For example, how accurately will an exercise stress test be in either confirming or ruling out coronary artery disease? If coronary artery disease is found, how long can the patient expect to have the pain? How likely is it that other complications—congestive heart failure, myocardial infarction, or atherosclerotic disease of other organs—will occur? Will the condition shorten his life? Will reduction of his risk factors for coronary artery disease (from cigarette smoking and hypertension) reduce his risk? Should other possible risk factors be sought? If medications control the pain, would a coronary revascularization procedure add benefit—by preventing a future heart attack or cardiovascular death? Since the patient is unemployed and without health insurance, can less expensive diagnostic workups and treatments achieve the same result as more expensive ones?
Clinical Questions and Clinical Epidemiology
The questions confronting the patient and doctor in the example are the types of clinical questions at issue in most doctor-patient encounters: What is “abnormal”? How accurate are the diagnostic tests we use? How often does the condition occur? What are the risks for a given disease, and how do we determine the risks? Does the medical condition usually get worse, stay the same, or resolve (prognosis)? Does treatment really improve the patient or just the test results? Is there a way to prevent the disease? What is the underlying cause of the disease or condition? and How can we give good medical care most efficiently? These clinical questions and the epidemiologic methods to answer them are the bedrock of this book. The clinical questions are summarized in Table 1.1. Each is also the topic of specific chapters in the book.
Clinicians need the best possible answers to these kinds of questions. They use various sources of information: their own experiences, the advice of their colleagues, and reasoning from their knowledge of the biology of disease. In many situations, the most credible source is clinical research, which involves the use of past observations on other similar patients to predict what will happen to the patient at hand. The manner in which such observations are made and interpreted determines whether the conclusions reached are valid, and thus how helpful the conclusions will be to patients.
Health Outcomes
The most important events in clinical medicine are the health outcomes of patients, such as symptoms (discomfort and/or dissatisfaction), disability, disease, and death. These patient-centered outcomes are sometimes referred to as “the 5 Ds” (Table 1.2). They are the health events patients care about. Doctors should try to understand, predict, interpret, and change these outcomes when caring for patients. The 5 Ds can be studied directly only in intact humans and not in parts of humans (e.g., humeral transmitters, tissue cultures, cell membranes, and genetic sequences) or in animals. Clinical epidemiology is the science used to study the 5 Ds in intact humans.
What conditions lead to disease? What are the origins of the disease?
aFour chapters—Risk: Basic Principles (4), Chance (11), Systematic Reviews (13), and Knowledge Management (14)—pertain to all of these issues.
In modern clinical medicine, with so much ordering and treating of lab test results (for such things as plasma glucose levels, hematuria, troponins, etc.), it is difficult to remember that laboratory test results are not the important events in clinical medicine. It becomes easy to assume that if we can change abnormal lab tests toward normal, we have helped the patient. This is true only to the extent that careful study has demonstrated a link between laboratory test results and one of the 5 Ds.
A set of symptoms, physical signs, and laboratory abnormalities
Discomfort
Symptoms such as pain, nausea, dyspnea, itching, and tinnitus
Disability
Impaired ability to go about usual activities at home, work, or recreation
Dissatisfaction
Emotional reaction to disease and its care, such as sadness or anger
aPerhaps a sixth D, destitution, belongs on this list because the financial cost of illness (for individual patients or society) is an important consequence of disease. b Or illness, the patient’s experience of disease.
Example
The incidence of type 2 diabetes mellitus is increasing dramatically in the United States. Diabetics’ risk of dying from heart disease is two to four times greater than that among people without diabetes, and cardiovascular disease accounts for approximately 70% of all deaths in diabetic patients. New pharmacologic efforts to control diabetes have produced a class of drugs, thiazolidinediones, that increase insulin sensitivity in muscle, fat and the liver. Several studies showed that these drugs lower hemoglobin A1C levels in diabetic patients. One such drug, rosiglitazone, was approved for use in 1999. However, over the ensuing years, several follow-up studies demonstrated a surprising result: Patients on the drug were likely to experience more, not less, heart trouble, with different studies showing increases in heart attacks, heart failure, stroke, and cardiovascular or all-cause mortality (1, 2, 3). Because many of the studies demonstrating positive results of the drug on glucose and hemoglobin A1C levels were not originally designed to examine longer-term cardiovascular results, most follow-up studies were not rigorous trials. Nevertheless, enough concern was raised that, in 2010, the U.S. Food and Drug Administration restricted use of rosiglitazone; in Europe, sales of the drug were suspended.
