In this article hereditary genodermatoses with cancer predisposition are reviewed, including nevoid basal cell carcinoma syndrome, neurofibromatosis types 1 and 2, tuberous sclerosis complex, xeroderma pigmentosum, and dyskeratosis congenita. Hereditary melanoma is also included, though it differs from the others in several respects. The underlying genetic aberrations causing these syndromes are largely known, allowing novel treatments to be developed for some of these disorders. Early recognition and diagnosis allows for close follow-up and surveillance for associated malignancies.
Nevoid basal cell carcinoma syndrome (Gorlin syndrome)
History and Overview
A relationship between multiple basal cell carcinomas and developmental defects was suggested by Binkley and Johnson in 1951 and Howell and Caro in 1959, but it was Gorlin and Goltz who, in 1960, first described a distinct syndrome consisting of the presence of multiple nevoid basal cell epitheliomas, jaw cysts, and bifid ribs. Nevoid basal cell carcinoma syndrome (NBCCS), or Gorlin syndrome, is a rare condition, with an estimated prevalence of 1 per 40,000 to 57,000, though the figure may be higher. Two major features characterize the phenotype of NBCCS: developmental abnormalities and multiple neoplasms. Developmental abnormalities include palmar and plantar pits, coarse facies with frontal bossing, cleft palate, strabismus, corpus callosum dysgenesis, falx cerebri calcification, spina bifida occulta, bifid ribs, mesenteric cysts, macrocephaly, and polydactyly. Neoplasms include basal cell carcinomas (BCCs), medulloblastomas, rhabdomyosarcomas, odontogenic keratocysts, fibrosarcomas, meningiomas, and ovarian fibromas, among other benign and malignant neoplasms. In a study of 105 individuals with NBCCS, mostly from multiple case families, palmar pits, jaw cysts, BCCs, and calcification of the falx cerebri were present in more than 50% of cases, and bifid ribs were present in 42% of cases. Clinical studies have led to revisions of the diagnostic criteria over time. Diagnosis of NBCCS may be made by the presence of 2 major and 1 minor or 1 major and 3 minor criteria. Major criteria include: (1) lamellar calcification of the falx cerebri in persons younger than 20 years, (2) histologically confirmed odontogenic (jaw) keratocyst, (3) 2 or more palmar/plantar pits, (4) greater than 5 BCCs in a lifetime or a BCC before age 30 years, and (5) a first-degree relative with NBCCS. Minor criteria include: (1) childhood medulloblastoma, (2) lymphomesenteric or pleural cysts, (3) macrocephaly, (4) cleft lip/palate, (5) vertebral/rib anomalies including bifid vertebrae/ribs, extra ribs, and/or splayed ribs, (6) polydactyly, (7) ovarian/cardiac fibromas, and (8) ocular abnormalities including cataracts. Of note, making the diagnosis may be difficult in African Americans because those affected with NBCCS have fewer BCCs than their Caucasian counterparts.
Genetics
Chromosomal mapping and genetic studies elucidated the role of inactivating mutations in the human homologue of Drosophila Patched gene ( PTCH1 ) on chromosome 9q22.3 as the cause of almost all cases of NBCCS. Approximately 70% of germline PTCH1 mutations are rearrangements leading to formation of a truncated protein, although deletions, insertions, splice site alterations, nonsense and missense mutations of PTCH1 are also reported. About 6% of mutations are whole gene deletions. Mutations in PTCH1 are inherited in an autosomal dominant manner, and although penetrance is nearly complete, phenotypic expression of the syndrome is widely variable. This phenotypic variation does not appear to be related to the type of PTCH1 mutation present. PTCH1 inactivation has been proposed to occur in 2 steps—the first “hit” occurs in the germline and the second, postnatally. Heterozygosity for PTCH1 due to the inherited germline mutation is likely to give rise to the developmental abnormalities seen in NBCCS. Subsequent postnatal loss of the normal Patched allele by mutation or silencing may lead to multiple BCCs and other neoplasms. Thus, PTCH1 acts as a tumor suppressor. Reports of segmental cases of NBCCS, hypothesized to be caused by postzygotic mutations, are rare. A few cases of NBCCS are caused by mutations in PTCH2 on chromosome 1p32, which is also a tumor suppressor, and suppressor of fused ( SUFU ) on chromosome 10q24-q25.
