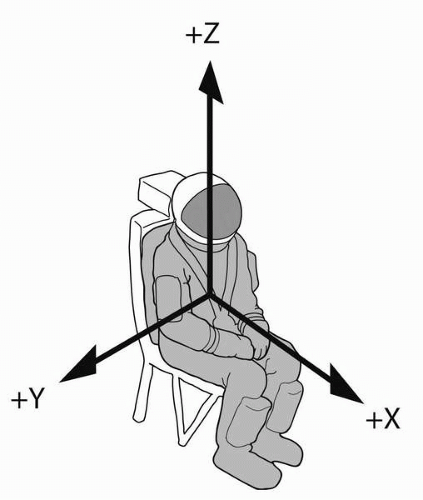
Sustained acceleration occurs during normal and aerobatic flight. Because most aircraft maneuvers (such as pitch and banked turns) expose seated occupants to predominantly +G
z, the effects of
+Gz on humans has received most of research attention. Negative-G
z has received much less attention, most of it during and shortly after World War II. G
x and zero-G are most relevant to space flight. G
y has only begun to receive research attention with the development of vectored thrust fighters.
Relevant Mechanics
Humans respond physiologically to G. When an aircraft follows a curving path, the velocity changes continuously along the curve (being a vector, although speed may remain constant) and the aircraft experiences acceleration. The acceleration of the aircraft depends on the velocity of the aircraft and the radius of the turn. This is expressed as:
where v = velocity, r = radius of the turn.
If the aircraft occupants are “fixed” to the aircraft, they experience the same acceleration, which is expressed as:
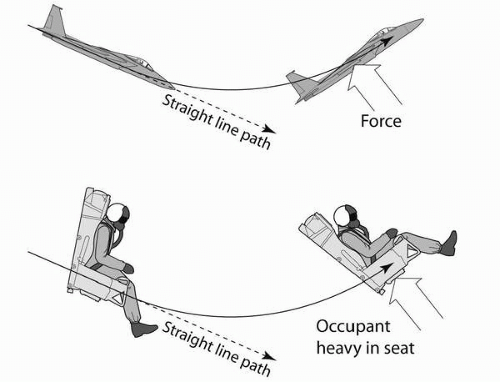
When an occupant experiences +G
z, the associated force is felt as increasing pressure of the buttocks against the surface of the seat. The occupant experiences “heaviness,” and activities, such as lifting an arm, will be more difficult. When relative
−Gz is experienced, there is a reduction in pressure on the buttocks and the occupant may feel a rise off the seat. As
−Gz increases, pressure of the shoulder and lap restraints is experienced. Ultimately, the occupant may feel suspended by the shoulders and have the sensation of being inverted.
Some aircraft, including civilian aerobatic and military aircraft, are capable of executing large pitch changes at relatively high velocities and can therefore generate high Gz. The magnitude and duration of Gz that an aircraft generates depends on its structural strength and thrust.
Incidentally,
Equation 3 can be used to calculate orbital velocity. In stable circular orbit, the acceleration of gravity is equal and opposite to the acceleration due to radius of turn. With a low-Earth orbital radius of 6,700
km, it is easy to show that the turn velocity necessary to create 1 G in opposition to the 1 G of gravity is approximately 8
km/s, which is the low-Earth orbital velocity previously mentioned. This orbital balance of acceleration vectors is a special and important case of weightlessness. Both the freefall concept and the acceleration balance concept are useful and correct in understanding orbital weightlessness.
The Fluid Model
When force is applied to fluid in a constrained volume, the pressure within increases. Pressure is a measure of force (per unit area) transmitted by fluids. For example, squeezing a filled plastic water bottle increases the pressure of the water inside the bottle. If the top is off, the increased water pressure compels the water to squirt out against the constraint of gravity and the resistance of the opening. Similarly, heart contraction during systole increases the pressure within the left ventricle and compels high-pressure blood to open the aortic valve and flow into the aorta.
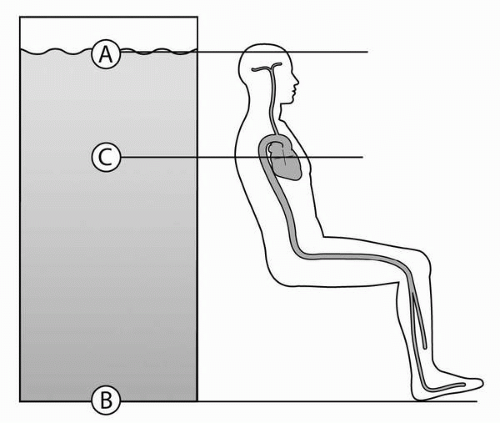
On Earth, the force acting on a fluid at any depth varies with the weight of the fluid above, a principle of hydrostatics. Therefore, pressure increases with increased depth, a fact well known to divers. Referring to the depiction of the column of fluid in
Figure 4-6, we expect the pressure of fluid to be less at point A than at point B because there is no fluid
above point A. Because fluids are freely mobile, and have no internal rigid structure, pressure is transmitted within the fluid according to Pascal’s principle (which states that a change in pressure at any point in a fluid is transmitted to every part of the fluid).
