, Hans Guski2 and Glen Kristiansen3
(1)
Carl-Thiem-Klinikum, Institut für Pathologie, Cottbus, Germany
(2)
Vivantes Klinikum Neukölln, Institut für Pathologie, Berlin, Germany
(3)
Universität Bonn, UKB, Institut für Pathologie, Bonn, Germany
2.1 Cytokeratins
Cytokeratins are the most important markers used for the diagnosis of epithelial neoplasms. Cytokeratins are intermediate filament proteins building an intracytoplasmic network between the nucleus and cell membrane of epithelial cells. Cytokeratins are a complex family composed of more than 20 isotypes and divided into 2 types [1, 2].
Type I (acidic group) including cytokeratins 9–20
Type II (basic group) including cytokeratins 1–8
Different cytokeratins are expressed in different epithelial types and at different stages of differentiation; consequently, different epithelial types have different specific cytokeratin expression profiles, which usually remains constant after neoplastic transformation [3–5].
Often cytokeratins from the acidic group are paired with their basic counterpart such as CK8 and CK18 that frequently go together. In immunohistochemical sections, cytokeratins reveal typically a diffuse cytoplasmic expression pattern; nevertheless, abnormal staining patterns such as perinuclear and dot-like expression patterns are characteristic for different neuroendocrine tumors. The following examples demonstrate this phenomenon, which is also of diagnostic value:
- 1.
Merkel cell carcinoma with perinuclear cytokeratin deposits (mainly cytokeratin 20)
- 2.
Small cell carcinoma (mainly cytokeratin 19)
- 3.
Carcinoid tumors and pancreatic endocrine tumors
- 4.
Renal oncocytoma (with low molecular weight cytokeratins)
- 5.
Medullary thyroid carcinoma
- 6.
Seminoma (with low molecular weight cytokeratins)
- 7.
Granulosa cell tumor
- 8.
Rhabdoid tumor
- 9.
Few mesenchymal tumors including desmoplastic small round cell tumor, leiomyosarcoma, and monophasic synovial sarcoma
The most commonly used cytokeratins in routine histopathology are listed in this chapter in addition to other frequently used epithelial markers such as epithelial membrane antigen, epithelial specific antigen, carcinoembryonic antigen, p63, p40, claudin, and different mucins.
Pan-cytokeratin and cytokeratin cocktails | ||
|---|---|---|
Expression pattern: cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Screening for epithelial neoplasms | See diagnostic pitfalls below | Epithelial and myoepithelial cells |
Positive control: appendix, tonsil | ||
Diagnostic Approach
Before the interpretation of a pan-cytokeratin stain, it is always to consider that there is no pan-cytokeratin that reacts absolutely with all cytokeratins; nevertheless, cytokeratin cocktails are very effective in screening for epithelial differentiation or epithelial neoplasms [6]. The following cytokeratin cocktails and clones are the most commonly used markers in routine immunohistochemistry:
AE1/AE3 is a mixture of both AE1 and AE3, whereas AE1 reacts with type I cytokeratins and AE3 with type II cytokeratins. AE1/AE3 is a widely used as pan-cytokeratin marker but lacks the reactivity with cytokeratin 18. Few epithelial tumors are negative or weakly positive for this cocktail such as hepatocellular and renal cell carcinoma, adrenal cortical carcinoma, prostatic adenocarcinomas, and neuroendocrine tumors. Cross-reactivity of this cocktail with glial fibrillary acidic protein (GFAP) is reported and can be a source of interpretation error [7].
KL1 is a broad-spectrum cytokeratin clone that reacts with the cytokeratins 1/2/5/6/7/8/11/14/16/17/18, which makes it one of the best broad-spectrum epithelial markers. Similarly, the AE1/AE3 cocktail KL1 shows also cross-reactivity with GFAP.
MNF116 is a cytokeratin clone that reacts with the cytokeratins 5/6/8/17/19.
CAM 5.2 is a cytokeratin clone that reacts with the cytokeratins 8/18/19.
MAK-6 is a cytokeratin clone that reacts with the cytokeratins 14/15/16/18/19.
Cytokeratin OSCAR is a broad-spectrum cytokeratin that reacts with the majority of epithelial cell types and carcinomas derived from these cells. Cytokeratin OSCAR reacts with the cytokeratins 7, 8, 18, and 19. Cytokeratin OSCAR does not show cross-reactivity with GFAP, but it reacts with follicular dendritic cells in lymphatic tissue.
