This article provides a short summary of hematological practice in India. It focuses particularly on how the patterns of hematologic practice differ from those of countries in the West with particular respect to genetic hematological diseases and a wide range of malignant disorders of hemopoiesis. It also focuses on the difficulties of control and management of hematological disorders set against a background of a relatively poor country.
Key points
- •
Globally, India contributes significantly to the burden of hematological disorders because of the large population and inadequate resources for diagnosis and management.
- •
Iron deficiency anemia in children is commonly nutritional, whereas in women, menorrhagia and pregnancy contribute significantly. Thalassemia major (TM) and hemophilias are common genetic disorders with increased morbidity, and preventive strategies are required to contain the disorders.
- •
Factor v leiden prevalence in inherited thrombophilias ranges between 3% to 20%, and PT G20210A is absent.
- •
Non hodgkin lymphoma and acute leukemias are common with presentation at 10 years younger median ages for chronic myeloid leukemia, chronic lymphocytic leukemia and multiple myeloma than the west. Limited finances restrict use of standard treatment protocols in the majority.
Introduction
Hematological practice ranges from availability of advanced diagnostic facilities and treatment to unavailability of basic medical services to rural India. Problems include a huge population (1.21 billion in the 15th national census survey www.census2011.co.in ), socioeconomic disparity, minimal coverage of health insurance schemes, and the government’s inability to provide universal health coverage. Therefore India contributes significantly to global disease burden for hematological disorders. Lack of national registries contributes to inaccurate epidemiologic data and nonavailability of micromapping of diseases. Health services are offered nationally as a public (Government of India–Ministry of Health and Family Welfare) and private service; however, most patients have to arrange personal finances for diagnosis and treatment.
Nutritional iron deficiency anemia (IDA) is common in pediatric practice, whereas anemia caused by bleeding disorders and anemia of chronic disorders (ACD) are more common in adults. Nationally, the most common genetic disorder is thalassemia major (TM), and other genetic red cell disorders include sickle cell anemia, glucose-6-phosphate dehydrogenase (G6PD) deficiency, and hereditary spherocytosis. Among acquired conditions, autoimmune hemolytic anemia, severe aplastic anemia, and paroxysmal nocturnal hemoglobinuria are encountered.
Coagulation disorders encountered include bleeding and thrombotic disorders. Patients on oral anticoagulants, hepatic dysfunction, or disseminated intravascular coagulation also require close monitoring in coagulation laboratories. Genetic bleeding disorders like hemophilia A (HA) and B (HB) occur in similar frequencies to global figures. Consanguinity is prevalent in few endogamous communities where autosomal recessive disorders like von Willebrand disease (vWD) are more common. Complexity of coagulation testing, need for expert laboratory staff, high cost of reagents, and equipment are common difficulties for wider availability of coagulation tests.
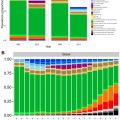
The National Cancer Registry Program (NCRP) was launched in 1981 by the Indian Council of Medical Research (ICMR) for obtaining epidemiologic data on hematological malignancies. A 3-year report (2009–2011) of the Population Based Cancer Registry (PBCR) from 25 registries determined non-Hodgkin lymphoma (NHL) to be the most frequent, followed by lymphoid and myeloid leukemias. Difficulties in complete characterization include unavailability of diagnostic and prognostic facilities like flow cytometry, karyotyping, and molecular genetics. Prohibitive cost of therapy leads to inability of treating physicians to use standard recommended protocols, and hence interprotocol comparative merits are difficult to assess.
Introduction
Hematological practice ranges from availability of advanced diagnostic facilities and treatment to unavailability of basic medical services to rural India. Problems include a huge population (1.21 billion in the 15th national census survey www.census2011.co.in ), socioeconomic disparity, minimal coverage of health insurance schemes, and the government’s inability to provide universal health coverage. Therefore India contributes significantly to global disease burden for hematological disorders. Lack of national registries contributes to inaccurate epidemiologic data and nonavailability of micromapping of diseases. Health services are offered nationally as a public (Government of India–Ministry of Health and Family Welfare) and private service; however, most patients have to arrange personal finances for diagnosis and treatment.
Nutritional iron deficiency anemia (IDA) is common in pediatric practice, whereas anemia caused by bleeding disorders and anemia of chronic disorders (ACD) are more common in adults. Nationally, the most common genetic disorder is thalassemia major (TM), and other genetic red cell disorders include sickle cell anemia, glucose-6-phosphate dehydrogenase (G6PD) deficiency, and hereditary spherocytosis. Among acquired conditions, autoimmune hemolytic anemia, severe aplastic anemia, and paroxysmal nocturnal hemoglobinuria are encountered.
