Highlights
- •
Stimulated Raman histology can be interpreted by humans and artificial intelligence.
- •
Stimulated Raman histology can provide procedural tumoral mapping during cryosurgical ablation of prostate cancer.
- •
Stimulated Raman histology can identify prostate cancer in a prostate biopsy in approximately 1 minute.
- •
Identification of clinically significant prostate cancer radial to a MRI predicted margin during cryosurgical ablation is at high risk for recurrence.
Abstract
Background
In-field or in-margin recurrence after partial gland cryosurgical ablation (PGCA) of prostate cancer (PCa) remains a limitation of the paradigm. Stimulated Raman histology (SRH) is a novel microscopic technique allowing real time, label-free, high-resolution microscopic images of unprocessed, un-sectioned tissue which can be interpreted by humans or artificial intelligence (AI). We evaluated surgical team and AI interpretation of SRH for real-time pathologic feedback in the planning and treatment of PCa with PGCA.
Methods
About 12 participants underwent prostate mapping biopsies during PGCA of their PCa between January and June 2022. Prostate biopsies were immediately scanned in a SRH microscope at 20 microns depth using 2 Raman shifts to create SRH images which were interpreted by the surgical team intraoperatively to guide PGCA, and retrospectively assessed by AI. The cores were then processed, hematoxylin and eosin stained as per normal pathologic protocols and used for ground truth pathologic assessment.
Results
Surgical team interpretation of SRH intraoperatively revealed 98.1% accuracy, 100% sensitivity, 97.3% specificity for identification of PCa, while AI showed a 97.9% accuracy, 100% sensitivity and 97.5% specificity for identification of clinically significant PCa. 3 participants’ PGCA treatments were modified after SRH visualized PCa adjacent to an expected MRI predicted tumor margin or at an untreated cryosurgical margin.
Conclusion
SRH allows for accurate rapid identification of PCa in PB by a surgical team interpretation or AI. PCa tumor mapping and margin assessment during PGCA appears to be feasible and accurate. Further studies evaluating impact on clinical outcomes are warranted.
1
Introduction
Partial gland cryosurgical ablation (PGCA) of prostate cancer (PCa) is an operative technique which balances oncologic and function outcomes. Confluent destruction of the target volume is a primary oncologic goal of PGCA. Reported In-field recurrence rates are range from 7.5 to 35% and likely represent undertreatment of the target volume, either through nonconfluent ablation or treatment margin failures [ , ]. Treatment margin failure can occur for a variety of reasons including poor localization of tumor, underestimation of tumor volume on imaging and inadequate size of ablation [ , ]. Techniques to ensure complete confluent destruction of the target volume that may reduce in field recurrence are critical to the success of PCa PGCA.
We postulated that intraoperative prostate mapping biopsies may represent 1 method to improve localization of PCa and assess treatment margins during PGCA. Techniques enabling rapid assessment of prostate biopsy (PB) pathology in the therapeutic setting are time and resource intensive, limiting routine implementation. While frozen section analysis offers the potential for real-time evaluation of tissues, the efficiency of such an approach is highly variable, with centers reporting substantive delays of up to 30 to 40 minutes for frozen section analysis [ ].
A clinical microscope using stimulated Raman spectroscopy has been used to create high-resolution, real-time images of unprocessed, unlabelled, fresh tissue; the images produced by the microscope are referred to as stimulated Raman histology (SRH) [ ]. The SRH microscope creates images, which with a pseudo-coloring appear similar to conventional hematoxylin and eosin (H&E) staining [ , ]. Initial validation of SRH to prostate biopsies revealed an accuracy for PCa identification 96.9% for pathologists [ ] and 96.5% for artificial intelligence (AI) [ ].
The procedural application of SRH to PGCA promises to provide a method for rapid lesion localization, mapping, and margin assessment. This study sought to determine if use of intraoperative biopsies visualized with SRH could provide near real-time pathologic feedback to guide PGCA treatment. We hypothesized that SRH could provide histologic images of diagnostic quality, and that such images could be interpreted by a surgical team or AI during PGCA.
2
Materials and methods
2.1
Participants selection
Utilizing this FDA-approved device, patients undergoing PGCA between January and June 2022 were offered intraprocedural prostate mapping biopsies at time of surgical consent. Twelve participants were consecutively recruited based on availability of the microscope undergoing PGCA by 1 of 2 faculty urologists. Participants were excluded if they received preoperative androgen deprivation therapy.
2.2
Magnetic resonance imaging and magnetic resonance imaging-ultrasound fusion targeted biopsy
As previously described, all MRI were performed with a 3T MRI device with an external phased array coil [ ]. Regions of interest were identified on MRI and scored as per PI-RADSv2 [ ]. MRI to ultrasound fusion targeted biopsy was performed with the Artemis TM prostate biopsy system utilizing the Profuse TM co-registration software (Eigen, Grass Valley, California) for segmentation and MRI to ultrasound co-registration of potential regions [ ]. All participants underwent targeted and systematic biopsies (4 targeted prostate biopsies taken from the region(s) of interest, in addition to 12 systemic) [ ].
