 Figure 5.1. Axial contrast-enhanced CT image from a patient with a thyroglossal duct cyst (TGDC) demonstrates the basic tissue densities on CT. As discussed in greater detail in the text, there is progressively increasing density of air (dark black), subcutaneous fat, fluid or water (within the TGDC), muscle (soft tissue), and bone. Various intermediate densities are seen, such as the brightly opacified carotid arteries (CA), secondary to a higher concentration of intravenous iodinated contrast, with density much higher than muscle but less than bone. |
Table 5.1 Basic Tissue and Tumor Characteristics on Contrast-Enhanced CT | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
typically between -1,000 and +3,000 HU. Increased iodine content of a tissue also results in increased density of that tissue, which forms the basis of contrast-enhanced CT images.
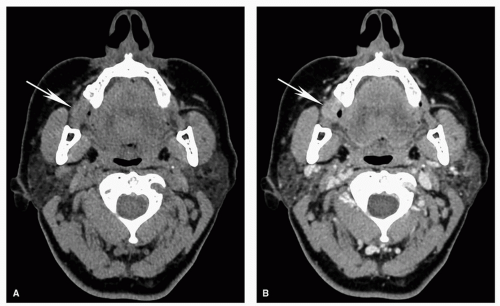 Figure 5.2. Contrast-enhanced neck CT for tumor evaluation. Axial CT images obtained (A) before and (B) after administration of IV contrast from a 59-year-old woman with a right buccal squamous cell carcinoma (arrow) are shown. A: Without IV contrast, there is asymmetry at the site of tumor, but the density is nearly identical (isodense) to muscle, and it is very difficult to clearly visualize the tumor margins. B: After administration of IV contrast, there is differential enhancement of tumor compared to adjacent soft tissues with better delineation of tumor margins. |
Commonly used display windows are also usually preprogrammed using different function keys for easy and rapid access.
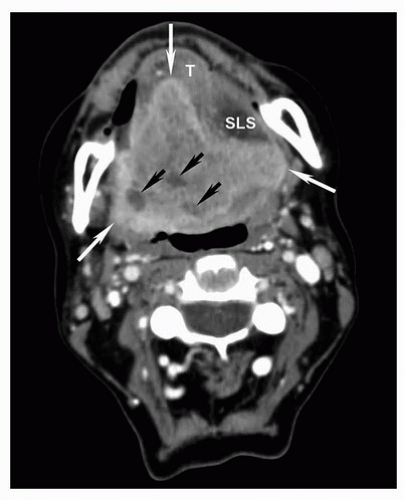 Figure 5.3. Contrast-enhanced neck CT for tumor evaluation and delineation. Axial contrast-enhanced CT image from a 56-year-old woman with a large invasive oral tongue cancer is shown. Because of differences in tumor vascularity compared to normal tissues, contrast-enhanced images are used to distinguish tumor from otherwise similar density soft tissues such as muscle. Note the clear demarcation of the enhancing edge of tumor (white arrows). The small low-density areas within the tumor represent areas of cystic change and necrosis (small black arrows). T, tongue muscles; SLS, sublingual space. |
 Figure 5.4. Optimal window display for evaluation of bones on CT. Axial contrast-enhanced CT images are shown from a 67-year-old woman with squamous cell carcinoma of the right gingivobuccal sulcus with extension to the retromolar trigone. The same slice is shown using two different reconstruction algorithms and display windows. A: Image displayed using narrow soft tissue windows is used for demonstration and evaluation of the mass (white arrows) and adjacent soft tissues. Notice how the cortex of the mandible is very bright when displayed in soft tissue windows with poor visualization of bone architecture (black arrow). This image is not diagnostic of cortical invasion. B: The same slice reconstructed and displayed in bone “algorithm” demonstrates a small defect (arrow) corresponding to a pathologically proven focal cortical invasion of the mandible, resulting in a T4 stage designation. Note that although the bone windows demonstrate cortical invasion to better advantage, the soft tissue mass itself is poorly seen using these display parameters. |
diagnostic quality of the examination. This results in increased propensity to motion artifact, particularly below the hard palate, where there can also be image degradation secondary to swallowing artifact. A more detailed comparison of the two techniques will be provided later.
