arranged around the periphery. When epithelial bridges are present, they appear stretched or twisted and commonly show central attenuation. Micropapillary projections, if present, are typically tuft-like or elongated and tapering, resembling the pattern of hyperplasia seen in gynecomastia. The cells comprising UDH are cytologically benign; vary in size, shape, and orientation; are arranged in a haphazard pattern; and have poorly defined borders that may result in a syncytial appearance. The cells do not polarize around lumens within the proliferation. In some instances, there is prominent streaming or swirling of the cells. The nuclei vary in size, shape, and contour and may show overlapping. Nuclear grooves and intranuclear cytoplasmic inclusions may be evident. These architectural and cytologic features of UDH are illustrated in Figs. 3.1, 3.2, 3.3, 3.4, 3.5, 3.6, 3.7, 3.8 and 3.9 and e-Figs. 3.1, 3.2, 3.3, 3.4, 3.5, 3.6, 3.7 and 3.8. Multiple cell types (including metaplastic cells with apocrine or, less often, squamous features) may be present (Figs. 3.10 and 3.11, e-Figs. 3.9 and 3.10). Foamy histiocytes (Fig. 3.12), as well as calcifications (Fig. 3.13), may be seen in association with the proliferating epithelial cells. Rarely, foci of necrosis are present (Fig. 3.14, e-Fig. 3.11). Alterations in the surrounding stroma, such as fibroblastic proliferation, elastosis, and mononuclear cell infiltrates, are uncommon. The key features of UDH are summarized in Table 3.1.