Coagulation disorders encountered include bleeding and thrombotic disorders. Patients on oral anticoagulants, hepatic dysfunction, or disseminated intravascular coagulation also require close monitoring in coagulation laboratories. Genetic bleeding disorders like hemophilia A (HA) and B (HB) occur in similar frequencies to global figures. Consanguinity is prevalent in few endogamous communities where autosomal recessive disorders like von Willebrand disease (vWD) are more common. Complexity of coagulation testing, need for expert laboratory staff, high cost of reagents, and equipment are common difficulties for wider availability of coagulation tests.
The National Cancer Registry Program (NCRP) was launched in 1981 by the Indian Council of Medical Research (ICMR) for obtaining epidemiologic data on hematological malignancies. A 3-year report (2009–2011) of the Population Based Cancer Registry (PBCR) from 25 registries determined non-Hodgkin lymphoma (NHL) to be the most frequent, followed by lymphoid and myeloid leukemias. Difficulties in complete characterization include unavailability of diagnostic and prognostic facilities like flow cytometry, karyotyping, and molecular genetics. Prohibitive cost of therapy leads to inability of treating physicians to use standard recommended protocols, and hence interprotocol comparative merits are difficult to assess.
Disorders of red cells
Nutritional Anemias
India has the largest number of anemic persons worldwide, and common etiologies are nutritional deficiency of iron, folic acid, and vitamin B12 in descending order of frequency. The National Nutritional Anaemia Prophylaxis Programme (NNAPP) was started in 1972 for iron and folic acid supplementation to pregnant women and children. Screening for anemia, iron–folate therapy, and route of administration for prevention and management of anemia was incorporated. The national prevalence of IDA in children younger than 5 years, women 15 to 49 years, and pregnant women are 75%, 51%, and 87%, respectively. Estimates on maternal deaths from anemia/year are 22,000, which contribute to 20% to 40% of maternal deaths and low birth weight. Anemia increases susceptibility to infections, reduced work capacity, and poor concentration. The National Rural Health Mission was launched in 2005 to educate mothers on health and nutrition in villages. Despite continued efforts, anemia continues to be a major problem affecting all population strata ( http://www.mohfw.nic.in ).
Plausible reasons include adverse effects of iron pills, improper utilization of health service, and personal beliefs. Poor iron (<20 mg/d) and folic acid intake (<70 μg/d), poor bioavailability of iron (3%–4%) in a phytate fiber-rich Indian diet, and chronic blood loss due to malaria and hookworm infestations contribute to continued high prevalence of IDA. Oral iron therapy is useful, as ferrous ascorbate and intravenous colloidal preparations are reserved only after inadequate response to oral preparation.
Thalassemias and Hemoglobinopathies
These constitute a heterogeneous group of autosomal-recessive disorders caused by globin gene defects causing quantitative reduction (thalassemias) or qualitative defects (hemoglobinopathies) in globin chains. Thalassemias are classified based on defective globin chain, as α-thalassemia, β-thalassemia, δ-thalassemia, and. Symptomatic hemoglobinopathies include sickling syndromes like homozygous HbS, HbS/BTT, and rarely HbS/HbD Punjab. Double heterozygosity of HbE with beta thalassemia causes symptomatic thalassemia syndrome in eastern states.
Identification of asymptomatic β-thalassemia traits (BTT) has led to screening of partners and offered prenatal diagnosis to at-risk pregnancies. Hypochromic microcytosis with raised red blood cell count is encountered in BTT and α-thalassemia trait. The diagnostic hallmark of BTT is HbA2 of between 4% and 8%, which remains normal (2.2%–3.5%) in α-thalassemia trait. The national average frequency of BTT is 3.5% (range 0.3%–15%) and greater than 10,000 infants affected with TM are born each year. Estimates of α-thalassemia traits are limited, because DNA-based molecular tests are required. The average frequency ranges from 12.5% in the general population to 78.4% in endogamous tribal population. Management of TM includes 3 weekly blood transfusions and iron chelation. Currently, 3 centers are offering bone marrow transplantation (BMT) to TM patients nationally.
Molecular analysis to detect causative mutations for β-thalassemia shows regional differences. There are 64 mutations reported nationally, and the most common 5 traits, namely IVSI-5(G→C), 619 bpdel, IVSI-1(G→T), Codon 41/42(-TCCT), and Codon 8/9(-G) account for 82.5% of alleles. Uncommon mutations like Codon 15(G→A), Codon 30(G→C), Cap+1(A→C), Codon 5(-CT), and Codon 16(-C) account for an additional 11% of mutations. Ten centers perform prenatal diagnosis for reducing the burden of TM.