PTCH1 , PTCH2 , and SUFU are components of the Hedgehog (Hh) signaling pathway, which was first elucidated in Drosophila . Two transmembrane proteins—Patched and Smoothened—transduce the secreted Hh protein signal. In the absence of Hh, Patched catalytically inhibits Smoothened. Secreted Hh binds to Patched, releasing inhibition of Smoothened and effecting downstream events including cell cycle regulation via the transcription factor Ci and a complex of cytoplasmic proteins including Fused (Fu), Suppressor of Fused (Su(fu)), and Costal-2 (Cos2). In this model, Patched inactivation or the constitutive activity of Smoothened leads to overactivity of the Hh pathway resulting in neoplasm formation, though the mechanism connecting pathway overactivity and tumor formation is not yet defined. Not surprisingly, PTCH1 , Smoothened ( SMO ), and SUFU mutations have been identified in sporadic BCCs, medulloblastomas, and odontogenic keratocysts, further implicating the role of the Hh signaling pathway in the development of these tumors.
Genetic Testing and Treatment
Molecular genetic testing can confirm the diagnosis in individuals when the diagnosis is clinically considered. Prenatal diagnosis of NBCCS is possible, though knowledge of the disease-causing mutation in a given family is required.
There are many current treatments for BCCs such as surgical excision and topical immunomodulation. However, the application of these traditional treatments to the BCCs that occur in NBCCS is problematic because of the multiplicity and recurrent nature of the tumors. Photodynamic therapy is emerging as a promising treatment for BCCs in patients with NBCCS. A recent trial with oral nonsteroidal anti-inflammatory drugs in patients with NBCCS with less severe disease showed significantly reduced numbers of BCC in the treated as compared with the placebo group. Because BCCs arise in NBCCS as a result of overactivation of the Hh pathway, novel therapies inhibiting this pathway might be expected to suppress tumor growth. Cyclopamine, a Hh pathway antagonist, inhibited growth of medulloblastomas in a mouse model of NBCCS. In recent clinical trials, the effects of Hh inhibitors were studied in 1 patient with sporadic metastatic medulloblastoma and 33 patients with locally advanced or metastatic BCC, one of whom had NBCCS. Rapid reductions of tumor size and associated symptoms were noted in the patient with metastatic medulloblastoma. Eighteen of 33 patients with locally advanced or metastatic BCC had a partial or complete response, and 11 had stable disease. These studies are promising; however, further research is needed to guide recommendations for use of these Hh inhibitors in individuals with NBCCS.
Neurofibromatosis type 1
History and Overview
Neurofibromatosis type 1 (NF1), first described by von Recklinghausen in 1882, occurs in approximately 1 in 3500 individuals. NF1 is characterized by a combination of cutaneous, neurologic, skeletal, and ocular findings, including benign and malignant tumors primarily of the nerve sheath. To date, the National Institutes of Health (NIH) diagnostic criteria for NF1 includes at least 2 of the following features: (1) 6 or more café-au-lait macules (with largest diameter >0.5 cm in prepubertal individuals or >1.5 cm in postpubertal individuals), (2) axillary or inguinal freckling (Crowe sign), (3) 2 or more neurofibromas of any type or at least 1 plexiform neurofibroma, (4) 2 or more iris hamartomas (Lisch nodules), (5) a distinctive bony lesion, such as sphenoid wing dysplasia or long bone cortical thinning with or without pseudoarthrosis, and (6) a first-degree relative with NF1. The majority of individuals can be diagnosed by age 3 years.
Café-au-lait macules are the most common feature of NF1, occurring in 95% of individuals and typically appearing by age 3 years. Other cutaneous manifestations include axillary and/or inguinal freckling, present in most children; xanthogranulomas, observed in early childhood and possibly associated with chronic myeloid leukemia in children; and diffuse hyperpigmentation. Neurofibromas, benign nerve sheath tumors arising from Schwann cells, are a hallmark finding of NF1, though their numbers vary across affected patients. Dermal, spinal, and plexiform neurofibromas may occur in NF1. The number of neurofibromas varies among patients with NF1. Spinal neurofibromas may cause nerve compression. Dermal and plexiform neurofibromas can lead to significant cosmetic deformity; additionally, plexiform neurofibromas may develop into malignant peripheral nerve sheath tumors (MPNST), which may metastasize extensively and be fatal. The lifetime risk for development of MPNST is 10%. Additional neurologic findings include optic pathway gliomas, cognitive deficits including learning disabilities, and epilepsy. Optic pathway gliomas are low-grade pilocytic astrocytomas capable of involving the optic nerve, chiasm, tract, and/or hypothalamus, which may cause visual loss and/or endocrine dysregulation. Vascular abnormalities cause significant mortality and include severe hypertension, usually secondary to renal artery stenosis; cerebrovascular disease, possibly leading to cerebral hemorrhage; and pulmonary arterial hypertension. Skeletal abnormalities associated with significant morbidity include scoliosis, pseudoarthroses, sphenoid wing dysplasia, macrocephaly, and short stature. Additional malignancies that may occur in patients with NF1 include pheochromocytoma, pancreatic endocrine tumors, rhabdomyosarcomas, and duodenal somatostatinomas. Glomus tumors were also recently associated with NF1.