Diagnostic Pitfalls
Different cytokeratins are also expressed in various non-epithelial tissue types and neoplasms or in tumors with features of epithelial differentiation. The following list represents the most popular examples:
Mesothelial cells and mesothelioma
Smooth muscle and smooth muscle tumors
Meningioma and chordoma
Epithelioid sarcomas
Synovial sarcoma
Desmoplastic small round cell tumor
Angiosarcoma
A small subset of alveolar rhabdomyosarcoma
Clear cell sarcoma
Subset of germ cell tumors
Nerve sheath tumors
Rhabdoid tumor
Malignant melanoma
Undifferentiated pleomorphic sarcoma
Proliferating myofibroblasts
Anaplastic and diffuse large cell lymphomas [8]
Plasma cell neoplasms
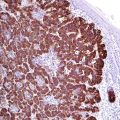
The aberrant expression of cytokeratin in mesenchymal tumors is usually patchy and may show dot-like expression pattern. The diagnosis of carcinoma based only on a positive pan-cytokeratin reaction is one of the sources of serious mistakes in tumor diagnosis. For appropriate diagnosis, it is always advisable to determine the cytokeratin profile of the tumor and then to search for other tissue-specific markers. Ectopic benign epithelial structures in lymph nodes such as heterotopic ducts and glands in cervical, thoracic, and abdominal lymph nodes in addition to Müllerian epithelial inclusions and endometriosis in pelvic lymph nodes must be kept in mind in screening lymph nodes for metastatic carcinoma or disseminated tumor cells (Fig. 2.1).
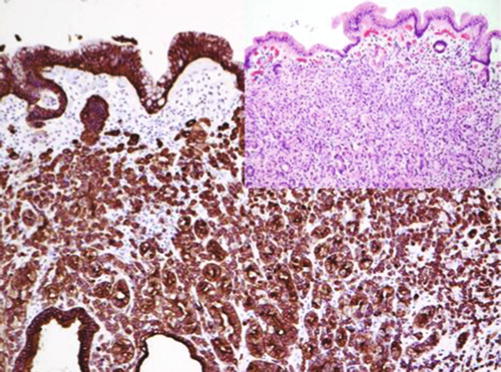
Fig. 2.1
Pan-cytokeratin (CK MNF116) highlighting the neoplastic cells in diffuse gastric adenocarcinoma
Cytokeratin 5 | ||
Expression pattern: cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Squamous cell carcinoma, mesothelioma, myoepithelial tumors | Myoepithelial cells in prostatic and mammary glands, basal-like phenotype breast carcinoma, adrenocortical tumors | Squamous epithelium, basal-type epithelial cells, myoepithelial cells, transitional epithelium, mesothelial cells, cornea |
Positive control: tonsil | ||
Diagnostic Approach
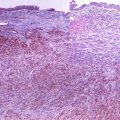
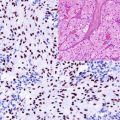
Cytokeratin 5 is a type II cytokeratin and a main component of the cytoskeleton of basal cells of stratified epithelium. Cytokeratins 5, 6, and 14 are related cytokeratins expressed in stratified squamous epithelium, myoepithelium, and mesothelium. This expression spectrum makes these cytokeratins valuable markers for the diagnosis of squamous cell carcinoma. They also clearly label normal myoepithelial cells, myoepithelial cell components in some tumors such as salivary gland tumors and myoepithelial tumors. Highlighting the myoepithelial cells using this group of cytokeratins is essential for the interpretation of prostatic biopsies, as basal cells are absent in neoplastic prostatic glands. An identical approach is also important to distinguish between simple hyperplasia, atypical ductal hyperplasia, and ductal carcinoma in situ (DCIS) in breast biopsies highlighting the myoepithelial and luminal cells with the cytokeratins 5/6/14 and 8/18, respectively. Cytokeratins 5/6/14 are highly expressed in mesothelial cells and are not suitable for discriminating between squamous cell carcinoma and mesothelioma in pleural or peritoneal biopsies or cytology (Fig. 2.2). This group of cytokeratins is usually absent in gastrointestinal adenocarcinomas, germ cell tumors, prostatic carcinoma, thyroid tumors, and hepatocellular and renal cell carcinomas.
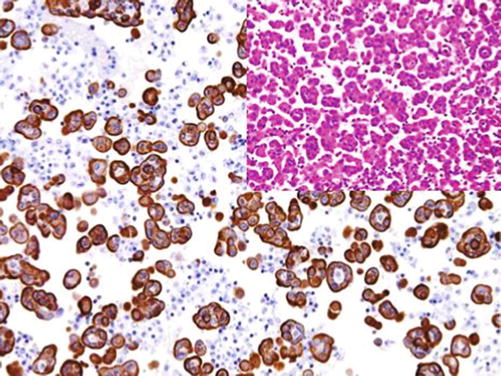
Fig. 2.2
Mesothelioma cells labeled by cytokeratin 5 in pleural effusion
Recently, CK5/14 is frequently replaced by p63 and p40 that highlights the nuclei of myoepithelial and basal cells of the glands as well as the basal and intermediate cells of squamous epithelium and urothelium [1]. Both markers are discussed below.
