Fig. 9.1
High nuclear grade DCIS in a 47 year old found on screening mammography. (a) CC spot magnification view demonstrates segmental pleomorphic calcifications (b) MRI performed for extent of disease, maximum intensity projection (MIP) images demonstrates regional nonmass enhancement with a clumped internal enhancement pattern in the inner right breast
In the second edition of BI-RADS for MR, the internal enhancement pattern “clustered ring” has been added. This is defined as small rings of enhancement, which are clustered together (Figs. 9.2 and 9.3) [39]. A study by Tozaki et al. showed that this finding was seen in 63 % of cases of malignancy (including both invasive and non-invasive), versus only 4 % of benign cases. The specificity for malignancy of the finding of clustered ring enhancement was 96 % [40].
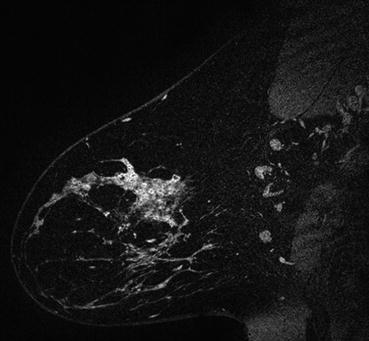
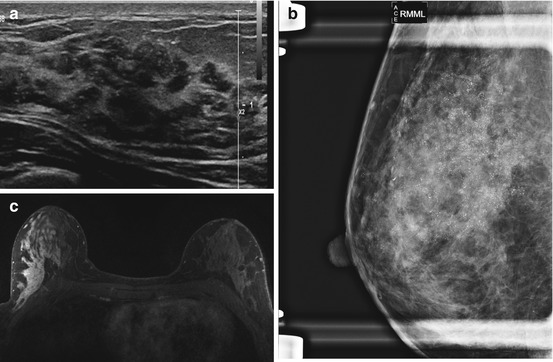
Fig. 9.2
Sagittal post-contrast subtracted image demonstrates segmental NME with a clustered ring internal enhancement pattern, compatible with biopsy proven DCIS in a 38 year old
Fig. 9.3
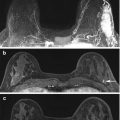
28-year-old female with a palpable lump in the right breast. Given the patient’s age she had an ultrasound examination to start. (a) Ultrasound images show an irregular mass containing multiple echogenic foci (b) Subsequently performed CC mammogram demonstrates fine pleomorphic calcifications. (c) MRI performed for extent of disease demonstrates regional NME with a clustered ring internal enhancement pattern, consistent with biopsy proven DCIS
When DCIS presents as NME, the most common distribution pattern is a segmental distribution, seen in approximately 14–77 % of cases [36–38, 41]. This is defined as a triangular region of enhancement, apex pointing to the nipple, suggesting a duct or its branches (Fig. 9.4) [39]. It may also present less commonly in a linear, focal, regional, or diffuse enhancement pattern [36–38, 41]. The MR BI-RADS 2nd edition has removed the distribution ductal from the lexicon [39].
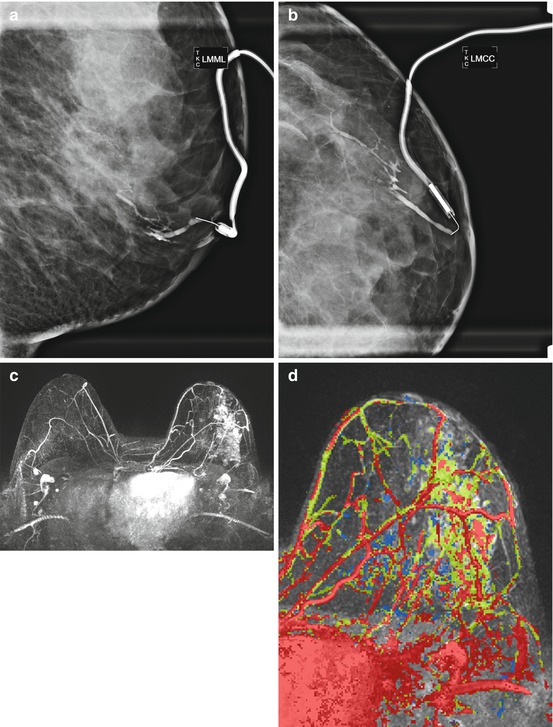
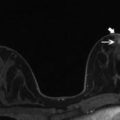
Fig. 9.4
34 year old with left bloody nipple discharge, normal mammogram and ultrasound. (a) LM and (b) CC views from a ductogram show an intraductal-filling defect in a slightly lower, slightly outer duct. Left duct surgical excision revealed IDC and DCIS on pathology. (c) MRI post-contrast subtracted MIP demonstrated extensive clumped NME with a segmental distribution (d) Kinetic image demonstrates mixed, predominantly Type 2 and Type 3 delayed kinetics. MR guided biopsy revealed DCIS and IDC. Kinetic key: Type 1 = blue, Type 2 = green, Type 3 = red
DCIS may also present as a mass morphology on MRI. A mass is defined as a 3D space occupying structure with convex outward contour, which may or may not displace or otherwise affect the surrounding normal breast tissue [39]. This morphology has been seen in approximately 14–41 % of cases of DCIS on MRI [36–38]. Masses are further defined by shape, margin, and internal enhancement patterns. When DCIS presents as a mass on MRI it most commonly is an irregular mass, seen in 14–83 % of cases (Fig. 9.5). Less frequently