 Figure 5.5. Superior soft tissue contrast of MRI compared to CT. Axial CT (A) and MRI (B, C) images are shown from a patient with an adenoid cystic carcinoma involving the right hard palate. On the contrast-enhanced CT image, the approximate area of the lesion is marked by the arrows. The lesion is not clearly visible on CT, and only mild asymmetry and minimal heterogeneous density are seen in the region of the tumor. STIR (B) and contrast-enhanced T1w fatsuppressed MR images (C), on the other hand, demonstrate abnormal high signal and heterogeneous enhancement in the right hard palate (arrows, B and C, respectively). Although CT typically enables excellent tumor delineation, occasionally, such as in this case, the lesion is much better seen on MRI because of MRI’s superior soft tissue contrast. |
to motion artifact, which can degrade image quality. Therefore, the MRI protocols are designed carefully and optimized to achieve the best result taking into account these variables. When detailed evaluation of a small area of interest, such as skull base foramina, is required, this is best performed as a targeted exam focusing on the area of interest, rather than an evaluation of the entire neck, if possible. An optimal examination is designed to achieve reasonable scan times that can be tolerated by the patient and also enable acquisition of high-quality images without significant motion degradation and image distortion.
Table 5.2 Basic MRI Sequences and Tissue Characteristics | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
MRI for cancers below the level of the hard palate. CT is also a safer environment for the evaluation of acutely ill patients or patients with respiratory difficulties who would have difficulty lying still in the supine position for a prolonged period of time.
 Figure 5.6. T1w and contrast-enhanced imaging for evaluation of cancer of the head and neck. Images are shown from a 59-yearold man with oral tongue squamous cell carcinoma. A: Axial T1w image without fat suppression. As discussed in the text, there is good depiction of normal anatomy. Muscle has intermediate signal (e.g., MS, masseter), and fat is very bright (or hyperintense), for example, the subcutaneous fat (black asterisk). Cortical bone is dark, whereas the fatty marrow is bright (A, e.g., white circle around the right mandibular ramus). The tumor (T) has intermediate signal on the unenhanced T1w image and is not very conspicuous. Because this patient has a relatively fatty tongue, the tumor margins are still visible. B: Postcontrast axial T1w image without fat suppression. Because of the intrinsically bright signal associated with the fat in the tongue, this sequence does not show the enhancing tumor (T) well. Postcontrast axial (C) and coronal T1w image (D), both with fat suppression. Note how the enhancing tumor (T) is much more conspicuous on the fat-suppressed images compared to the non-fat-suppressed image (B). |
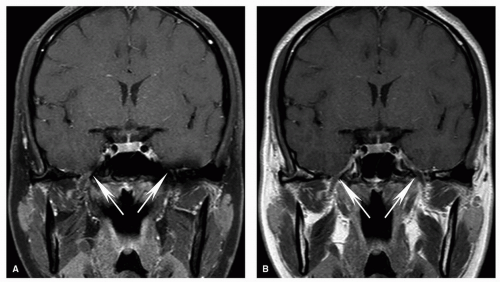 Figure 5.7. Effects of fat suppression on artifacts at the skull base. Coronal postcontrast T1w images with fat suppression (A) and without fat suppression (B) are shown. On the fat-suppressed image (A), the foramen ovale (arrows) is partly obscured bilaterally, especially on the left side. On the other hand, the foramen ovale is well seen bilaterally on the T1w image obtained without fat suppression (B, arrows), and a normal intermediate signal V3 branch is well seen on both sides. Therefore, although fat-suppressed T1w images are the primary sequence for evaluation of lesion enhancement, in select cases, addition of a non-fat-suppressed T1w sequence can improve diagnostic evaluation. |
