In gastrointestinal oncology, one of the most important factors influencing cancer-specific survival is the presence of positive lymph nodes. Although it remains controversial, adequate lymph node examination is required for accurate staging such that patients can receive appropriate adjuvant treatments and for stratification in clinical trials. Nevertheless, wide variation exists in the quality of lymph node examination in the United States, and many centers are not meeting guideline treatment recommendations.
- •
Lymph node status is one of the most important predictors of survival in gastrointestinal cancer.
- •
The number of lymph nodes examined after surgical resection considerably affects staging accuracy, which is relevant for treatment decisions and when stratifying patients in clinical trials.
- •
For colon and rectal cancers, at least 12 lymph nodes should be examined after surgical resection; however, for other cancer sites and after neoadjuvant therapy, the precise number of nodes required is less clearly established.
- •
Current evidence suggests that there is lack of adequate lymph node examination across all gastrointestinal cancers in the United States.
Given these statistics, it is imperative to identify strategies that improve the quality of cancer care in GI oncology. One of the most important predictors of survival is the presence of lymph node metastasis; however, the precise number of examined lymph nodes needed for accurate staging of each cancer site is variable and not always clearly defined. Nevertheless, the number of lymph nodes examined after surgical resection considerably affects staging accuracy, which is relevant for treatment decisions and when stratifying patients in clinical trials. In addition, evidence suggests that the extent of lymphadenectomy could be a surrogate of other unmeasured factors, such as the quality of surgical technique, more thorough pathologic examination, or both. Therefore, to address these issues, this article aims to explore current evidence and controversies with respect to lymph node staging standards in GI oncology.
History
The concept that lymph nodes may act as functional barriers and channels of cancer spread began to be accepted by the mid 1800s. Immediately after, William Halsted, an American-born surgeon, popularized the idea that cancer spreads in an orderly manner by way of lymphatic channels. Based on his own theory, Halsted advocated radical mastectomy for treating women with breast cancer, an operation that removes the breast, underlying muscles, and all lymphatic tissues in the axilla. In this manner, Halsted believed that he was removing all locoregional diseases, particularly cancer cells harbored in axillary lymph nodes, which he postulated would decrease recurrence and ultimately improve survival.
Nevertheless, the role of lymph node sampling in the natural history of cancer continued to evolve. In contrast to the Halstedian theory, a new concept championed by Bernard Fisher and Blake Cady emerged. Fisher in particular believed that lymph node involvement was more an indicator of cancer biology than a step in the sequence toward distant metastases. He did not believe that variations in locoregional therapy were as important as addressing the systemic disease, and pushed for less radical surgical treatments. Fisher went on to cofound the National Surgical Adjuvant Breast and Bowel project and conduct a series of landmark randomized controlled trials that demonstrated, among other important findings, that en bloc resection of axillary lymph nodes and radical surgery in all women with breast cancer were not associated with better outcomes.
A critical notion that emerged out of these trials and other discussions was that standardizing the classification of specific cancers into separate stages was important for both prognostic and treatment purposes, and nodal status was an integral component of overall stage. In 1959, 6 founding organizations (the American Cancer Society, American College of Surgeons [ACS], American Society of Clinical Oncology [ASCO], Centers for Disease Control and Prevention, National Cancer Institute [NCI], and College of American Pathologists) convened to launch the American Joint Committee on Cancer (AJCC). The objective of the AJCC was to define cancer-staging groups that optimized prognostic estimates based on tumor size, nodal status, and presence of distant metastasis. Standardizing cancer staging has allowed researchers to reliably evaluate many important questions in cancer surgery, including those specific to the optimal extent of lymphadenectomy.
Colon cancer
Colon cancer is the fourth most common malignancy diagnosed in the United States, and approximately 80% of patients present with potentially resectable disease. Nodal metastases have long been recognized as the most important factor that predicts long-term survival and are an important determinant in the decision to administer adjuvant chemotherapy. With the demonstration of highly effective systemic therapies for colon cancer over the last decade, it is essential to ensure that all patients who would benefit from such treatment are well staged and have access to these therapies.
Studies have shown an improvement in disease-specific and overall survival when increasing numbers of lymph nodes are examined for colon cancer. This improvement in outcomes is due in part to stage migration or more accurate staging that allows for increased use of adjuvant chemotherapy. Although estimates have varied widely, numerous studies and consensus guidelines (eg, College of American Pathologists Consensus Statement 1999 ) have suggested that the examination of 12 regional lymph nodes is a reasonable minimum for adequate nodal evaluation of colon cancer. Despite these findings, population-based assessments have shown that most patients in the United States do not have 12 or more nodes examined. This assessment, in part, motivated the ACS, ASCO, and National Comprehensive Cancer Network (NCCN) to harmonize a quality measure requiring the resection and pathologic examination of 12 or more lymph nodes for the evaluation of colon cancer. Subsequently, the National Quality Forum endorsed the 12-node measure for quality surveillance.