it may present as an oval or round mass [36, 37, 42]. Of note, the 2nd edition of the MR BI-RADS lexicon has removed the shape lobular for mass lesions to be consistent with the mammogram and ultrasound sections. Masses with up to 3 lobulations now simply are described as “oval” [39]. The literature describes various mass margins when DCIS presents as a mass on MRI, including irregular (14–92 % of cases) and spiculated (0–92 % of cases) (Fig. 9.5). Infrequently DCIS presenting as a mass may have smooth margins (4–8 % cases) [36, 37, 42]. DCIS manifesting as a mass on MRI, may have various internal enhancement patterns. The most common pattern is heterogeneous (9–67 %), followed by homogenous (9–25 %), and less commonly rim enhancement (0–8 %) (Fig. 9.6) [36, 37]. To our knowledge, there has not been a report of non-enhancing dark internal septa in reports of DCIS seen as a mass on MRI. Of note, the terms central enhancement and enhancing septations have been removed from the new BI-RADS lexicon [39].
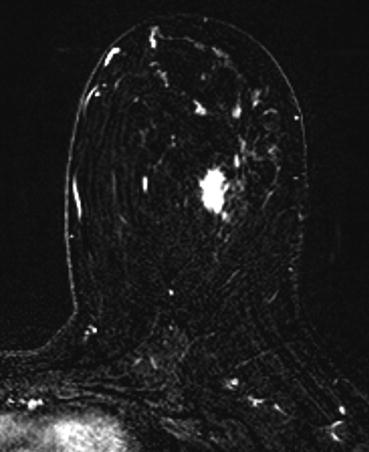
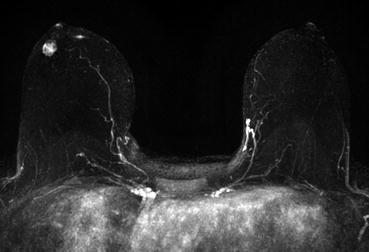
Fig. 9.5
Micropapillary DCIS in a 38-year-old woman with a palpable lump in the left breast. Post-contrast subtracted MR image shows an irregular mass, with spiculated margins, consistent with biopsy proven micropapillary DCIS
Fig. 9.6
High grade DCIS in a 38 year old female with new diagnosis of DCIS. Post-contrast MIP image demonstrates an oval mass with irregular margins and a heterogeneous internal enhancement pattern in the slightly outer right breast
The least common morphologic appearance of DCIS is a focus [36–38]. A focus is defined as a lesion <5 mm, which is too small to further characterize (Fig. 9.7) [39]. The new BI-RADS edition has removed the term foci from the lexicon [39]. Rosen et al. found that pure DCIS manifests as a focus in 12.5 % of cases while 3.0 % of invasive carcinomas manifest as a focus [38]. Van Goethem et al. found that a focus was seen in 20 % of DCIS cases versus 2.8 % invasive cancers [44]. Factors suggesting that a focus is malignant on MRI include: no T2 hyperintensity, lack of fatty hilum, washout kinetics, new or enlarging in size. Signs of benignity of a focus include: T2 hyperintensity, presence of a fatty hilum, persistent kinetics, and stability [39].
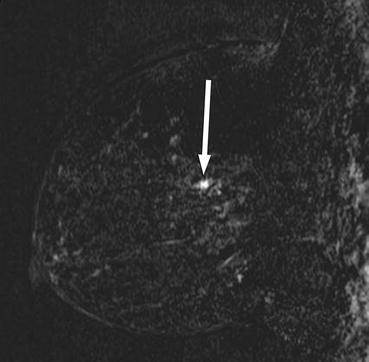
Fig. 9.7
Intermediate-grade DCIS in a 44 year old woman with negative mammographic findings who underwent screening MR imaging because of a strong family history of premenopausal breast cancer. Sagittal postcontrast subtraction image demonstrates a 4 mm focus that demonstrated type 3 (washout) kinetics (Reprinted with permission from Greenwood et al. [43], with permission from Radiology Society of North America (RSNA®))
Jansen et al. found that there was no statistically significant difference between MR morphology in low, intermediate, and high nuclear grade DCIS lesions [36]. Additional studies by Chan et al., and Rahbar et al., also found no significant difference in MR morphology between high grade and non-high grade DCIS [37, 45]. At this point, no study to our knowledge has shown that MR morphology is able to predict nuclear grade of DCIS.