During their training, clinicians are steeped in the biology of disease, the sequence of steps that leads from subcellular events to disease and its consequences. Thus, it seemed reasonable to assume that an intervention that lowered blood sugar in diabetics would help protect against heart disease. However, although very important to clinical medicine, these biologic mechanisms cannot be substituted for patient outcomes unless there is strong evidence confirming that the two are related. (In fact, the results of studies with several different medications are raising the possibility that, in type 2 diabetes, aggressively lowering levels of blood sugar does not protect against heart disease.) Establishing improved health outcomes in patients is particularly important with new drugs because usually pharmacologic interventions have several clinical effects rather than just one.
THE SCIENTIFIC BASIS FOR CLINICAL MEDICINE
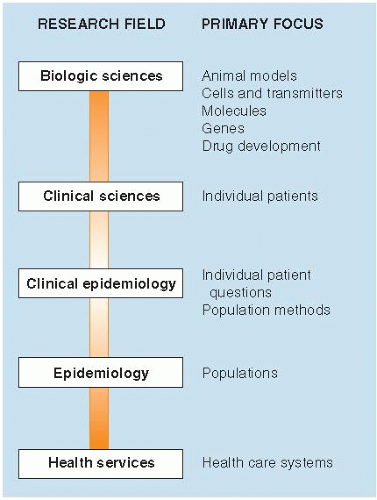
Clinical epidemiology is one of the basic sciences that clinicians rely on in the care of patients. Other health sciences, summarized in Figure 1.1, are also integral to patient care. Many of the sciences overlap with each other.
Clinical epidemiology is the science of making predictions about individual patients by counting clinical events (the 5 Ds) in groups of similar patients and using strong scientific methods to ensure that the predictions are accurate. The purpose of clinical epidemiology is to develop and apply methods of clinical observation that will lead to valid conclusions by avoiding being misled by systematic error and the play of chance. It is an important approach to obtaining the kind of information clinicians need to make good decisions in the care of patients.
Figure 1.1 ▪ The health sciences and their complementary relationships.
The term “clinical epidemiology” is derived from its two parent disciplines: clinical medicine and epidemiology. It is “clinical” because it seeks to answer clinical questions and to guide clinical decision making with the best available evidence. It is “epidemiology” because many of the methods used to answer questions about how to best care for patients have been developed by epidemiologists and because the care of individual patients is seen in the context of the larger population of which the patient is a member.
Clinical sciences provide the questions and approach that can be used to care for individual patients. Some biologic sciences, such as anatomy and physiology, are “clinical” to the extent that they provide sound information to guide clinical decisions. For example, knowing the anatomy of the body helps determine possibilities for diagnosis and treatment of many symptoms.
The population sciences study large groups of people. Epidemiology is the “study of disease occurrence in human populations” (4) by counting health-related events in people in relation to the naturally occurring groups (populations) of which they are members. The results of many such studies are directly applicable to the care of individual patients. For example, epidemiology studies are used as the basis for advice about avoiding behaviors such as smoking and inactivity that place patients at increased risk. Other epidemiologic studies, such as those showing harmful effects of passive smoking and other environmental and occupational hazards, are the basis for public health recommendations. Clinical epidemiology is a subset of the population sciences useful in the care of patients.
Clinicians have long depended on research evidence to some extent, but understanding clinical evidence is more important in modern times than it was in the past for several reasons. An extraordinary amount of information must be sorted through. Diagnostic and therapeutic interventions have the potential for great effectiveness, as well as risk and cost, so the stakes in choosing among them are high. Clinical research at its best has become stronger and, thus, can be a sounder basis for clinical decisions. Nevertheless, the credibility of clinical research continues to vary from study to study, so clinicians need to have a method for sorting out strong from weak evidence.
Evidence-based medicine is a modern term for the application of clinical epidemiology to the care of patients. It includes formulating specific “answerable” clinical questions, finding the best available research evidence bearing on those questions, judging the evidence for its validity, and integrating the critical appraisal with the clinician’s expertise and the patient’s situation and values (5). This book deals with several aspects of evidence-based medicine, especially critically appraising the evidence about clinical questions.