Genetics
NF1 is caused by an approximately equal number of spontaneous and autosomal dominantly inherited germline mutations in the NF1 gene, located on chromosome 17q11.2, encoding neurofibromin, a tumor suppressor predominantly expressed in neural crest cells including neurons, Schwann cells, and early melanocytes. Similar to BCCs in Gorlin syndrome, neurofibromas are thought to arise after a “second hit” to NF1 , leading to loss of heterozygosity. Neurofibromin regulates Ras guanosine triphosphatase activity by converting Ras into its inactive form and suppressing cell growth. In NF1, the Ras/Raf/ERK signaling pathway is unchecked, leading to unregulated cell proliferation. One important protein activated by Ras is the mammalian target of rapamycin (mTOR) protein. Of interest is that another protein in this signaling pathway, SPRED1, inhibits the Raf protein, and mutations in SPRED1 account for an NF1-like syndrome consisting of multiple café-au-lait macules, axillary freckling, and macrocephaly.
In individuals with NF1, there is complete penetrance by age 20 years, although there is variable phenotypic expression. Even among individuals from the same family sharing the same mutation, phenotypes can differ substantially. Partial and complete gene deletions, insertions, nonsense, frameshift, and splice mutations as well as amino acid substitutions and chromosomal rearrangements affecting the NF1 gene may cause NF1. Of note, NF1 can be manifested by somatic mosaicism due to mutations in the NF1 gene that occur postzygotically during development.
Genetic Testing and Treatment
A comprehensive genetic screening test identified mutations in more than 95% of subjects who fulfilled the NIH diagnostic criteria. Genetic testing is indicated for prenatal testing, preimplantation genetic diagnosis, and for confirmation in individuals with suspected NF1 who do not meet the full diagnostic criteria. One caveat of genetic testing, however, is that in most cases the disease phenotype cannot be predicted by the genotype. Exceptions are for patients with complete deletions of the NF1 gene and a 3–base-pair inframe deletion in exon 17, which do result in predictable phenotypes. Complete deletions are associated with a severe NF1 phenotype including numerous neurofibromas, significant cognitive deficits, dysmorphic facies, and an elevated risk of MPNST development. The 3–base-pair inframe deletion is associated with a mild phenotype, including even the absence of cutaneous neurofibromas.
Affected individuals should be followed annually with physical examinations, including fundoscopy at least until age 7 years, with assessment and workup of symptoms that may indicate MPNST development; routine imaging in asymptomatic individuals is not recommended. Thalidomide and a vascular endothelial growth factor receptor (VEGFR) inhibitor, both angiogenesis inhibitors, are being tested to treat MPNSTs and plexiform neurofibromas, because both tumors require intact vascular supplies. Novel treatments for NF1 are emerging from advances in understanding the functional consequences of the genetic mutations, specifically altering the Ras/Raf/ERK signaling pathway. Ras inhibitors, for example, are postulated to inhibit the pathway, and in this manner substitute for neurofibromin. Tipifarnib, a farnesyltransferase inhibitor that targets Ras, is currently being investigated for treatment in NF1 patients with plexiform neurofibromas. Rapamycin, though primarily used for its immunosuppressive properties, is now being considered for use in NF1 patients because it, like neurofibromin, inhibits mTOR signaling and may substitute for NF1 in this way.
Neurofibromatosis type 1
History and Overview
Neurofibromatosis type 1 (NF1), first described by von Recklinghausen in 1882, occurs in approximately 1 in 3500 individuals. NF1 is characterized by a combination of cutaneous, neurologic, skeletal, and ocular findings, including benign and malignant tumors primarily of the nerve sheath. To date, the National Institutes of Health (NIH) diagnostic criteria for NF1 includes at least 2 of the following features: (1) 6 or more café-au-lait macules (with largest diameter >0.5 cm in prepubertal individuals or >1.5 cm in postpubertal individuals), (2) axillary or inguinal freckling (Crowe sign), (3) 2 or more neurofibromas of any type or at least 1 plexiform neurofibroma, (4) 2 or more iris hamartomas (Lisch nodules), (5) a distinctive bony lesion, such as sphenoid wing dysplasia or long bone cortical thinning with or without pseudoarthrosis, and (6) a first-degree relative with NF1. The majority of individuals can be diagnosed by age 3 years.