Hydrostatic principles apply to all fluids in the body, including the pericardial, pleural, abdominal, and cerebrospinal fluids, and both venous and arterial vascular systems. To the right of the water column in
Figure 4-6, we present a seated upright human, and depict the continuous fluid column (cardiovascular system) that extends from the scalp to the feet. Ignoring any pressure generated by the heart, and considering only the hydrostatic pressure of the fluid column, blood pressure at level A is zero, because there is almost no blood above. Blood pressure at the feet (level B) is greatest and equal to the weight of the fluid above. At level C, blood pressure measured at the heart, is intermediate. This component of blood pressure is termed the
hydrostatic pressure component.
Pressure due to contraction of the heart adds to the hydrostatic component of blood pressure. If we consider left ventricular contraction during systole, the force applied to the contained blood by cardiac muscle increases intraventricular blood pressure until the aortic valve opens. The increased blood pressure is then transmitted to the aorta and into the arterial system according to Pascal’s principle. This component of blood pressure is termed the dynamic pressure component.
Total blood pressure is the sum of the dynamic and hydrostatic pressures. The measured systolic blood pressure at the heart level of a young healthy adult is typically approximately 120
mm Hg and is the sum of the two blood pressure components. Measurements taken at other vertical locations (e.g., the ankle) will be different.
Numerical estimates of hydrostatic blood pressure can be made using
Equation 5, which states:
where p = hydrostatic pressure, ρ = blood fluid density, z = vertical depth of fluid.
For a specific gravity of blood of 1.06, and after converting the units of
p from Pascals to millimeters of mercury (
mm Hg),
Equation 5 becomes:
where
p is in
mm Hg, and z is in cm.
Equation 6 can be used to estimate the hydrostatic component of blood pressure at different vertical fluid column depths on Earth (+1 G
z). For example, if the vertical distance from the aortic valve to the top of the head is 38 cm,
Equation 6 predicts that the hydrostatic pressure at the aortic valve in an upright person is approximately 30
mm Hg (0.78 × 38).
As G increases, the apparent weight (force) of any object increases directly, and this applies equally to fluids. Under increased G,
Equation 6 becomes:
Equation 7 can be used to predict G-tolerance, if physiological compensation is not considered. For example, an individual with a vertical fluid distance of 38 cm from the aortic valve to near the top of the head, and having a systolic blood pressure
at the aortic valve of 120
mm Hg, would be expected to have zero systolic blood flow near the vertex at approximately +4 G
z [
Equation 7: 120
mm Hg = 0.78(
38)(4.0)]. This is a point above which the dynamic systolic blood pressure is unable to oppose the hydrostatic component of the blood. Consequently blood flow to the upper brain would cease.
Equation 7 can also be used to estimate blood pressures at other locations.
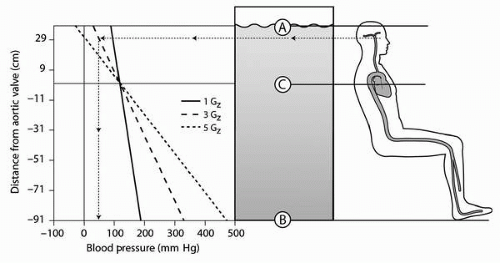
Figure 4-7 shows the person seated upright as depicted previously in
Figure 4-6. To the left of the human figure are plots of systolic blood pressures versus distance from the aortic valve based on
Equations 6 and
7. There are three plots depicted: +1 G
z, +3 G
z, and +5 G
z, and they are based on the approximate dimensions of a 50% average male. Any estimates, using this simple model, will vary with individuals of different sizes. Note the very high blood pressures in the lower extremities at +5 G
z. Similarly, pressures at head level are predicted to be less than atmospheric pressure at +5 G
z. Once again, the underlying assumption is a heart-level systolic blood pressure of 120
mm Hg.
Equation 7 can be used for other postural orientations such as reclined or inverted.
Figure 4-8A depicts the expected blood pressures for a seated reclined individual. Because of the reclined posture, the vertical heart-to-brain distance is decreased, and the hydrostatic blood pressure component is less. Positive-G
z tolerance is predictably
increased.
Figure 4-8B demonstrates the effect of inversion, and also the very high head-level blood pressures that can be experienced during −G
z.
These predictions agree well with human studies that show a head-level reduction of blood pressure of approximately 30
mm Hg per change of each 1 G (
4).