Table 1.3 Factors Other Than Evidence-Based Medicine That May Influence Clinical Decisions
Eminence-based medicine
Senior colleagues who believe experience trumps evidence
Vehemence-based medicine
Substitution of volume and stridency for evidence
Eloquence (or elegance)-based medicine
Sartorial elegance and verbal eloquence
Providence-based medicine
The decision is best left in the hands of the Almighty
Diffidence-based medicine
Too timid to make any medical decision
Nervousness-based medicine
Fear of litigation is a powerful stimulus to overinvestigation and overtreatment
Confidence-based medicine
Bravado
Adapted from Isaacs D, Fitzgerald D. Seven alternatives to evidence-based medicine. BMJ 1999;319:1618.
In real-life clinical settings, other kinds of “evidence” compete for clinicians’ attention and can influence medical decisions. Table 1.3 describes some of them in a parody of evidence-based medicine that was published some years ago, but is still true today. Probably all clinicians have experienced at least one of these factors during their training years! Another factor, not so humorous but very relevant, has been described as level IV evidence (6). Clinicians tend to remember cases when things go terribly wrong in the care they give an individual patient and are more likely to change practice after such an experience than after reading a well-done study. Less valid alternatives to evidence-based medicine can be very compelling at the emotional level and may provide a convenient way of coping with uncertainty, but they are a weak substitute for good research evidence.
Health services research is the study of how non-biologic factors (e.g., clinical workforce and facilities, how care is organized and paid for, and clinicians’ beliefs and patients’ cooperation) affect patients’ health. Such studies have shown, for example, that medical care differs substantially from one small geographic area to another (without corresponding differences in patients’ health); that surgery in hospitals that often perform a specific procedure tends to have better outcomes than hospitals in which the procedure is done infrequently; and that aspirin is underutilized in the treatment of acute myocardial infarction, even though this simple practice has been shown to reduce the number of subsequent vascular events by about 25%. These kinds of studies guide clinicians in their efforts to apply existing knowledge about the best clinical practices.
Other health services sciences also guide patient care. Quantitative decision making includes cost-effectiveness analyses, which describe the financial costs required to achieve a good outcome such as prevention of death or disease and decision analyses, which set out the rational basis for clinical decisions and the consequences of choices. The social sciences describe how the social environment affects health-related behaviors and the use of health services.
Biologic sciences, studies of the sequence of biologic events that lead from health to disease, are a powerful way of knowing how clinical phenomena may play out at the human level. Historically, it was primarily the progress in the biologic sciences that established the scientific approach to clinical medicine, and they continue to play a pivotal role. Anatomy explains nerve entrapment syndromes and their cause, symptoms, and relief. Physiology and biochemistry guide the management of diabetic ketoacidosis. Molecular genetics predicts the occurrence of diseases ranging from common cardiovascular diseases and cancer to rare inborn errors of metabolism, such as phenylketonuria and cystic fibrosis.
However, understanding the biology of disease, by itself, is often not a sound basis for prediction in intact humans. Too many other factors contribute to health and disease. For one thing, mechanisms of disease may be incompletely understood. For example, the notion that blood sugar in diabetic patients is more affected by ingestion of simple sugars (sucrose or table sugar) than by complex sugars such as starch (as in potatoes or pasta) has been dispelled by rigorous studies comparing the effect of these foods on blood glucose. Also, it is becoming clear that the effects of genetic abnormalities may be modified by complex physical and social environments such as diet and exposure to infectious and chemical agents. For example, glucose-6-phosphate dehydrogenase (G6PD) is an enzyme that protects red blood cells against oxidant injury leading to hemolysis. G6DP deficiency is the most common enzyme deficiency in humans, occurring with certain mutations of the X-linked G6PD gene. However, males with commonly occurring genetic variants of G6PD deficiency are usually asymptomatic, developing hemolysis and jaundice only when they are exposed to environmental oxidant stresses such as certain drugs or infections. Finally, as shown in the example of rosiglitazone treatment for patients with type 2 diabetes, drugs often have multiple effects on patient health beyond the one predicted by studying disease biology. Therefore, knowledge of the biology of disease produces hypotheses, often very good ones, about what might happen in patients. But these hypotheses need to be tested by strong studies of intact human beings before they are accepted as clinical facts.
Only gold members can continue reading. Log In or Register to continue