Café-au-lait macules are the most common feature of NF1, occurring in 95% of individuals and typically appearing by age 3 years. Other cutaneous manifestations include axillary and/or inguinal freckling, present in most children; xanthogranulomas, observed in early childhood and possibly associated with chronic myeloid leukemia in children; and diffuse hyperpigmentation. Neurofibromas, benign nerve sheath tumors arising from Schwann cells, are a hallmark finding of NF1, though their numbers vary across affected patients. Dermal, spinal, and plexiform neurofibromas may occur in NF1. The number of neurofibromas varies among patients with NF1. Spinal neurofibromas may cause nerve compression. Dermal and plexiform neurofibromas can lead to significant cosmetic deformity; additionally, plexiform neurofibromas may develop into malignant peripheral nerve sheath tumors (MPNST), which may metastasize extensively and be fatal. The lifetime risk for development of MPNST is 10%. Additional neurologic findings include optic pathway gliomas, cognitive deficits including learning disabilities, and epilepsy. Optic pathway gliomas are low-grade pilocytic astrocytomas capable of involving the optic nerve, chiasm, tract, and/or hypothalamus, which may cause visual loss and/or endocrine dysregulation. Vascular abnormalities cause significant mortality and include severe hypertension, usually secondary to renal artery stenosis; cerebrovascular disease, possibly leading to cerebral hemorrhage; and pulmonary arterial hypertension. Skeletal abnormalities associated with significant morbidity include scoliosis, pseudoarthroses, sphenoid wing dysplasia, macrocephaly, and short stature. Additional malignancies that may occur in patients with NF1 include pheochromocytoma, pancreatic endocrine tumors, rhabdomyosarcomas, and duodenal somatostatinomas. Glomus tumors were also recently associated with NF1.
Genetics
NF1 is caused by an approximately equal number of spontaneous and autosomal dominantly inherited germline mutations in the NF1 gene, located on chromosome 17q11.2, encoding neurofibromin, a tumor suppressor predominantly expressed in neural crest cells including neurons, Schwann cells, and early melanocytes. Similar to BCCs in Gorlin syndrome, neurofibromas are thought to arise after a “second hit” to NF1 , leading to loss of heterozygosity. Neurofibromin regulates Ras guanosine triphosphatase activity by converting Ras into its inactive form and suppressing cell growth. In NF1, the Ras/Raf/ERK signaling pathway is unchecked, leading to unregulated cell proliferation. One important protein activated by Ras is the mammalian target of rapamycin (mTOR) protein. Of interest is that another protein in this signaling pathway, SPRED1, inhibits the Raf protein, and mutations in SPRED1 account for an NF1-like syndrome consisting of multiple café-au-lait macules, axillary freckling, and macrocephaly.
In individuals with NF1, there is complete penetrance by age 20 years, although there is variable phenotypic expression. Even among individuals from the same family sharing the same mutation, phenotypes can differ substantially. Partial and complete gene deletions, insertions, nonsense, frameshift, and splice mutations as well as amino acid substitutions and chromosomal rearrangements affecting the NF1 gene may cause NF1. Of note, NF1 can be manifested by somatic mosaicism due to mutations in the NF1 gene that occur postzygotically during development.
Genetic Testing and Treatment
A comprehensive genetic screening test identified mutations in more than 95% of subjects who fulfilled the NIH diagnostic criteria. Genetic testing is indicated for prenatal testing, preimplantation genetic diagnosis, and for confirmation in individuals with suspected NF1 who do not meet the full diagnostic criteria. One caveat of genetic testing, however, is that in most cases the disease phenotype cannot be predicted by the genotype. Exceptions are for patients with complete deletions of the NF1 gene and a 3–base-pair inframe deletion in exon 17, which do result in predictable phenotypes. Complete deletions are associated with a severe NF1 phenotype including numerous neurofibromas, significant cognitive deficits, dysmorphic facies, and an elevated risk of MPNST development. The 3–base-pair inframe deletion is associated with a mild phenotype, including even the absence of cutaneous neurofibromas.
Affected individuals should be followed annually with physical examinations, including fundoscopy at least until age 7 years, with assessment and workup of symptoms that may indicate MPNST development; routine imaging in asymptomatic individuals is not recommended. Thalidomide and a vascular endothelial growth factor receptor (VEGFR) inhibitor, both angiogenesis inhibitors, are being tested to treat MPNSTs and plexiform neurofibromas, because both tumors require intact vascular supplies. Novel treatments for NF1 are emerging from advances in understanding the functional consequences of the genetic mutations, specifically altering the Ras/Raf/ERK signaling pathway. Ras inhibitors, for example, are postulated to inhibit the pathway, and in this manner substitute for neurofibromin. Tipifarnib, a farnesyltransferase inhibitor that targets Ras, is currently being investigated for treatment in NF1 patients with plexiform neurofibromas. Rapamycin, though primarily used for its immunosuppressive properties, is now being considered for use in NF1 patients because it, like neurofibromin, inhibits mTOR signaling and may substitute for NF1 in this way.