 Figure 5.8. Denervation changes on MRI and utility of fat-suppressed T2w images. Axial fat-suppressed T2w (A) and contrast enhanced T1w (B) images are shown from a 43-year-old woman with recurrent nasopharyngeal cancer to the left Meckel cave (not shown). There are typical denervation changes in the distribution of the mandibular division of the left trigeminal nerve (V3) with hyperintense T2 signal (A) and abnormal enhancement (B) in the lateral pterygoid (LP), temporalis (TP), and masseter (MS) muscles. Note the preservation of muscle architecture with striations that is typical of denervation change and should not be mistaken for tumor. Fat-suppressed T2w images (or STIR images—not shown) are excellent for demonstrating edema. |
 Figure 5.9. Tumor appearance on STIR images. STIR image is shown from the same case displayed in Figure 5.6. Note the bright signal of the tongue cancer (T) compared to adjacent tissues. Fluid, such as that of cerebrospinal fluid (CSF), is very bright on STIR. |
Table 5.3 Comparison of Relative Strengths of CT and MRI for Head and Neck Cancer Imaging | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
which in turn can be detected and localized with a PET scanner. When integrated with an anatomic technique like CT, this provides a robust functional evaluation while enabling accurate anatomic localization, which is very important given the complex anatomy in the head and neck. Therefore, current standard practice is to perform a combined PET/CT for evaluation of head and neck cancer.13,14 Most PET/CTs for head and neck cancer are performed using the radiopharmaceutical 2-18F-fluoro-2-deoxy-D-glucose (FDG), a glucose analog that is taken up by cells but is not metabolized.13,14 The rationale for FDG-PET cancer imaging is that in general, cancer cells have greater uptake on PET than do normal tissues (known as Warburg effect) (Fig. 5.10). However, one must take into account that increased FDG uptake is not specific to cancer cells and may be seen in context of inflammation/infection including biopsy sites, some benign neoplasms, or increased muscular activity under certain circumstances. This needs to be taken into account when interpreting PET scans; to be discussed later.
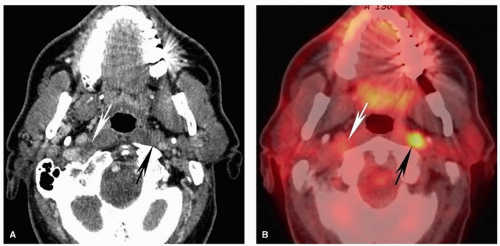 Figure 5.10. Advantages and pitfalls of PET for detection of metastatic lymph nodes. Axial contrast-enhanced CT scan (A) and fused PET image (B) are shown from a 60-year-old man with squamous cell carcinoma of the left lateral pharyngeal wall (not shown). There is abnormal, markedly increased uptake in the left lateral retropharyngeal lymph node (black arrow) that on the CT is barely visible and cannot be convincingly characterized as abnormal but which is quite evident on the PET study. This illustrates the increased sensitivity of PET compared to CT. On the other hand, there is a subtle but clearly necrotic, pathologic right lateral retropharyngeal lymph node seen on CT without significant uptake on PET (white arrow). Necrotic nodes are a known potential pitfall of PET because there may be insufficient metabolically active tissue to permit visual detection. This case highlights the importance of combined interpretation of a diagnostic CT and PET scan. |
performed in 199319 and has been used by some for evaluation of head and neck cancer.20 Therefore, although it is useful as a reference for potential pathology, there is no clear evidence that this threshold can be extrapolated to lymph nodes or tissues and lesions outside the thorax. For example, others have used an SUV of 3.5 to 4 as threshold for evaluation of lymphadenopathy,21 and one study showed that the greatest specificity for determination of metastatic nodal disease in squamous cell carcinoma (SCC) was achieved when a threshold of 5 was used.22 As discussed by Escott,13 another pitfall of using strict SUV criteria for determination of lymphadenopathy is that small pathologic lymph nodes may have an SUV value below an accepted threshold and thus be visually difficult to call abnormal. This highlights the importance of using the SUV as a guide, rather than absolute determining value, and carefully correlating with findings on the contrastenhanced CT for determination of pathologic lesions and lymphadenopathy.