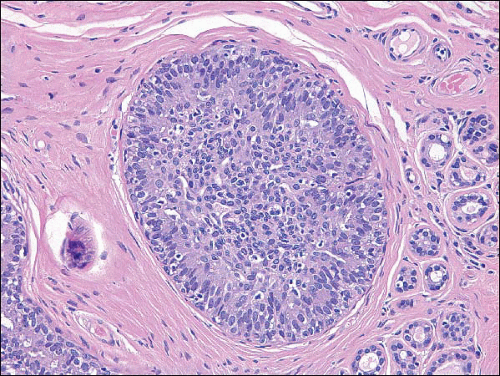 FIGURE 3.1 Usual ductal hyperplasia. There is a solid proliferation of cells filling the space. The cells and nuclei vary in size, shape, and orientation. |
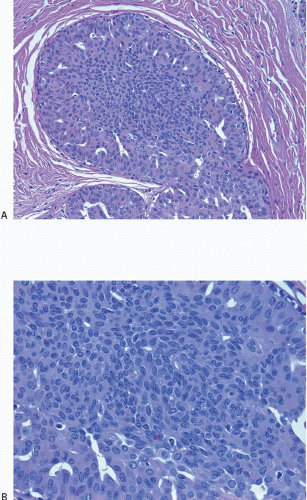 FIGURE 3.2 Usual ductal hyperplasia. A: The few fenestrations present in this mostly solid proliferation are slit-like and irregular in shape and present primarily toward the periphery. B: Higher power view illustrates heterogeneity in cell size, shape, and placement, as well as poorly defined cell borders. |
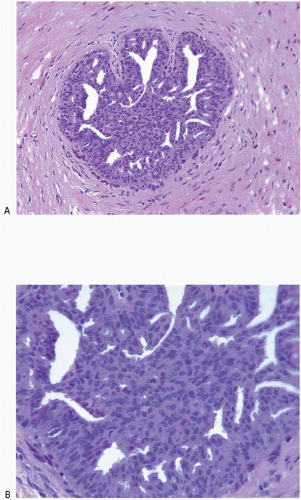 FIGURE 3.3 Usual ductal hyperplasia. A: Fenestrations in this proliferation vary in size and shape. B: Higher power view demonstrates haphazard arrangement of cells, with no regular orientation around the fenestrations. |
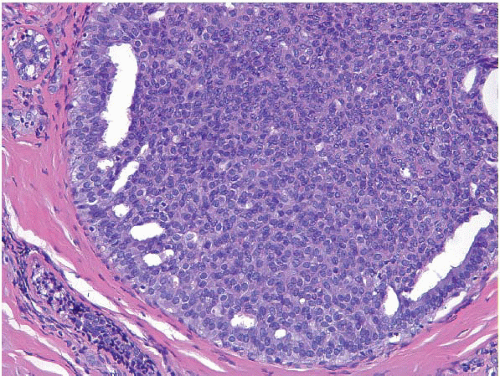 FIGURE 3.4 Usual ductal hyperplasia. Solid proliferation of cells with poorly defined cell borders and peripheral fenestrations. |
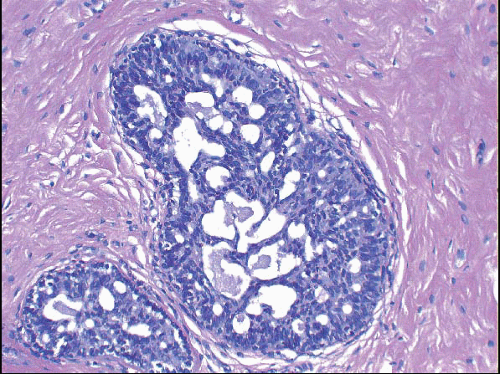 FIGURE 3.5 Usual ductal hyperplasia. The cellular bridges that traverse the lumen appear stretched and thinned. Nuclei in these bridges are compressed, stretched, and oriented in the same direction as the bridges. |
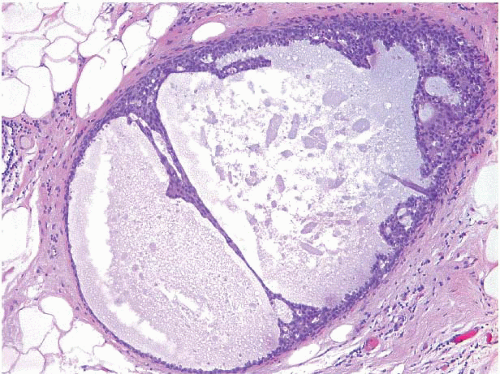 FIGURE 3.6 Usual ductal hyperplasia. The bridge traversing the lumen shows extreme attenuation. |