Neurofibromatosis type 2
History and Overview
Neurofibromatosis type 2 (NF2), like NF1, is a neurocutaneous disorder. Although NF2 shares some features with NF1, they are distinct syndromes with many differences firmly distinguished in 1987, with the discovery that the gene causing NF1 mapped to chromosome 17q whereas tumor DNA from individuals with NF2 showed loss of heterozygosity for markers on chromosome 22q. First described in 1822, NF2 is rare, affecting 1 in 25,000 individuals. Bilateral vestibular schwannomas are the most frequent clinical feature, present in up to 95% of cases. According to the most commonly used Manchester diagnostic criteria, NF2 can be diagnosed by this feature alone. NF2, however, is a multiple neoplasia syndrome, and other tumors affecting the nervous system, skin, and eyes also occur. Diagnostic criteria, in addition to bilateral vestibular schwannomas, include: (1) a family history of NF2 and a unilateral vestibular schwannoma or 2 NF2-associated nervous system tumors or cataracts, (2) a unilateral vestibular schwannoma and 2 NF2-associated nervous system tumors or cataracts, or (3) multiple meningiomas and a unilateral vestibular schwannoma or 2 other NF2-associated nervous system tumors or cataracts. Nervous system tumors include schwannomas developing in cranial nerves other than 8, spinal nerves, and peripheral nerves; meningiomas, ependymomas, pilocytic astrocytomas, and occasionally, neurofibromas as in NF1. Bilateral hearing loss, secondary to vestibular schwannomas, is common. Peripheral neuropathy, though not one of the diagnostic criteria for NF2, can develop in affected individuals, both in association with and independent of nerve-compressing tumors. The most common ocular finding is early cataracts, which may lead to loss of vision. Other ocular manifestations include epiretinal membranes and retinal hamartomas. Cutaneous findings include rough, slightly hyperpigmented plaques with overlying hypertrichosis as well as subcutaneous and intradermal tumors, typically schwannomas, although as previously mentioned, neurofibromas may occur. Café-au-lait macules, typical of NF1, may be seen in NF2 as well, though in one series no patient had more than 6.
Genetics
NF2 is caused by mutations in the tumor suppressor NF2 gene on chromosome 22q12. The NF2 protein (named merlin or alternatively schwannomin) normally regulates mitogenic intracellular pathways including the phosphoinositide-3-kinase (PI3K) signaling pathway, which includes Akt and mTOR, and the mitogen-activated protein kinase (MAPK) signaling pathway, which includes Ras/Raf/MEK/ERK. Inherited in an autosomal dominant fashion, NF2 has nearly complete penetrance by age 60 years. Age of onset is typically around 18 years. Affected individuals in the same family usually share similar phenotypic features, but there is variable expressivity among families, which can largely be attributed to the type of NF2 mutations segregating in each family. Severe disease and a higher mortality are associated with constitutional nonsense or frameshift mutations, which result in a truncated protein, as well as splice-site mutations within exons 1 to 5. Mild disease and a lower mortality are associated with missense mutations and inframe or large deletions as well as splice-site mutations within exons 11 to 15. Fifty percent of NF2 patients have a de novo mutation, and mosaic forms of NF2 occur with high frequency in these patients. Most patients with mosaic forms of NF2 have mild disease or limited involvement; there is also a lower risk of transmission to offspring from individuals with mosaic forms of NF2 because it is likely that less than 50% of germ cells carry the mutation.
Genetic Testing and Treatment
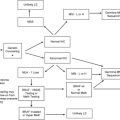
Genetic testing of individuals without symptoms from affected families is recommended and allows for early diagnosis, which can improve clinical care. For asymptomatic individuals with an affected parent, screening guidelines recommend: annual follow-up by an ophthalmologist, neurologist, and audiologist from infancy; head and spinal magnetic resonance imaging (MRI) starting at around age 10 years repeated every 2 to 3 years for spinal MRI; and presymptomatic genetic testing at around age 10 if not performed earlier by request of the parents. For asymptomatic individuals from families with severe disease, MRI and genetic testing are recommended at an earlier age, and MRI may be performed annually.
