Thalassemias and hemophilias are the most important inherited hematological diseases in Hong Kong and China. Prenatal diagnosis has significantly decreased the burden of these diseases. For thalassemia major, adequate transfusion and iron chelation therapy have dramatically improved patient outlook. Hematopoietic stem cell transplantation is curative for thalassemia major and is increasingly adopted. The efficacy of arsenic trioxide in acute promyelocytic leukemia (APL) was discovered in China. An oral formulation of arsenic trioxide was developed in Hong Kong for newly diagnosed and relapsed APL patients. With combination chemotherapy containing non-P-glycoprotein-dependent drugs and L-asparaginase, durable remission can be achieved in the most patients.
Key points
- •
Prenatal diagnoses of thalassemia, the most important inherited hematological disease in Hong Kong and Southern China, and hemophilia A and B have very significantly decreased the burden of these disorders.
- •
Adequate transfusion and iron chelation therapy for thalassemia major patients, and optimal factor replacement for hemophilia patients, have dramatically improved the outlook of these disorders.
- •
Arsenic trioxide is an active drug for acute promyelocytic leukemia on presentation and at relapse; the availability of an oral formulation means that long-term consolidation of remission with this drug can be achieved.
- •
Natural killer cell lymphomas, prevalent in Hong Kong and parts of China, have much better prognosis when treated with combination chemotherapy containing non-P-glycoprotein-dependent drugs and L-asparaginase.
Introduction
China has a population of 1.3 billion. Hong Kong is a special administrative region in China, with a population of 7.5 million. The Han ethnic group accounts for about 92% of the population in both places. Disease patterns in Hong Kong therefore closely reflect those in China.
The first major hematology center combining clinical and laboratory research was established in China in 1958. In Hong Kong, research in blood diseases also started in the late 1950s. Allogeneic hematopoietic stem cell transplantation (HSCT) was first performed in 1981 in China, and in 1990 in Hong Kong.
Health Care Systems in China and Hong Kong
For a long time, patients or their employers were responsible for medical expenses in China. Recently, 3 systems of government-subsidized insurance schemes have been introduced, which cover up to 95% of the population. Hong Kong adopted a model similar to a national health care system, with patients paying a nominal daily fee of less than 15 US dollars even for complicated treatment such as HSCT.
However, with rising medical costs, such systems are becoming difficult to maintain. Whether the soaring fees should be met by increasing government expenditure or higher insurance premiums is hotly debated.
Burden of Hematological Diseases
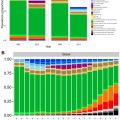
Nonmalignant diseases including hemoglobin and bleeding disorders were predominant hematological problems in China and Hong Kong. However, malignant diseases now constitute the major burden, owing to an aging population and improvement in patient survivals.
Introduction
China has a population of 1.3 billion. Hong Kong is a special administrative region in China, with a population of 7.5 million. The Han ethnic group accounts for about 92% of the population in both places. Disease patterns in Hong Kong therefore closely reflect those in China.
The first major hematology center combining clinical and laboratory research was established in China in 1958. In Hong Kong, research in blood diseases also started in the late 1950s. Allogeneic hematopoietic stem cell transplantation (HSCT) was first performed in 1981 in China, and in 1990 in Hong Kong.
Health Care Systems in China and Hong Kong
For a long time, patients or their employers were responsible for medical expenses in China. Recently, 3 systems of government-subsidized insurance schemes have been introduced, which cover up to 95% of the population. Hong Kong adopted a model similar to a national health care system, with patients paying a nominal daily fee of less than 15 US dollars even for complicated treatment such as HSCT.
However, with rising medical costs, such systems are becoming difficult to maintain. Whether the soaring fees should be met by increasing government expenditure or higher insurance premiums is hotly debated.
Burden of Hematological Diseases
Nonmalignant diseases including hemoglobin and bleeding disorders were predominant hematological problems in China and Hong Kong. However, malignant diseases now constitute the major burden, owing to an aging population and improvement in patient survivals.
Nonmalignant hematological diseases: genetic disorders
The most common genetic diseases in this region are thalassemias (α- and β-thal) and glucose-6-phosphate dehydrogenase (G6PD) deficiency.
Thalassemias
The combined carrier rates for α + – and α 0 -thalassemia in Hong Kong are 4% and 3.5% for β-thalassemia minor. In China, thalassemias are mainly restricted to the southern provinces of Guangxi and Guangdong, with α-thalassemia much more prevalent in Guangxi, with a carrier rate of up to 15%. In Guangdong, incidences of both types of thalassemias are similar to those in Hong Kong. In Northern China, thalassemias are uncommon.