Blood pressure at the head is further lowered if circulating blood volume is reduced. When blood pressure increases during increased +G
z, as it does in the lower (dependent) areas of the body (
Figure 4-7), stretching of tissues occurs. As a result of stretching of tissues in the abdomen and lower extremities, a portion of the circulating blood volume becomes unavailable for circulation.
Individual variations in heart-to-brain distances, and differences in blood pressures at the aortic valve, will change these predictions. Therefore, people with smaller vertical dimensions when upright will have an advantage tolerating
+Gz when compared to taller people. Elevation of blood pressure at the aortic valve would predictably increase
+Gz tolerance.
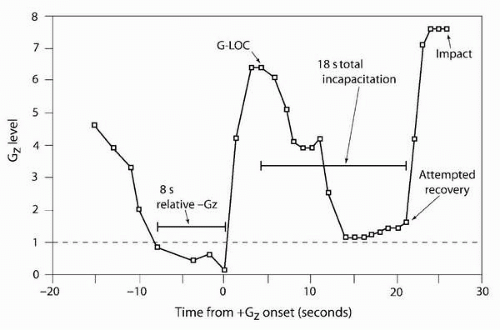
Human Tolerance to Sustained +Gz
Human tolerance to
+Gz has been studied on ground-based centrifuges using human volunteers. Objective measures of tolerance in the past have included ear pulse opacity, direct and indirect measures of blood pressure, and loss of consciousness. A less objective, but more widely used measure, consists of subject reports of visual changes. Unfortunately, reporting is variable and may be influenced by psychological or social pressures, anatomy, and slowed mental processing.
Human tolerance to
+Gz is influenced by many variables, including anthropometry (heart-to-brain distance), muscle straining, anti-G suit inflation, and rate of
+Gz onset. To control against some of these factors, standardized
approaches have been developed. One is to determine the tolerance of relaxed subjects. This allows for
+Gz tolerance to be reported without the confounding influences of muscle strain or anti-G suit inflation, and offers a means of determining passive psychophysiological compensatory responses. Slower G-onset levels allow for cardiovascular compensation to influence the measure. Faster G-onset levels measure tolerance before a full cardiovascular response occurs.
In general, two separate types of subject tests are used, as defined by G-onset rate: (i) rapid-onset rate (
ROR) tests and (ii) gradual-onset rate (
GOR) tests.
ROR is defined as a rate greater than 0.33 G/s, often as high as 6 G/s.
GOR is defined as slower than 0.25 G/s. Measurements of relaxed
ROR +Gz tolerance are approximately 1 G lower than
GOR tolerances. The results of a study involving 1,000 relaxed male subjects reported tolerances presented in
Table 4-2A (
16). The results of World War II era centrifuge studies, based on subjective reports with onset rates of 2 G/s, are also presented in
Table 4-2B (
17).
Researchers have studied other potential influences on human tolerance to +G
z. Studies assessing female relaxed tolerance to
+Gz concluded that they are equivalent to males, with reported
ROR tolerances of 4.2 ± 0.5 G and
GOR tolerances of 5.2 ± 0.6 G (
18). Female time-to-fatigue during simulated air combat maneuvers is not significantly different from that for males (
19,
20). Menstruation in women on oral contraception has no effect on
+Gz tolerance (
19). Motion sickness lowers
+Gz tolerance (
21).
Relative Negative Vertical Acceleration and Negative Acceleration (−Gz)
In response to increased relative −G
z, heart rate is reduced and generalized vasodilatation occurs, a response that is relatively rapid. This response is dose related in the sense that increased relative −G
z, moving toward zero-G and then −G
z, results in increasing blood pressure in the upper body and a more vigorous parasympathetic response (
10).
During −G
z, intracerebral blood pressure increases. Congestion of the face and a subjective sensation of eye bulging occurs; this can become intense with increasing −G
z. There is upward movement of the abdominal contents and
the work of breathing is increased. Inverted flight (−1 G
z) can be unpleasant, but tolerable. Between −2 and −3 G
z, there is severe facial congestion and occasional reddening of vision. Most subjects can tolerate −3 G
z for 5 seconds, although some can reach −5 G
z without injury (
10,
22). The feeling of facial congestion becomes intense at −3 to −4.5 G
z. The restraints, which are supporting the entire mass of the body, cause additional painful sensations. Competitive aerobatic pilots describe sustaining up to −9 G
z for very brief durations.
Some of the adverse effects of
−Gz derive from increased arterial blood pressure in the head, especially where it is unopposed. Within the skull, where increased arterial pressures are balanced by increased pressures in the surrounding cerebrospinal fluid, adverse effects are generally not seen (
23). Where increased pressures are unopposed, injury can occur. Facial petechiae have been described by competitive airshow pilots. Nose bleeds and subconjunctival hemorrhage have been reported due to high −G
z.
There are no generally accepted countermeasures to −G
z, although some aerobatic pilots report that they relax while exposed to
−Gz so as not to further increase thoracic pressure.