Treatment for NF2 is directed at early and complete removal of bilateral vestibular schwannomas to preserve hearing. In patients with an intact cochlear nerve following vestibular schwannoma surgery, cochlear implants may improve hearing. Meningiomas are typically managed by neurosurgical intervention. These tumors may or may not be fully resectable, depending on their location in the nervous system; furthermore, resection of meningiomas in some locations, such as the skull base or optic nerve sheath, carries greater risks than other locations, such as the cerebral hemisphere or spinal canal. With close ophthalmologic follow-up, cataracts may be found early and those associated with significant loss of visual acuity extracted. Skin tumors, when symptomatic, may be excised. The use of mTOR inhibitors is currently being investigated for individuals with NF2.
Tuberous sclerosis complex
History and Overview
Similar to NF1 and NF2, tuberous sclerosis complex (TSC) is a neurocutaneous disorder affecting multiple systems. First reported by Bourneville in 1880, TSC was named after the cerebral cortical lesions resembling tubers and the periventricular calcification characteristic of the disorder. Multiple hamartomas, or tumors, can develop in multiple organs, such as the brain, skin, kidney, eye, lung, and liver in TSC patients. The incidence is estimated to be 1 per 6000 live births. Diagnostic criteria for TSC endorsed by the Tuberous Sclerosis Alliance organization include both major and minor categories. The diagnosis is made with 2 major features (excluding lymphangioleiomyomatosis and renal angiomyolipoma alone) or 1 major and 2 minor features. Major diagnostic criteria include: (1) facial angiofibromas (“adenoma sebaceum”) or forehead plaque, (2) nontraumatic ungual or periungual fibroma (“Koenen tumor”), (3) 3 or more hypomelanotic macules (“ash leaf spots” or “Fitzpatrick patches”), (4) connective tissue nevus (“Shagreen patch”), (5) multiple retinal nodular hamartomas, (6) cortical tuber, (7) subependymal nodule, (8) subependymal giant cell astrocytoma, (9) single or multiple cardiac rhabdomyoma, (10) lymphangioleiomyomatosis, and (11) renal angiomyolipoma. Minor criteria include: (1) multiple dental enamel pits, (2) hamartomatous rectal polyps, (3) bone cysts, (4) cerebral white matter radial migration lines, (5) gingival fibromas, (6) nonrenal hamartomas, (7) retinal achromic patch, (8) cutaneous symmetric hypopigmented macules (“confetti” macules), and (9) multiple renal cysts.
Neurologic manifestations are present in approximately 85% of children and adolescents with TSC and include epilepsy, cognitive impairment, behavioral problems, and autism. These neurologic problems are the primary cause of morbidity and mortality in affected individuals, and are likely caused by the presence of brain lesions including cortical tubers, subependymal nodules, subependymal giant cell tumors, and white matter abnormalities. In familial cases of TSC, nodules have a high likelihood of transforming into an ependymal giant cell tumor, with a prevalence of about 11% in affected individuals. Epilepsy, caused by diminished γ-aminobutyric acid (GABA) neuronal inhibition, typically starts in the first few months of life and affects 90% to 96% of TSC patients. Control of seizures is necessary to reduce the risk of cognitive impairment. Mental retardation (MR) is seen in up to 50% of affected individuals, almost all of whom have seizures; however, not all patients with seizures have MR.
After neurologic complications, those from renal involvement are the major contributors to mortality in TSC. Angiomyolipomas, the most common renal abnormality, affect about 80% of individuals with TSC, increase in incidence with age, and are usually treated with embolization or renal-sparing surgery if necessary. Angiomyolipomas are typically bilateral and may be symptomatic, especially in women. Renal cysts and renal cell carcinoma can also occur. Cardiac rhabdomyomas are often the first manifestation of TSC; they are benign, largely asymptomatic tumors that regress with age and rarely require surgery. MRI can diagnose cardiac rhabdomyomas in utero; most of these cases are affected with TSC. Pulmonary involvement is rare in TSC; the most common lesion is lymphangioleiomyomatosis, typically affecting premenopausal adult women. Ocular findings include retinal astrocytic hamartomas (also called “mulberry lesions”), which occur in 40% to 50% of TSC patients and increase with age. Oral involvement includes pitting of dental enamel, occurring in about 50% to 100% of cases, and gingival fibromas, noted mostly on the anterior upper jaw. Surgery may be needed for large gingival lesions.