2.3
Partial gland cryosurgical ablation with prostate mapping biopsy technique
All PGCA were performed under general anesthesia in the dorsal lithotomy position. Disease specific treatment plans were designed based upon cognitive or visual estimation of the location of previously segmented regions of interest demonstrating cancer on targeted biopsy. An intended treatment zone was contoured to achieve at least a 10mm intraprostatic margin beyond the tumor segmentation (limited to 3mm beyond any adjacent prostate capsule), while incorporating the location of adjacent systematic cancer-bearing cores [ ]. Between 2 and 4 cryosurgical probes were initially placed under ultrasound guidance. Temperature sensing probes were placed within the freeze zone, at its planned margin and within surrounding critical structures to be preserved. Additionally, a urethral warming catheter was placed over a guidewire for urethral protection during treatment. Two freeze/thaw cycles were carried out for each treatment utilizing the Cryocare CS TM system (Endocare, Austin, TX).
Prior to freezing a PB was obtained from the site of anticipated tumor and 2 cores were taken from adjacent 10mm treatment margins based upon MRI predicted tumor volume. During the freeze, biopsy samples were obtained from 3 to 5mm beyond the ice ball. Biopsies were immediately scanned in a SRH microscope which were interpreted by the surgical team intraoperatively. Interpretation of SRH was conducted by M.P.M. and S.S.T. whom have significant experience in the prostate SRH including the development of technique and physician training which included review of over 1000 PCa SRH histologic images [ , ]. Initial experience with physician testing and training for prostate SRH interpretation has been previously described by Mannas et al.[ ] If intraoperative margins returned positive, the freezing was widened to include the positive margin during the second freeze/thaw cycle at the operator’s discretion.
2.4
Creation and interpretation of stimulated Raman histology
Samples were placed in normal saline solution to remain fresh, unstained, and unlabelled prior to scanning in the NIO, a FDA approved stimulated Raman histology microscope (NIO, Invenio Imaging, Santa Clara, CA). As previously described by Mannas et al., PB were placed into a modified, linear NIO slide that compress the samples to a thickness of 225um. Images of 18×1.5mm were then acquired by means of strip-tiling at a fixed imaging depth from the sample surface to create digital image by scanning PBs at a depth of 20 microns using 2 Raman shifts: 2845cm −1 and 2930cm −1 [ ]. SRH was created by applying pseudo-coloring to the raw images, as described by Orringer et al, in order to generate a digital image that mimics the appearance of H&E staining [ ]. The SRH microscope produces images during SRH creation which allows for interpretation of the images before completion of scanning. Time to PCa diagnosis and total scan time for each biopsy was recorded. Once the process of creating SRH was completed the PBs were placed into 10% formalin to be processed as per normal pathologic protocols and interpreted by a genitourinary pathologist, utilizing H&E and if necessary, immunohistochemistry.
2.5
Convolutional neural network
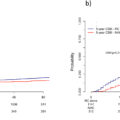
Due to the time limitation for intraoperative creation and interpretation of SRH we retrospectively sought to assess if this could be improved by utilizing our previously assessed AI convolutional neural network (CNN) at regular and increased scanning speeds [ ]. Briefly, for the classification of a PB we aggregated the score of all SRH images of that PB by looking at the maximum tumor overall prediction. The previously tested CNN threshold >89% maximum tumor overall prediction for PB malignant classification was utilized as per Mannas et al., otherwise the PB was classified as benign [ ].
2.6
Statistical analysis
All statistical analysis was conducted with SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). The sensitivity, specificity, and accuracy of the surgical team and AI interpretation of SRH were compared to the final pathologic result determined by pathologist interpretation of H&E staining with immunohistochemistry, if required. Fisher’s exact test was used to compare accuracy for PCa identification between human and AI interpretation. Atypical small acinar proliferation was excluded from the analysis, as the diagnosis is benign, however, glands may represent a small focus of malignancy.
3
Results
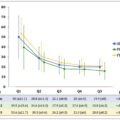
About 12 consecutive men with intermediate risk PCa met inclusion criteria and underwent prostate mapping biopsies with real-time procedural SRH interpreted by the surgical team. The mean PB SRH scan time was 5.8 minutes and mean time to PCa diagnosis was only 3.4 minutes. A total of 69 prostate mapping biopsies were obtained, with a median number of 5 per participant; 7 biopsies containing atypical small acinar proliferation were excluded. The surgical team showed an accuracy of 98.2%, sensitivity 100% and specificity 97.4% for identification of PCa, Table 2 . One biopsy containing benign adenosis was classified as PCa intraoperatively; however, H&E was insufficient to render a diagnosis and immunohistochemistry was required to rule out malignancy. PCa was identified at a 10mm planned margin from the estimated tumor segmentation in 6 biopsies, from 5 participants and PCa was identified beyond the first cycle ice ball in 2 biopsies from 2 participants, Table 1 .
Related posts:
 A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
 Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
 Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
 The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
 Testosterone recovery after androgen deprivation therapy
Testosterone recovery after androgen deprivation therapy
 Testicular cancer malpractice trends
Testicular cancer malpractice trends
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