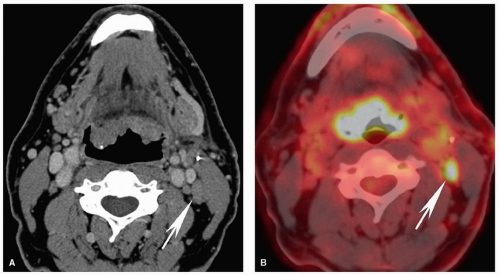 Figure 5.11. Pitfalls and false positives in PET: lymphoid tissues of the Waldeyer ring. Axial contrast-enhanced CT scan (A) and fused PET image (B) are shown from a 50-year-old with carcinoma of unknown primary who presented with an N2C neck. On CT, there are enlarged lingual tonsils at the base of the tongue without a focal enhancing mass. On PET, there is diffusely increased uptake of this lymphoid tissue. However, all base of tongue biopsies were negative. Note the pathologic level IIb node detected on PET (arrow). On CT, the node is prominent but cannot be characterized as abnormal by anatomic imaging criteria. |
when necessary help with biopsy planning. Imaging can also be helpful in clinically misleading presentations, and sometimes the radiologist is the first to suggest the presence and site of a head and neck cancer (Fig. 5.14). However, frequently, at the time of initial evaluation, the diagnosis has already been made, and the main role of imaging is to stage the tumor. The added value of imaging in that scenario is typically to upstage the clinical assessment by identifying involvement of critical structures, lymph nodes, or distant metastases that are not reliably identified clinically. Imaging can also guide biopsy when there are potentially important equivocal findings. Furthermore, imaging plays a key role in follow-up and surveillance of cancers to evaluate response to treatment, progression of disease, and tumor recurrence.
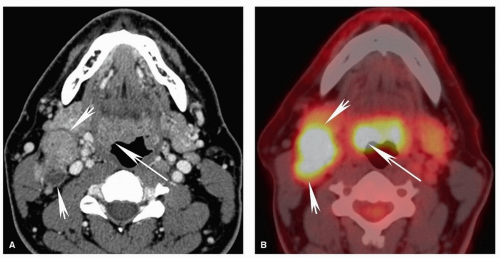 Figure 5.12. Pitfalls and false positives in PET: lymphoid tissues of the Waldeyer ring. Axial contrast-enhanced CT scan (A) and fused PET image (B) are shown from a 52-year-old with biopsy-proven squamous cell carcinoma of the right base of the tongue. Similar to the case in Figure 5.11, there is diffuse uptake at the base of the tongue without clear focally increased uptake at the site of tumor on the right (long arrow). On CT, there is asymmetric enlargement of the right base of tongue tissues (long arrow). Although by itself this is insufficient for a confident diagnosis, it is useful for directing the biopsy, which demonstrated cancer at that site. Note the large, partly necrotic, right level II pathologic nodal mass with diffusely increased uptake on PET (short arrows). |
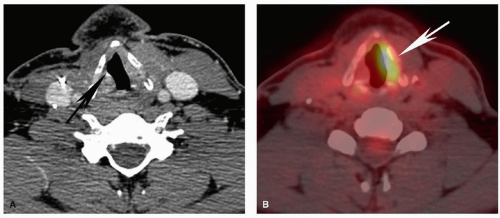 Figure 5.13. Pitfalls and false positives in PET: asymmetric muscle uptake associated with vocal cord paralysis. Axial contrastenhanced CT scan (A) and fused PET image (B) are shown from a 33-year-old patient operated for thyroid cancer with right vocal cord paralysis. The CT image demonstrates a patulous laryngeal ventricle on the right (black arrow) typical of vocal cord paralysis. The PET image demonstrates typical compensatory increased activity in the normal left true vocal cord (white arrow). This should not be mistaken for tumor. |