TSC patients typically have a variety of dermatologic manifestations. Small, confetti-like hypopigmented macules and medium to large hypopigmented patches with an ash leaf, round, or polygonal shape may be observed. The “ash leaf spot” is typically present at birth, and so can help to confirm the diagnosis. Facial angiofibromas, small pink papules, are typically found around the central face, particularly the nasolabial folds, and can be removed with carbon dioxide or other destructive lasers. Fibrous plaques, resembling angiofibromas histologically, are large plaques typically found on the forehead or scalp. Whereas angiofibromas typically appear around age 5 years, fibrous plaques may be present in affected individuals younger than 2 years or even at birth. Many consider angiofibromas and fibrous plaques the same in terms of diagnostic criteria for TSC. Ungual or periungual fibromas, pink papulonodules arising from the nail bed and also resembling angiofibromas histologically, become apparent at puberty and increase in number with age; they affect toenails more commonly than fingernails and may be symptomatic, requiring surgery. Connective tissue nevi, or Shagreen patches, can be found on the trunk, especially the lumbosacral region, and may also increase in size with age. Café-au-lait macules may also occur in up to 30% of TSC patients, although their frequency in TSC patients compared with unaffected individuals is the same. Molluscum fibrosum pendulum, pedunculated skin-colored papules, may also develop.
Genetics
TSC is caused by autosomal dominantly inherited and sporadic mutations in 2 genes: TSC1 , located on chromosome 9q34, encoding tuberin, and TSC2 , located on chromosome 16p13.3, encoding hamartin. Tuberin and hamartin proteins bind tightly to form a heterodimer with tumor suppressor properties including regulation of cell growth by inhibiting mTOR via the Rheb (Ras homologue enriched in brain) protein. Studies in Drosophila have exposed the role of the tuberin and hamartin genes downstream of the insulin receptor in regulation of cell size.
TSC exhibits complete penetrance with wide phenotypic variability, even within families sharing the same mutation. In TSC, germline mosaicism is possible. In large, multigeneration TSC families, TSC1 and TSC2 gene mutations occur in a 1:1 ratio; however, TSC2 mutations account for the majority of sporadic cases, apparently because of an increased rate of second-hit events. TSC1 mutations are generally small deletions and insertions as well as nonsense mutations, whereas TSC2 mutations can include these as well as large deletions and rearrangements. Phenotype severity generally cannot be predicted by the type and location of the mutation, although some missense mutations in TSC2 are associated with a mild phenotype. Of note, large deletions of TSC2 can also result in deletions of the nearby gene responsible for polycystic kidney disease, PDK1 , resulting in individuals with TSC and multiple renal cysts in infancy. Disease phenotype has been found to differ among TSC patients with TSC1 versus TSC2 mutations; individuals with TSC2 mutations have a similar but more severe phenotype, including more severe mental retardation and increased numbers of cortical tubers, retinal hamartomas, and facial angiofibromas, than those with TSC1 mutations.
Genetic Testing and Treatment
DNA testing can be performed to confirm a diagnosis as well as for prenatal diagnosis. Identification of affected individuals before or at birth, or during infancy allows for prompt diagnostic evaluation with neuroimaging studies, cardiac evaluation, and renal ultrasonography as well as early intervention with seizure-controlling medications, reducing the potential for intellectual impairment. When TSC-associated seizures are intractable despite standard antiepileptic medication, vigabatrin (γ-vinyl-γ-aminobutyric acid), a selective GABA-transaminase inhibitor, may be used to reduce infantile spasms; however, this medication is not available in the United States. TSC patients should be managed by a team of physicians, including neurologists, dermatologists, urologists, pediatricians, and geneticists.
Because mTOR is unregulated in TSC as in NF1, rapamycin may play a role in the treatment of TSC-related tumors. Studies in animal models demonstrate that rapamycin and other mTOR inhibitors are effective treatments for renal tumors, liver hemangiomas, epilepsy, and cutaneous tumors. In human studies, rapamycin decreases the volume of renal angiomyolipomas and subependymal giant cell astrocytomas. Further studies are needed to evaluate this promising therapy for individuals affected with TSC.
Xeroderma pigmentosum
History and Overview
Xeroderma pigmentosum (XP) is characterized by severe ultraviolet (UV) light photosensitivity and a greater than 1000-fold increase in frequency of squamous cell carcinoma, basal cell carcinoma, and melanoma. Sun sensitivity and freckling are typically seen by 2 years of age. Skin cancers can develop in the first decade of life, with the majority occurring on the head, neck, or face. In addition to cutaneous findings, patients often have ocular abnormalities including ectropion, corneal opacities, and neoplasms; these may cause blindness. Neurologic abnormalities may also occur, depending on the underlying genetic abnormality. XP patients also have increased risks of other cancers, especially oral cancer, most commonly affecting the anterior tongue.