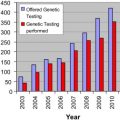
Using data from the National Cancer Data Base (NCDB) and examining treatment of colon cancer in patients who underwent colectomy at 1296 hospitals, Bilimoria and colleagues found that although the proportion of compliant hospitals increased considerably during the study period, 60% of hospitals failed to comply with the 12-node measure ( Fig. 1 ). Prior studies conducted at the level of individual patients have demonstrated that approximately 37% to 50% of patients with colon cancer in the United States have 12 or more nodes examined. Nodal evaluation is likely to improve further with the development of the 12-node measure for quality, as physicians and hospitals recognize that the requirement to examine 12 or more nodes may affect referral and reimbursement. This quality measure will also soon be reported publicly.
Colon cancer
Colon cancer is the fourth most common malignancy diagnosed in the United States, and approximately 80% of patients present with potentially resectable disease. Nodal metastases have long been recognized as the most important factor that predicts long-term survival and are an important determinant in the decision to administer adjuvant chemotherapy. With the demonstration of highly effective systemic therapies for colon cancer over the last decade, it is essential to ensure that all patients who would benefit from such treatment are well staged and have access to these therapies.
Studies have shown an improvement in disease-specific and overall survival when increasing numbers of lymph nodes are examined for colon cancer. This improvement in outcomes is due in part to stage migration or more accurate staging that allows for increased use of adjuvant chemotherapy. Although estimates have varied widely, numerous studies and consensus guidelines (eg, College of American Pathologists Consensus Statement 1999 ) have suggested that the examination of 12 regional lymph nodes is a reasonable minimum for adequate nodal evaluation of colon cancer. Despite these findings, population-based assessments have shown that most patients in the United States do not have 12 or more nodes examined. This assessment, in part, motivated the ACS, ASCO, and National Comprehensive Cancer Network (NCCN) to harmonize a quality measure requiring the resection and pathologic examination of 12 or more lymph nodes for the evaluation of colon cancer. Subsequently, the National Quality Forum endorsed the 12-node measure for quality surveillance.
Using data from the National Cancer Data Base (NCDB) and examining treatment of colon cancer in patients who underwent colectomy at 1296 hospitals, Bilimoria and colleagues found that although the proportion of compliant hospitals increased considerably during the study period, 60% of hospitals failed to comply with the 12-node measure ( Fig. 1 ). Prior studies conducted at the level of individual patients have demonstrated that approximately 37% to 50% of patients with colon cancer in the United States have 12 or more nodes examined. Nodal evaluation is likely to improve further with the development of the 12-node measure for quality, as physicians and hospitals recognize that the requirement to examine 12 or more nodes may affect referral and reimbursement. This quality measure will also soon be reported publicly.
Rectal cancer
Rectal cancer exemplifies the Halstedian theory of cancer progression, that is, spreading in an orderly manner via surrounding lymphatic channels. However, lymph node resection in rectal carcinoma presents some distinct challenges. In 1979, Heald first described the total mesorectal excision (TME), a procedure that removes all regional lymph nodes in the mesorectum, since demonstrated to substantially decrease tumor recurrence and improve survival. However, the adequacy of TME may vary considerably even among experienced surgeons. For example, in the Dutch TME trial, even after surgical standardization was performed among all participating surgeons, the quality of TME specimens was inadequate in as many as one-third of patients who were treated with abdominoperineal resection.
Another challenge in rectal cancer is determining the optimal number of lymph nodes that should be examined after neoadjuvant therapy. Although treatment guidelines for rectal cancer are similar to those of colon cancer indicating that at least 12 nodes should be examined, patients with T3/T4 or N+ rectal cancers should receive neoadjuvant therapy. Because preoperative chemoradiotherapy may reduce the number of nodes available for examination, the precise number of nodes, if any, that should be optimally removed is unclear. Estimates in the literature are variable, ranging between 0 and 20, and there is yet to be a clear consensus. For example, in a recent report from the MD Anderson Cancer Center, over a 14-year period Tsai and colleagues found that when 7 or more nodes were examined, patients showed decreased tumor recurrence and improved cancer-specific survival. By contrast, Rullier and colleagues failed to find any association between the number of nodes examined and survival. Although this issue remains controversial, it is clear that staging of lymph nodes is important whether or not neoadjuvant therapy is administered. At present, the authors continue to advocate that surgeons and pathologists continue to follow guidelines recommending the examination of at least 12 lymph nodes.
Similar to colon cancer, in rectal cancer, hospital-level performance with respect to lymph node examination rates is variable. In one of the few population-based studies evaluating the number of patients with colorectal cancer with at least 12 lymph nodes examined, Baxter and colleagues found that rectal cancer was an independent factor associated with decreased lymph node harvests. The study also reported that overall only 23% of patients with stage I cancer received adequate lymph node evaluation. Nevertheless, rectal carcinoma poses unique challenges, and further research is required to elucidate these controversies.
Related posts:
 Variation in Mortality After High-Risk Cancer Surgery
Variation in Mortality After High-Risk Cancer Surgery
 Unexpected Readmissions After Major Cancer Surgery
Unexpected Readmissions After Major Cancer Surgery
 Racial Differences and Disparities in Cancer Care and Outcomes
Appropriate Use of Surgical Procedures for Patients with Cancer
Racial Differences and Disparities in Cancer Care and Outcomes
Appropriate Use of Surgical Procedures for Patients with Cancer
 Collaboration with the Community Cancer Center
Collaboration with the Community Cancer Center
 Value-Based Health Care
Value-Based Health Care
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