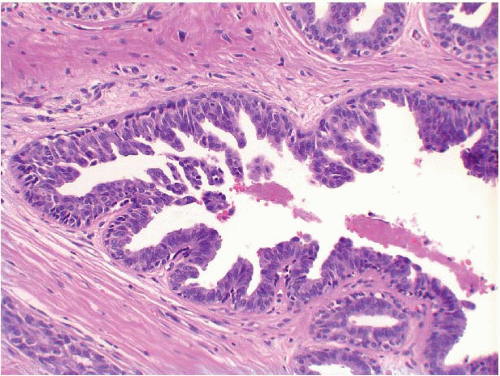 FIGURE 3.7 Usual ductal hyperplasia with micropapillary (gynecomastoid) features. Micropapillary fronds, many of which taper toward their tips, project into the lumen. This appearance is similar to that seen in gynecomastia. |
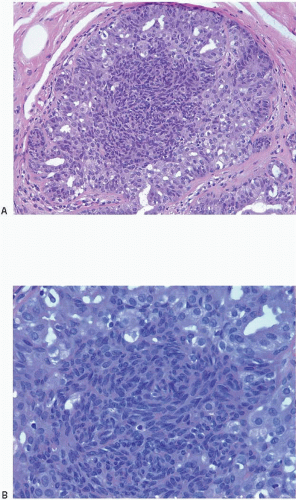 FIGURE 3.8 Usual ductal hyperplasia. A: Prominent cellular swirling is seen in the center of this proliferation. B: Higher power view illustrates cellular swirls with overlapping nuclei. |
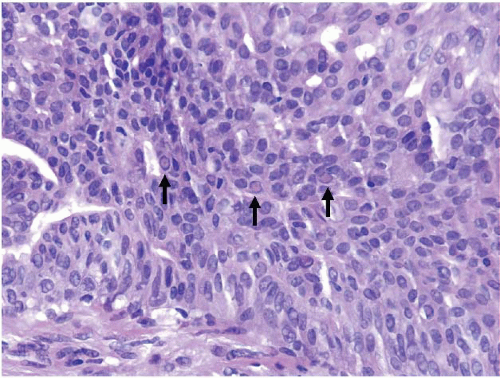 FIGURE 3.9 Usual ductal hyperplasia with several intranuclear cytoplasmic inclusions (arrows). |
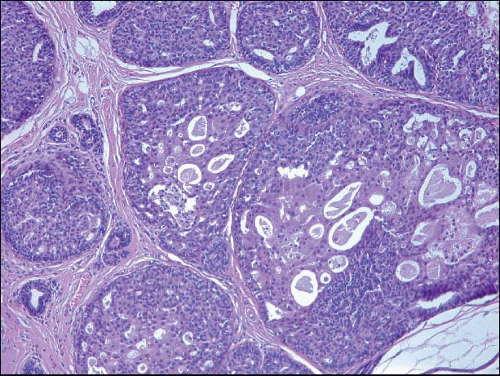 FIGURE 3.10 Usual ductal hyperplasia with foci of apocrine metaplasia. |
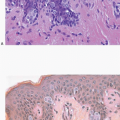
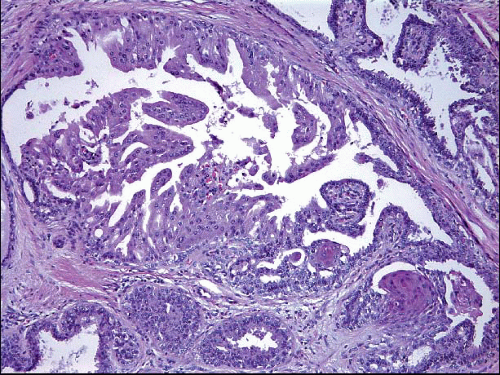 FIGURE 3.11 Usual ductal hyperplasia with apocrine metaplasia (upper left) and squamous metaplasia (lower right). |
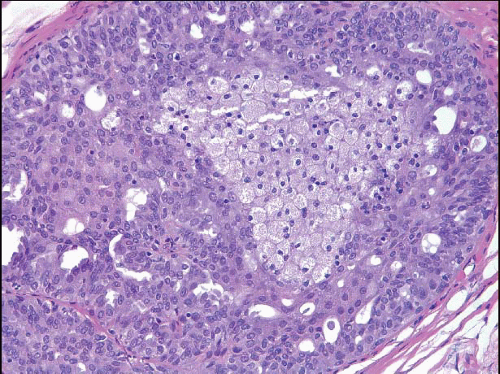 FIGURE 3.12 Usual ductal hyperplasia with foamy histiocytes. |
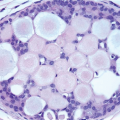
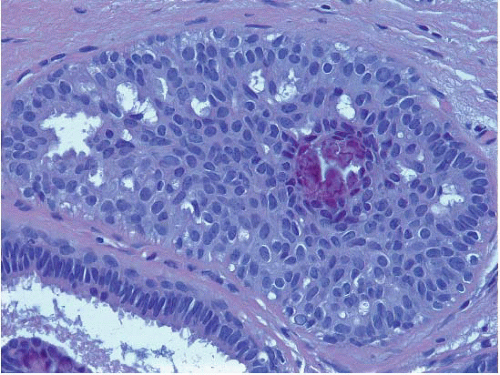 FIGURE 3.13 Usual ductal hyperplasia with calcification. |
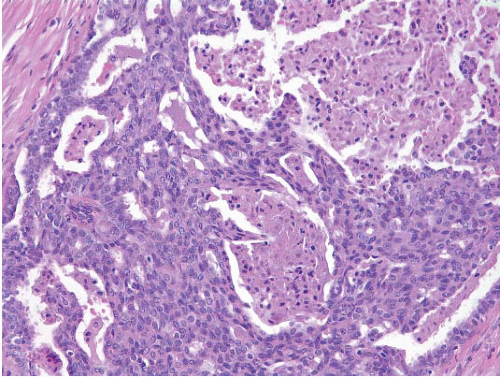 FIGURE 3.14 Usual ductal hyperplasia (UDH) with necrosis. This cellular proliferation with features characteristic of UDH also exhibits foci of necrosis. Although uncommon, the presence of necrosis does not preclude a diagnosis of UDH if the architectural and cytologic features of the proliferation support that diagnosis. |