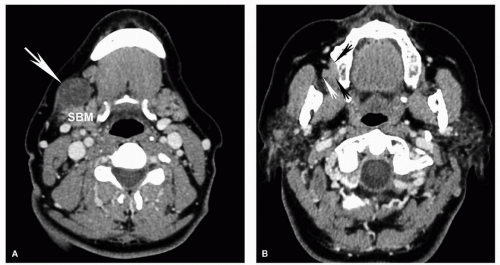 Figure 5.14. Nodal metastasis from squamous cell carcinoma presenting clinically as a submandibular region mass. Axial contrastenhanced CT images in a patient referred for evaluation of a new right submandibular mass demonstrate an inhomogeneous enlarged level IB node (large arrow; A) anterior to the submandibular gland (SBM), compressing and displacing the gland posteriorly. Images more superiorly demonstrate a small buccal mucosal primary cancer (small arrows; B). The small black arrows mark the medial margin of the tumor. The small white arrow marks the lateral margin of the tumor, resulting in partial obliteration and asymmetry of adjacent buccal space fat. Evaluation of subtle loss of symmetry is very useful for detection of small lesions in the neck. |
of intrinsic contrast on both CT and MRI and is clearly distinguishable from soft tissue characteristics of most nonlipomatous tumors. Careful evaluation of infiltration and obliteration/asymmetry in the fat within and fat planes separating various structures and spaces in the neck will enable identification of small tumors and areas of tumor infiltration (Fig. 5.14). Familiarity with the detailed anatomy of the neck is an essential asset to help evaluation. Disruption of normal tissue architecture is also important for evaluating tumor infiltration. For example, the preserved striated architecture of denervated muscle should enable
distinction from tumor invasion despite the abnormal signal (Fig. 5.8). By taking into account all the different characteristics, an optimal imaging evaluation and lesion characterization can be performed. Information from the PET scan complements the anatomic information provided on CT and MRI and can increase sensitivity for detection of tumor, lymphadenopathy, and recurrence in head and neck squamous cell carcinoma (HNSCC).13
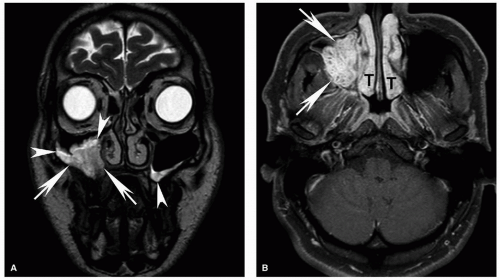 Figure 5.15. Adenoid cystic carcinoma of the maxillary sinus. Coronal T2w (A) and axial postcontrast T1w (B) fat-suppressed images from a 26-year-old patient. On T2w images, the tumor (arrows) is hyperintense to muscle but not strikingly bright. There is only a small amount of secretions and inflammatory mucosal changes on either sides (arrowheads), with higher signal than the tumor on T2w images (A). There is heterogeneous but robust enhancement of the tumor arrows in (B). The normal enhancement of the lining of nasal turbinates (T) should not be mistaken for tumor. In cases when tumor abuts the turbinates, this distinction may be more difficult, but careful evaluation of contiguity with the main tumor mass and subtle signal changes on all sequences may be helpful for making the distinction. |
 Figure 5.16. Buccal squamous cell carcinoma. Coronal T2w (A) and contrast-enhanced fat-suppressed T1w (B) images. The mass is heterogeneous and appears hyperintense to muscle on T2w images with heterogeneous enhancement that is greatest around its margins. |