Other Anemias
ACD is encountered because of disorders like tuberculosis, rheumatoid arthritis, and chronic renal failure. ACD causes increased morbidity and can coexist with IDA. Serum ferritin with soluble transferrin receptor (sTfR/log ferritin ratio) levels can distinguish between ACD and IDA; however, few laboratories perform sTfR. Physicians need to distinguish these disorders to decide treatment with iron supplementation or erythropoietin. Genetic hemolytic anemias like G6PD deficiency are common and present as neonatal hyperbilirubinemia or sporadic infection-related hemolysis. Hereditary spherocytosis, sideroblastic anemia, and congenital dyserythropoieticanemias are seen uncommonly. Recently, homozygosity mapping revealed a founder SEC23B –Y462C mutation in Indian CDA type II patients. Acquired anemias include aplastic anemia, paroxysmal nocturnal hemoglobinuria, and pure red cell aplasia, but there are no documented epidemiologic studies to indicate that the frequencies are different to the West.
Hereditary Hemochromatosis
Hereditary hemochromatosis, a common genetic disorder in the West, is rare in Indians. Low index of suspicion and a high prevalence of IDA could contribute to late presentation of the disorder. The HFE gene mutation c.845G→A; p.C282Y, which accounts for 90% to 95% of cases in Northern Europeans, is absent in Indians. Recently, the authors have found novel mutations in the hemojuvelin gene ( HJV ; Barjinder Kaur, Reena Das, unpublished 2013), and private mutations have been reported from Pakistan and Bangladesh.
Disorders of hemostasis and coagulation
Inherited Coagulation Disorders
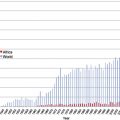
Hemophilias (HA and HB) are the most common inherited bleeding disorders. The Hemophilia Federation India, a nongovernment organization, was established in 1983 and has 76 chapters and provides data on bleeding disorders. In 2013, there were 16,800 registered HA patients, compared with 3000 in 2003. The registry is incomplete, and most patients are registered from west India. India reported 462 vWD cases and 458 cases with platelet function disorders and rare coagulation factor deficiencies. Among the latter, data from 54 hemophilia treatment centers showed FXIII (30%) to be the most common deficiency, followed by deficiencies of FX (15.6%), FVII (15%), and fibrinogen (12.1%). Automation in coagulation in referral hospitals has made tests standardized and reproducible.
Confirmatory tests for vWD (eg, von Willebrand Factor antigen assay, Ristocetin Cofactor assay, and multimer analysis) are available in specialized laboratories, leading to inaccurate diagnosis of type 2vWD. The Indian Society of Hematology and Blood Transfusion and the Christian Medical College, Vellore run an External Quality Assessment Scheme (EQAS) program for hemostasis with more than 100 participants. Prenatal diagnostic facilities for hemophilias are available nationally in five centers.
Qualitative Disorders of Platelets
Platelet function analyzers and aggregometers are not in common use, and therefore the estimates for qualitative disorders of platelets are inaccurate. Bernard Soulier Syndrome and Glanzmann thrombasthenia are uncommonly encountered. Confirmatory flow cytometry has facilitated early diagnosis but is restricted in availability.
Management of Bleeding Disorders
The chronic nature of the bleeding disorders requires comprehensive care involving replacement of deficient coagulation factor, preventing further bleeds, reducing disability, orthopedic support, and rehabilitation programs including psychosocial support to the family. Suboptimal management is reflected by presentation with joint deformities. Currently only 16 of 29 Indian states provide free FVIII and IX replacement to patients during a major bleed (on-demand situations). In other states, patients are dependent on fresh frozen plasma or cryoprecipitate. Financial constraints limit prophylactic replacement therapy. Plasma-derived factor products available are Immunate P and Immunine, whereas, recombinant factors available are Recombinate and Advate. There exists a large gap between the recommended 1 IU/capita usage of FVIII for optimal survival and the available 0.023 IU/capita. Bleeds in vWD are managed with 10 to 20 IU/kg of FVIII concentrates or 1 to 2 cryobags/10 kg weight. Supportive therapy includes topical tranexamic acid (30–40 mg/kg/d) for oral mucosal bleeds or epistaxis. Desmopressin is used in mild vWD with minor bleeds and menorrhagia. Females with vWD require hormonal preparations for regulating menstruation and iron supplementation. Use of rest, ice, compression, and elevation is beneficial and inexpensive supportive therapy. Need for compliance with hormonal therapy for control of ovulation may be overlooked with disastrous consequences. Indian patients have been managed with lower doses of FVIII replacement (35 IU/kg preoperatively and 10–20 IU/kg postoperatively in major surgery) without undue excess of serious bleeding in the setting of major and minor surgical procedures. Development of inhibitors is less frequent in Indians, possibly due to late initiation of replacement therapy. Inhibitors were seen in 6.07% of 1285 HA patients, with highest frequencies from South India (20.99%). Activated prothrombin complex concentrates and recombinant FVII are needed, but the high cost becomes a limiting factor. Immune tolerance is rarely attempted.