9.3.2 Kinetics
The kinetic pattern of DCIS varies widely. The initial enhancement phase is defined as occurring within the first 2 minutes after contrast injection or until peak enhancement is reached [39]. In the initial phase, the most common kinetic pattern for DCIS is a fast uptake, seen in 49–68 % of cases, less commonly an intermediate (<20 % of cases) or slow pattern (<20 % of cases) [36, 38, 46]. Of note, in the new BI-RADS 5th edition the term fast has replaced rapid [39]. The delayed enhancement phase is defined as following 2 minutes after contrast injection or after peak enhancement is reached and is used to described the shape of the curve [39]. There is a wide variety of delayed phase kinetic patterns seen in DCIS. The most common pattern is a plateau (type 2), seen in 20–52 % of cases (Fig. 9.8) followed by a washout pattern (type 3), in 28–44 % of cases, and persistent enhancement pattern is seen in 20–30 % of cases [36, 38, 46]. Given the significant variation in the kinetic patterns of DCIS, it is very important to base the assessment for DCIS on MRI primarily on morphology rather than kinetics.
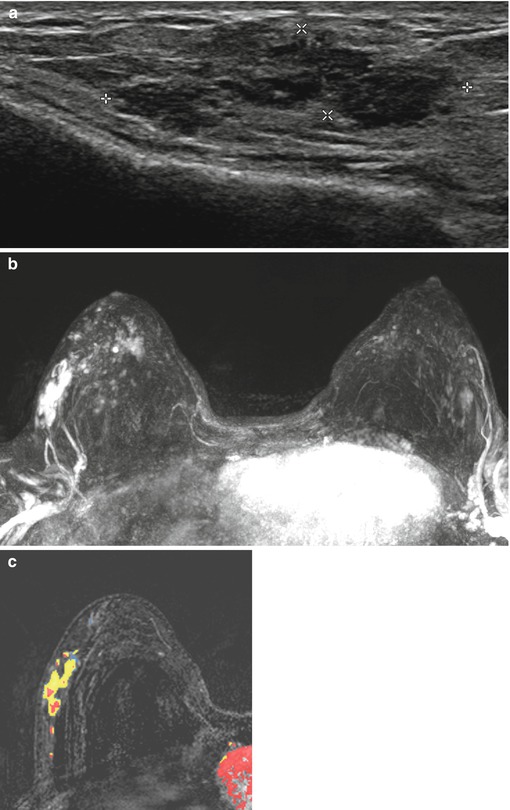
Fig. 9.8
High grade DCIS in a 56-year-old woman with a palpable lump (a) Ultrasound image demonstrates a hypoechoic mass with indistinct margins and echogenic foci, corresponding to calcifications on mammography. (b) MRI performed for extent of disease demonstrates corresponding segmental clumped NME (c) with predominantly Type 2 (plateau) delayed kinetic pattern, compatible with biopsy proven high grade DCIS (Kinetic key: Blue = type 1, yellow = type 2, red = type 3)
Additional studies have looked at whether kinetic patterns may predict grade of DCIS. Jansen et al. found no significant difference in kinetic patterns, both initial and delayed, and grade of DCIS [36]. A study in 2012 by Rahbar et al. found no significant association between nuclear grade and delayed phase of enhancement. They did find a non-significant trend (p = .05) towards higher peak initial enhancement in high-grade DCIS lesions, compared to non-high grade, at 1.5 T [47]. However, a subsequent study by Rahbar et al. in 2015, found no statistically significant difference in kinetic patterns, initial and delayed, of various grades of DCIS when done at 3 T MR imaging [45].
9.3.3 1.5 T Versus 3 T
There has been increasing use of 3 T MRI for clinical dynamic contrast enhanced breast imaging over the last decade. As it has become apparent that high spatial resolution allows for more accurate detection of DCIS, it follows that 3 T MRI may have increased sensitivity for DCIS, as a benefit of 3 T imaging is higher signal to noise ratio, which allows for higher spatial resolution [48]. Rahbar et al. did a prospective study in patients newly diagnosed with pure DCIS. Each patient underwent a pre-operative breast MRI at both 1.5 T and 3 T imaging. They found that maximum DCIS lesion size on 3 T had a higher correlation with maximum size found on pathology than did 1.5 T [49]. 3 T may therefore be clinically helpful in pre-operative planning for DCIS lesions and further research in this area may be of clinical significance.