TABLE 3.1 Key Features of Usual Ductal Hyperplasia | ||
|---|---|---|
|
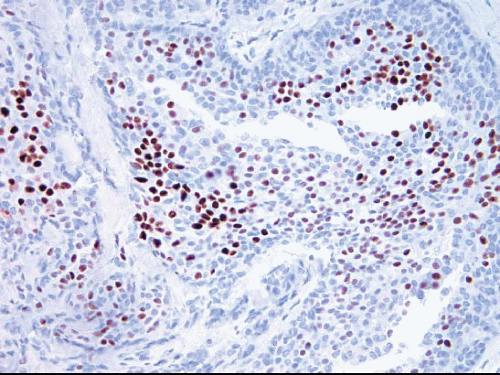 FIGURE 3.15 Usual ductal hyperplasia immunostained for estrogen receptor (ER). There is heterogeneity of nuclear ER expression in the cells comprising this lesion. Some cells are strongly positive, others are more weakly positive, and others are negative. |
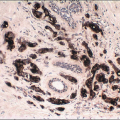
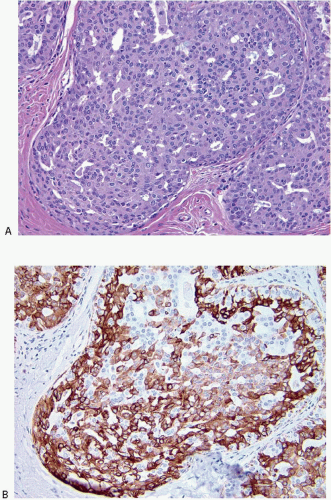 FIGURE 3.16 Usual ductal hyperplasia (UDH). A: H&E-stained section. B: Immunostain for CK5/6 illustrates the mosaic pattern of staining characteristic of UDH. |
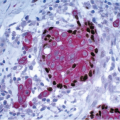
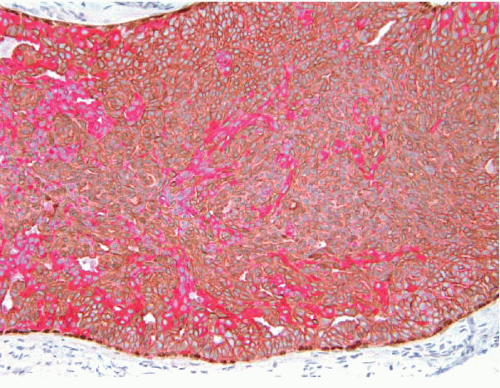 FIGURE 3.17 Usual ductal hyperplasia immunostained with a cocktail of antibodies to low-molecular-weight (luminal) cytokeratins CK7/18 (red cytoplasmic staining), high-molecular-weight (basal) cytokeratins CK5/14 (brown cytoplasmic staining), and p63 (brown nuclear staining). The proliferation is composed of a mixture of cells with luminal and basal phenotypes. p63-positive myoepithelial cells are confined to the periphery of the involved space. |
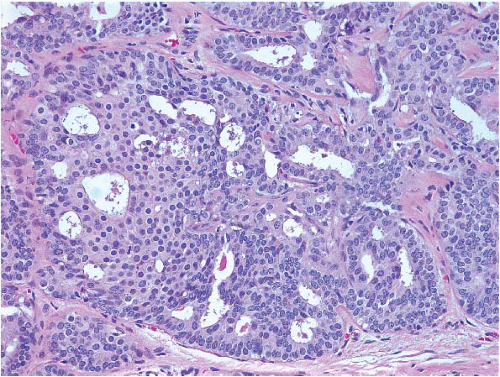 FIGURE 3.18 Atypical ductal hyperplasia. A portion of this space (left) contains a proliferation of monotonous cells with uniform, round, evenly spaced nuclei reminiscent of those seen in low-grade ductal carcinoma in situ. The cellular proliferation in the remainder of the space has features more characteristic of usual ductal hyperplasia. |