Thrombotic Disorders
Hospital-based studies on medical patients and postoperative surgical situations are available on the prevalence of deep vein thrombosis (DVT) and pulmonary embolism (PE). The DVT rate in a retrospective study from South India was 17.46 cases per 10,000 admissions, with 64% of cases in nonsurgical settings. A north Indian study found the incidence of DVT as 2.7/1000 person–days of hospital stay in medically ill patients with grade 1 to 2 mobility. Compression ultrasonography and color Doppler imaging are used for the diagnosis of limb DVT. Angiography, MRI and D-dimer assay are available. Risk factors like factor V Leiden (FVL; G1691A) mutation, deficiencies of protein C, S and antithrombin, and antiphospholipid antibodies are encountered. The prevalence of FVL ranges between 3% and 20% in patients with thrombosis at various sites. In contrast to the western population, prothrombin mutation G20210A is absent.
For thromboprophylaxis, unfractionated heparin is popular because of the low cost of therapy. The low molecular weight heparins (LMWH) available in India are dalteparin, enoxaparin, nadroparin, fondaparin, parnaparin, and fondaparinux. Monitoring of LMWH is mostly empirical, because anti-Xa assay is largely unavailable. The oral anticoagulants available are warfarin and acenocoumarol. Close monitoring of dosage is challenging, as point-of-care instruments are sparsely available. Becuse Indians are predominantly vegetarian, high consumption of green leafy vegetables can lead to variation in anticoagulant effect of the drugs, and good patient education and counseling are required. Experience with the newer anticoagulants is limited.
Hematologic malignancies
Launched by ICMR in 1981, collected national epidemiologic data on hematological malignancies. PBCR from 2009 to 2011 (included 25 centers) found NHL in the top 10 frequent cancers, and Hospital Based Cancer Registries (HBCRs), involving 7 hospitals, showed myeloid and lymphoid leukemia to be among thetop 10 common neoplasms ( Table 1 ).
| Center | Gender | NHL | Myeloid Leukemia | Lymphoid Leukemia | |||
|---|---|---|---|---|---|---|---|
| % | R | % | R | % | R | ||
| Mumbai (2006–07) | Males | 6.1 | 4 | 3.9 | 6 | 2.9 | 10 |
| Females | 3.5 | 6 | 2.2 | a | b | ||
| Bengaluru (2007–09) | Males | 4.6 | 7 | 3.9 | 9 | 3.5 | a |
| Females | 1.9 | 10 | 2.6 | 7 | b | ||
| Chennai (2007–10) | Males | 4.2 | 8 | 4.5 | 7 | 2.9 | a |
| Females | 1.7 | a | 2.7 | 7 | b | ||
| Thiruvananthapuram (2007–10) | Males | 5 | 4 | 4.9 | 5 | 3.8 | 9 |
| Females | 2.7 | 10 | 3.8 | 6 | b | ||
| Dibrugarh (2007–11) | Males | 2.9 | 9 | 1.6 | a | 0.9 | a |
| Females | 1.4 | a | 0.8 | a | b | ||
| Guwahati (2010–11) | Males | 1.9 | a | 0.5 | a | 0.4 | a |
| Females | 1.3 | a | 0.5 | a | b | ||
| Chandigarh (2011) | Males | 4.3 | 7 | 4.3 | 8 | 5.9 | 5 |
| Females | 2.2 | 10 | 2.6 | 8 | b | ||
Related posts:
 The Global Burden of Anemia
The Global Burden of Anemia
 Sickle Cell Disease in Sub-Saharan Africa
Sickle Cell Disease in Sub-Saharan Africa
 Problems and Approaches for Blood Transfusion in the Developing Countries
Problems and Approaches for Blood Transfusion in the Developing Countries
 Hematological Practice in India
Hematologic Changes Associated with Specific Infections in the Tropics
Improving Laboratory and Clinical Hematology Services in Resource Limited Settings
Hematological Practice in India
Hematologic Changes Associated with Specific Infections in the Tropics
Improving Laboratory and Clinical Hematology Services in Resource Limited Settings
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