Cytokeratin 6 | ||
Expression pattern: cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Squamous cell carcinoma | Poorly differentiated breast carcinoma (basal-like phenotype breast carcinoma) | Suprabasal cells, hair shaft, nail |
Positive control: Tonsil | ||
Diagnostic Approach
Cytokeratin 6 is a type I cytokeratin with the same tissue distribution as cytokeratin 5 and is usually used in routine immunohistochemistry as cocktail with cytokeratin 5.
Cytokeratin 7 | ||
Expression pattern: cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Adenocarcinomas of the lung, salivary glands, upper gastrointestinal tract, pancreas, biliary tract, breast, endometrium, transitional cell carcinoma, ovarian serous tumors | Thyroid carcinoma, papillary and chromophobe renal cell carcinoma, mesothelioma, synovial sarcoma, Merkel cell carcinoma | Epithelium of the upper gastrointestinal tract, salivary glands, biliary tract, pancreas, lung, female genital tract, renal collecting ducts, transitional epithelium, mesothelial cells, thyroid follicle cells, endothelia |
Positive control: appendix | ||
Diagnostic Approach
Cytokeratin 7 is a type II cytokeratin expressed in the majority of ductal and glandular epithelium in addition to transitional epithelium of the urinary tract. Cytokeratin 7 is one of the main markers for the diagnosis of adenocarcinoma of different origin; hence, it cannot be used alone to differentiate between primary and metastatic adenocarcinoma. An important diagnostic criterion is the co-expression of cytokeratin 7 and cytokeratin 20 (see diagnostic algorithms 1.6, 1.7, and 1.8) [2]. Cytokeratin 7 is strongly expressed by mesothelial cells and not suitable for discriminating between adenocarcinoma and mesothelioma.
Diagnostic Pitfalls
In the differential diagnosis between adenocarcinoma and squamous cell carcinoma, it is important to keep in mind that a minor component of cytokeratin 7-positive cells can be found in squamous cell carcinoma of different locations including carcinoma of the head and neck, lung, esophagus, and uterine cervix, mainly in poorly differentiated carcinoma. Cytokeratin 7 can also be expressed in non-epithelial tumors such as the epithelioid component of synovial sarcoma. Cytokeratin 7 is usually absent in seminoma and yolk sac tumors, epidermal squamous cell carcinoma, prostatic carcinoma, and pituitary tumors.
Cytokeratin 8 (tissue polypeptide antigen, TPA) | ||
Expression pattern: cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Adenocarcinoma of the lung, GIT, pancreas, biliary tract, breast, endometrium and transitional cell carcinoma, hepatocellular carcinoma, renal cell carcinoma, prostatic carcinoma, neuroendocrine carcinoma | Ameloblastoma, leiomyosarcoma, malignant rhabdoid tumor | Epithelium of the gastrointestinal tract, salivary glands, biliary tract, pancreas, lung, female genital tract, hepatocytes, proximal renal tubules, transitional epithelium, mesothelial cells, smooth muscle cells, myofibroblasts, arachnoid cells |
Positive control: appendix | ||
Diagnostic Approach
Cytokeratin 8 is a type II cytokeratin usually building heterodimer with cytokeratin 18. Both cytokeratins 8 and 18 are intermediate filament proteins expressed in the early embryonal stages and persist in adult simple epithelium. Cytokeratin 8 is usually positive in non-squamous carcinomas and accordingly cannot be used to discriminate between adenocarcinoma types. Cytokeratin 8b stains also few mesenchymal tumors such smooth muscle tumors and malignant rhabdoid tumor.
Diagnostic Pitfalls
Cytokeratin 8 reacts with several non-epithelial tissues and tumors such as smooth muscle cells and leiomyosarcoma.
Cytokeratin 10 | ||
Expression pattern: Cytoplasmic | ||
Main diagnostic use | Expression in other tumors | Expression in normal cells |
Squamous cell carcinoma | Breast ductal carcinoma | Keratinizing epithelium (suprabasal cells) |
Positive control: Tonsil | ||
Diagnostic Approach
Cytokeratin 10 is type I cytokeratin and intermediate filament usually associated with cytokeratin 1. Cytokeratin 10 is expressed in keratinizing and nonkeratinizing squamous epithelium. In routine immunohistochemistry, cytokeratin 10 is used in a cocktail with cytokeratins 13 and 14 as marker for squamous cell carcinoma.