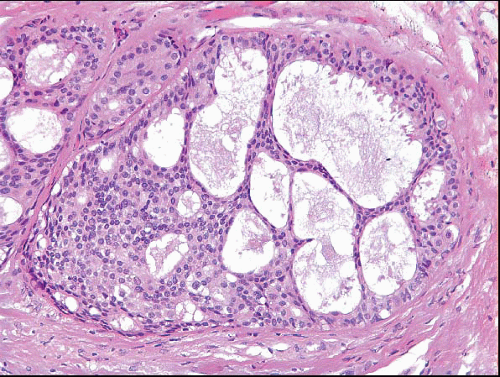 FIGURE 3.19 Atypical ductal hyperplasia (ADH). The proliferation on the left side of this space has features of low-grade ductal carcinoma in situ, characterized by a uniform cell population and punched-out spaces. However, the attenuated cellular bridges on the right are characteristic of those seen in usual ductal hyperplasia. Therefore, a diagnosis of ADH is appropriate. |
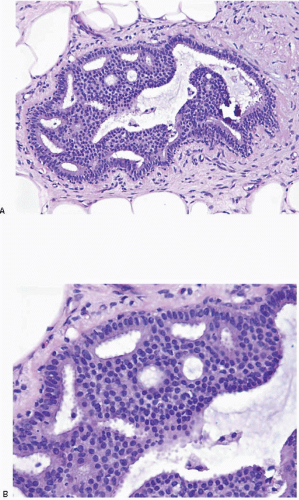 FIGURE 3.20 Atypical ductal hyperplasia. A: The uniform, atypical cell population involves only a portion of the space. B: High-power view of the atypical cell population demonstrating relatively evenly placed cells with uniform nuclei that focally polarize around extracellular lumina. |
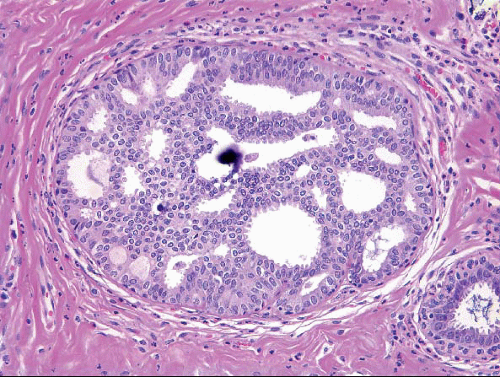 FIGURE 3.21 Atypical ductal hyperplasia with calcification. |
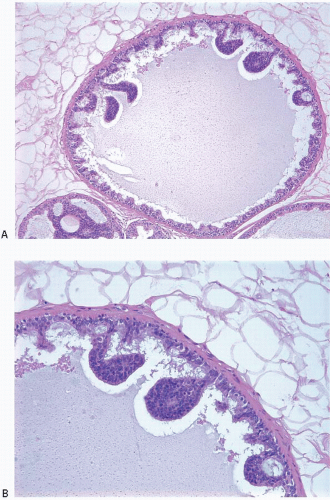 FIGURE 3.22 Atypical ductal hyperplasia with micropapillary features. A: Low-power view demonstrates a few club-shaped micropapillae protruding into the duct lumen. Only a portion of the space is involved. B: High-power view illustrates uniformity of the cell population within the micropapillae. |
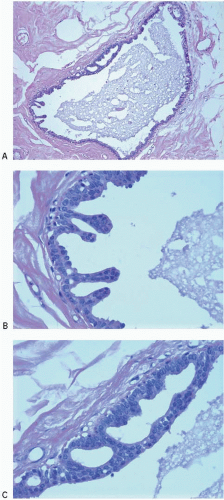 FIGURE 3.23 Atypical ductal hyperplasia. A: This duct contains a few bulbous micropapillations and a rigid arcade. High-power views of micropapillae (B) and cellular arcade (C) illustrate a monotonous cell population. The nuclei in the arcade are relatively round and evenly spaced. |