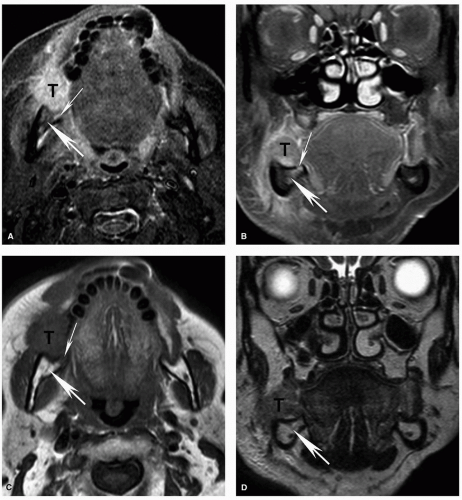 Figure 5.17. Superficial invasion of the mandibular cortex with reactive marrow edema on MRI. Axial STIR (A), coronal contrastenhanced fat-suppressed T1w (B), axial T1w (C), and coronal T2w (D) MRI images are shown from the same patient whose CT is shown in Figure 5.4. Corresponding to the small focal cortical break seen on CT, there is a potential defect (thin arrow), although the MRI is less convincing than the CT. There is also mildly increased signal within the marrow (thick arrow) on the STIR (A) and contrast-enhanced (B) images, demonstrating the increased sensitivity of MRI for detecting subtle marrow changes. However, in this case, the fat within the marrow is preserved on the T1w image (C; thick arrow) and the signal is normal on the T2w image (D; thick arrow). This suggests that the mild signal abnormality represents reactive marrow edema and not true marrow invasion. Pathology confirmed superficial cortical invasion without marrow invasion. |
arch. Level IV nodes are internal jugular chain nodes that extend from the level of the lower margin of the cricoid cartilage arch to the level of the top of the manubrium. Level V nodes are posteriorly located lymph nodes that are subdivided into levels VA and VB. Level VI nodes are the visceral nodes, and level VII nodes are those that lie caudal to the top of the manubrium, located between the medial margins of the left and right common carotid arteries in the substernal region45,46,47 (Fig. 5.19; Table 5.4). Please refer to Table 5.4 for a detailed description of the anatomic landmarks used for the imaging classification.
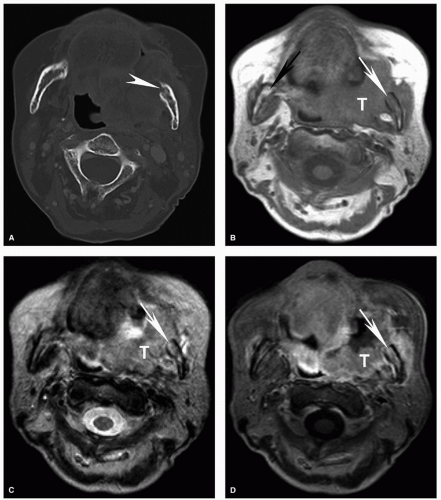 Figure 5.18. Increased sensitivity of MRI for determination of invasion of the bone marrow compared to CT. Axial CT displayed in bone windows (A) and unenhanced T1w (B), T2w (C), and contrast-enhanced fat-suppressed T1w (D) MRI images are shown from a patient with an advanced squamous cell carcinoma of the retromolar trigone (T) with invasion of multiple adjacent spaces including the buccal space, masticator space, and oropharynx. On CT, the cortical invasion of the left mandible is subtly evident (arrowhead). However, the marrow invasion is not clearly demonstrated. On the MRI, however, there is clear invasion of the marrow with replacement of the normal marrow fat in the mandibular ramus with tumor (white arrow). Note the difference compared to the normal marrow of the contralateral mandibular ramus, particularly well seen on the unenhanced T1w image (B, black arrow). Unlike reactive marrow edema shown in Figure 5.17, the marrow signal abnormality follows the signal of large extraosseous tumor mass on all sequences, a key feature for differentiating the two on imaging. |
Table 5.4 Landmarks Used for Cervical Lymph Node Localization Using the Imaging-Based Classification | |||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


