patient and HCP safety surveillance systems. Standardized definitions are provided by the CDC, and data are collected and reported actively by infection preventionists. The CDC publishes the data as standardized infection ratios (SIRs) annually. NHSN provides infection rates or ratios with some risk adjustment primarily for device-associated infections and SSIs. Reporting into a national database allows acute care hospitals to benchmark their data to other hospitals, provides information on the scope of healthcareassociated pathogens, and provides data on the frequency and antimicrobial susceptibility of pathogens.
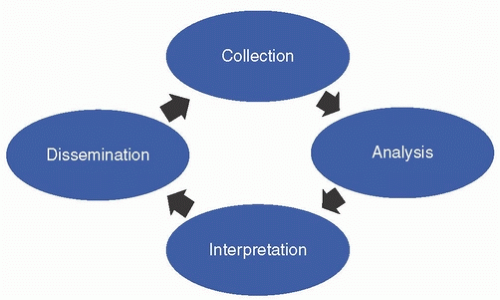 FIGURE 2-1 Ongoing, systematic steps of surveillance. |
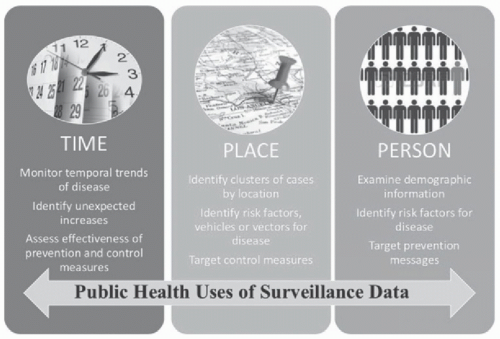 FIGURE 2-2 Uses of surveillance data. |
to visualize time trends. By assessing the geographic locations where diseases occur, epidemiologists can identify clusters of cases by location; identify risk factors, vehicles, or vectors for diseases; and target control measures to specific locations. Geographic information system mapping can aid in analysis and interpretation by place. Collecting surveillance data that allows for assessment of the types of persons affected by the disease can be important for identifying risk factors for disease and targeting prevention messages.
TABLE 2-1 Types of Surveillance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
or suspected to be high (eg, influenza); or additional epidemiologic, clinical, or laboratory data are desired (eg, CDC’s Active Bacterial Core surveillance system). For example, before carbapenem-resistant Enterobacteriaceae was added by the U.S. Council of State and Territorial Epidemiologists to the list of reportable public health diseases, several large hospitals were selected to perform laboratory-based surveillance.11 For different types of HAI surveillance, facilities should consider the scope or breadth of their surveillance activities (ie, will surveillance occur equally across the entire facility or be focused in targeted locations). In addition, facilities should consider which approach (ie, patient-based, laboratory-based) will be used for detection of HAI cases. While some smaller facilities can examine individual patient’s medical records to assess for signs/symptoms of infections, other facilities may use reports based on positive microbiological findings to investigate patients’ records for identification of HAIs.
Related posts:
 Legal Issues in Healthcare Epidemiology and Infection Prevention
Healthcare-Associated Bloodstream Infections (Non-device related)
MDRO Infections: Gram-Negative Organisms
Healthcare-Associated Infections in Obstetric Patients
Infection Prevention and Control in Resource-Limited Settings
Exposures to Contagious Infectious Diseases
Legal Issues in Healthcare Epidemiology and Infection Prevention
Healthcare-Associated Bloodstream Infections (Non-device related)
MDRO Infections: Gram-Negative Organisms
Healthcare-Associated Infections in Obstetric Patients
Infection Prevention and Control in Resource-Limited Settings
Exposures to Contagious Infectious Diseases
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