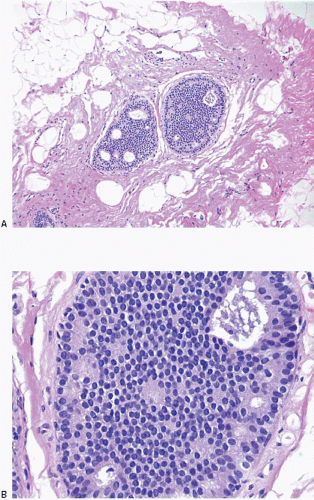 FIGURE 3.24 Atypical ductal hyperplasia vs. low-grade ductal carcinoma in situ (DCIS) seen at scanning magnification (A) and at high power (B). This lesion consists of a cribriform epithelial proliferation composed of a uniform population of cells with small, monomorphic nuclei. It is limited to two spaces and is less than 2 mm in size. Therefore, it could be categorized as either low-grade DCIS using the original Page criteria6 or atypical ductal hyperplasia using the Tavassoli and Norris criteria7. In current practice, most pathologists would fall short of categorizing a low-grade lesion of such limited extent as DCIS. |
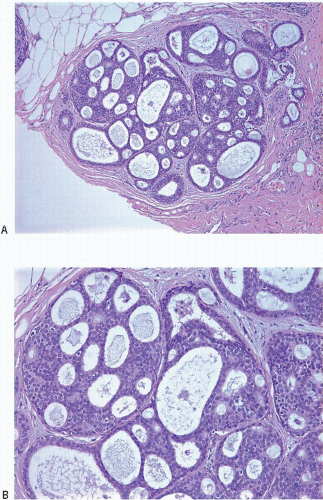 FIGURE 3.25 Severely atypical intraductal proliferation in a terminal duct lobular unit at low (A) and medium power (B). The qualitative features of this lesion approach those of low-grade ductal carcinoma in situ, but the lesion is limited in extent (see text). |
TABLE 3.2 Key Features of Atypical Ductal Hyperplasia | |||
|---|---|---|---|
|
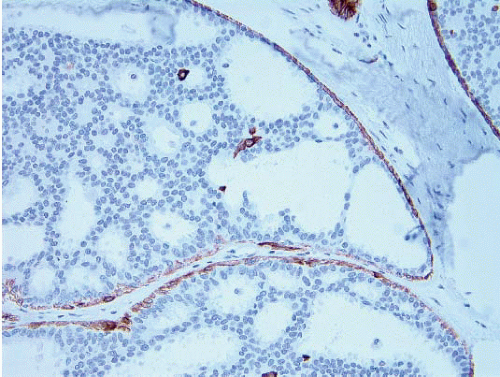 FIGURE 3.26 Atypical ductal hyperplasia, CK5/6 immunostain. The neoplastic cells comprising this proliferation are CK5/6 negative (surrounding myoepithelial cells show staining for CK5/6). |
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