Genetics
XP is an autosomal recessive disorder caused by mutations in nucleotide excision repair complementation groups, of which there are 7, A to G; there is also an XP-variant type caused by mutations in the DNA polymerase eta gene. XP variant type is characterized by photosensitivity, skin cancers, and absence of neurologic abnormalities. The complementation groups and DNA polymerase function in DNA repair, particularly after UV damage. Mutations in XPA and XPC account for approximately 50% of cases of XP. The relationship between defects in these complementation groups and the clinical disease phenotype is complex; whereas mutations in several genes can cause the same phenotype, different mutations in the same gene can cause different phenotypes. For example, some forms of XP are associated with neurologic problems including mental retardation, sensorineural deafness, spasticity, and hyporeflexia due to progressive neuronal degeneration. Furthermore, Cockayne syndrome (CS) and trichothiodystrophy (TTD), other autosomal recessive disorders, are also caused by defects in nucleotide excision repair genes. Although individuals with CS and TTD are photosensitive like XP individuals, they do not have an increased frequency of skin cancers. XP and CS can occur together in the same individual as the XP/CS complex; these individuals often have skin and eye findings of XP with the short stature, immature sexual development, retinopathy, and progressive neurologic degeneration of CS. It is interesting that polymorphisms in the XPD gene are related to early onset of sporadic basal cell carcinoma, suggesting the importance of the NER pathway in BCC development.
Genetic Testing and Treatment
Clinical molecular testing is available for XPA and XPC genes only. Treatment of XP involves early recognition, strict avoidance of UV exposure of the skin and eyes, routine skin examinations for detection followed by complete excision of skin cancers, and neurologic follow-up if needed. High-dose oral isotretinoin has been shown to decrease numbers of skin cancers in individuals with multiple skin cancers, though toxicity limits its use.
Dyskeratosis congenita
History and Overview
Dyskeratosis congenita (DC) is a rare syndrome with an unknown true prevalence, but is thought to affect about 1 in 1 million individuals in North America. DC is characterized by abnormal skin pigmentation, nail dystrophy, oral premalignant leukoplakia, bone marrow failure, and a predisposition to cancer, particularly myelodysplasia, acute myeloid leukemia, and cutaneous squamous cell carcinoma of the head and neck. Other findings include ocular abnormalities such as epiphora, blepharitis, and abnormal eyelashes; hair findings including alopecia and premature graying; dental findings such as periodontal disease, decreased tooth root/crown ratio, and enlarged tooth pulp chambers; microcephaly; short stature; and esophageal stenosis, among others. Approximately 90% of affected individuals develop bone marrow failure by age 30 years, which accounts for the majority of mortality. Age of onset and disease severity can vary among affected individuals, unpredictably, even within the same family.
Genetics
Mutations in 6 genes, TERC (RNA subunit of telomerase), TERT (telomerase reverse transcriptase), DKC1 (dyskerin), NHP2 (nucleolar protein family A, member 2, or NOLA2), NOP10 (nucleolar protein family A, member 3, or NOLA3), and TINF2 (TRF1-interacting nuclear factor 2), encoding telomerase complex components, cause about 50% of cases of DC. The mode of inheritance varies by gene, and X-linked, autosomal recessive, and autosomal dominant inheritance patterns have been described. These mutations uniformly result in short telomeres, which accumulate as cells divide and recruit DNA damage proteins that lead to apoptosis or cellular senescence that can lead to organ failure. Three main types of DC can occur: classic DC, and cryptic and severe variants. Cryptic variants include aplastic anemia, myelodysplasia, paroxysmal nocturnal hemoglobinuria, essential thrombocythemia, and pulmonary fibrosis. Severe variants include Hoyeraal-Hreidarsson syndrome and Revesz syndrome. Because there is marked clinical and genetic heterogeneity of DC, most of these variants were only recognized as being associated with classic DC after their underlying mutations were identified. The link between short telomeres, cellular senescence, and malignancy may be present in sporadic cancers as well as in DC.
Genetic Testing and Treatment
Leukocyte telomere length testing by automated multicolor flow cytometry fluorescence in situ hybridization should be used in individuals with suspected DC; findings of DC include telomeres less than the first percentile for age in 3 to 4 of 6 cell types examined. In these individuals, genetic testing should be considered. Management of DC includes routine screening for malignancies by gynecologists, otolaryngologists, dermatologists, and dentists, and annual pulmonary function testing. Treatment of bone marrow failure and/or leukemia may include hematopoietic stem cell transplant, but there is a higher mortality associated with use in DC than in other bone marrow failure syndromes. Other treatments include androgen therapy.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