9.4 Diffusion Weighted Imaging
As discussed earlier, DCIS has a variable morphologic and kinetic presentation at MRI, which may present diagnostic challenges. No statistically significant difference in morphology has been shown to predict high grade versus non-high grade DCIS [36, 37, 45]. As the concerns for overdiagnosis and overtreatment grow, this becomes a challenge. In addition, another challenge is that breast MRI requires gadolinium administration with may limit accessibility. Diffusion weighted imaging (DWI) is a valuable MRI technique that may better be able to predict grade of DCIS and in addition it does not require any intravenous contrast. DWI quantifies the random motion of water in biologic tissue. The apparent diffusion coefficient (ADC) is the most common quantification of this water transport. Cancers are often more cellular than normal tissue, therefore restrict the diffusion of free water, and this forms the basis of DWI in oncology [50]. In breast cancer, a restricted ADC is widely accepted as a marker of cellularity [51–57].
Rahbar et al. looked at 74 pure DCIS lesions and found that quantitatively these lesions demonstrated higher DWI and lower ADC than normal tissue in the same patient, with a statistical significant difference [58]. In a subsequent study Rahbar et al. studied whether 3 T MRI was able to identify low risk DCIS. This study looked at the features of 36 DCIS lesions on MRI, 8 classified as low risk and 28 high risk. Again no statistically significant differences were found for morphologic features and kinetics between low risk and high risk DCIS. However, low risk DCIS lesions showed different DWI features, such as higher contrast to noise ratio and lower normalized ADCs than high-risk DCIS lesions [45].
Iima et al. studied 22 patients with pure DCIS and found that the ADC of high and intermediate grade DCIS were significantly lower than those of low-grade DCIS, and there was a significant negative trend between mean ADC and tumor grade. These preliminary results suggest that possibly DWI may be able to identify patients with low grade DCIS, which if confirmed could decrease patient anxiety and decrease invasive approaches [59].
An additional study by Rahbar et al., suggests that the combination of findings on DCE MRI and DWI may be able to predict low grade from high grade DCIS, with up to 81% accuracy. Larger size lesions corresponded with higher grade DCIS. A higher contrast to noise ratio (CNR), between each lesion and normal tissue on DWI (b = 600 s/mm^2) was seen in non-high grade DCIS which was thought to be related to greater T2-shine through, as no significant difference in ADC values between high grade and non-high grade lesions [45]. This lack of difference between ADC values and grade of DCIS is different than the results of Iima et al., as ADC values are technique-dependent, and further research is required in this area.
9.5 MRI Features Suggestive of Occult Invasion
Microinvasive DCIS is a subtype of disease which shows 1 mm or less of extension of cancer cells through the basement membrane. Hahn et al. found that microinvasive DCIS showed more suspicious MR imaging characteristics than pure DCIS. These findings included spiculated mass-type lesion, segmental distribution, and clustered ring enhancement of nonmass enhancement, and strong initial enhancement kinetics with washout kinetics [60].
The early identification of an invasive cancer along with DCIS, which is different than microvinasive cancer, is important because it results in changes to surgical management, including a sentinel node biopsy [61]. Wisner et al. looked at whether certain MRI BI-RADS criteria or radiologist perception correlated with invasive cancer after initial diagnosis of DCIS on core-biopsy. 13/51 patients with core-biopsy proven DCIS had invasion at excision. There was a significant positive correlation between the presence of a mass and invasion while nonmass enhancement had a significant negative correlation with invasion [62]. Goto et al. found that that certain MR findings of breast lesions, particularly in NME lesions, including large size of lesion and relatively higher signal intensity on fat-saturated-T2 W images, were suggestive of invasion in biopsy proven DCIS [63]. However, Nori et al. did not find MRI morphologic features to be significantly associated with prediction of DCIS plus invasive cancer when looking at cases of DCIS diagnosed on percutaneous biopsy [64]. This is an area where future research attention may be helpful.
9.6 Summary
With the advent of screening mammography the incidence of DCIS has increased significantly. MRI has been shown to be the most sensitive examination in the detection of DCIS. Not only is MR the most sensitive imaging modality but it is likely the one to detect the most clinically relevant cases of DCIS, and it is therefore essential to recognize the various presentations of DCIS on MR imaging. The most common morphology of DCIS is nonmass enhancement, and the most common distribution for the NME is in a segmental pattern. The most common kinetic pattern of DCIS is a fast initial uptake, however there is great variation in the delayed phase. It is thus, essential to evaluate lesions based on the morphologic pattern.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