Prenatal Diagnosis for Thalassemias
Couples with the same thalassemia trait (α 0 -thal or β-thal minor) carry a 25% risk of having a homozygous child. The homozygous α 0 -thal fetus (Hb Barts hydrops fetalis) is incompatible with life. Early termination of pregnancy prevents maternal morbidity or even mortality. The homozygous β-thalassemia child (β-thalassemia major) lives, but is transfusion-dependent and suffers from the consequences of iron overload. Screening of at-risk couples in early pregnancy and subsequent prenatal diagnosis (PND) are advocated. Since 2000, screening is offered to all pregnant women on antenatal booking at every public hospital and maternity center in Hong Kong. A maternal mean corpuscular volume of less than 80 fl and a normal serum iron level necessitates investigation of the couple. In Hong Kong, PND was first performed in 1975 by globin-chain analysis of fetal blood. With the establishment of a DNA-based PND program in 1982, the detection of α-globin genes in fetal DNA excludes homozygous α 0 -thal, but misses the occurrence of nondeletion Hb-H hydrops fetalis. The various common nondeletion α-globin gene defects can be detected by reverse dot-blot or by microarray based on an allele-specific arrayed primer-extension technology ; this is important because nondeletion Hb-H accounts for 22.8% of Hb-H disease, with at least 4 types giving rise to hydrops fetalis. However, α-Quong Sze (QS) and α-Constant Spring (CS), highly prevalent in Guangxi province and Southeast Asia, respectively, rarely cause hydrops fetalis. Most Hb-H patients are not transfusion-dependent and have a long lifespan. Their only morbidity is increasing iron overload with age, which may then benefit from short-term iron chelation therapy. Hence, termination of pregnancy is not justified for nonhydropic Hb-H fetus.
An alternative strategy is noninvasive ultrasound diagnosis by measurement of the placental thickness or cardiothoracic ratio (CTR) and/or middle cerebral artery systolic velocity (MCA-PSV) of the fetus at 12 to 15 weeks of gestation. Transient and marginal increases in CTR and MCA-PSV have been reported in 2 fetuses affected by Hb-H-QS, but both were delivered alive. Hence, in cases of marginal increase in CTR, serial follow-up will be necessary and fetal DNA analysis is needed to confirm a positive ultrasound diagnosis.
In β-thalassemia, each ethnic group has its own specific gene mutations. For ethnic Chinese (constituting 95% of the Hong Kong population), 12 mutations of the β-globin gene have been characterized, with 4 common ones accounting for 87% of cases. A reverse dot-blot or microarray with allele-specific sequences for β-globin gene mutations provides a convenient means of PND. Noninvasive techniques with array-based detection of the paternal-derived mutation and informative paternal-derived single-nucleotide polymorphisms in maternal plasma-DNA have been explored. This method potentially achieves a diagnosis in 40% of cases, thus obviating invasive procedures.
In China, PND has been available in Guangzhou, Beijing, and Shanghai since the 1990s, but is mainly self-financed. Recent government funding is available to encourage PND among ethnic minorities in the Guangxi province.
Preimplantation Genetic Diagnosis
Since 2002, preimplantation genetic diagnosis (PGD) is offered to thalassemia couples with fertility problems, or a history of repeated elective terminations following PND of affected pregnancies. Only embryos diagnosed as unaffected are transferred to establish pregnancy.
Preimplantation Genetic Diagnosis of α-Thalassemia
Single-cell multiplex polymerase chain reaction (PCR) of the normal and α 0 -thal alleles is performed. The use of duplicate blastomeres prevents misdiagnosis due to allele dropout (ADO), and a second seminested PCR ensures specific amplification. The use of whole genome amplification, before allele-specific PCR, has decreased ADO.
Preimplantation Genetic Diagnosis of β-Thalassemia
For couples with a previous β-thalassemia major child, PGD is performed to select embryos that are either normal or have β-thalassemia minor, and when available, HLA-identical to the affected elder sibling, with a view to obtaining cord blood stem cells for HSCT.
Transfusion and Iron Chelation Therapy for Thalassemia Major
In 2009, it was estimated that 9.5% of the blood supply in Hong Kong (13,460 units) was used by about 380 transfusion-dependent thalassemia patients, with a predicted annual consumption increment of 0.8%. Blood safety has progressively improved, from the introduction of serologic testing for hepatitis C in 1991 to the implementation of rapid nucleic acid testing for infectious agents and full compliance with the ISO (International Organization for Standardization) international standards in the late 2000s. Thalassemia patients have been provided with prestorage filtered blood as a standard for the past 15 years. Iron chelation with subcutaneous desferrioxamine started in the late 1970s. Since then, regular blood transfusion and subcutaneous desferrioxamine have become the standard management. However, complications due to iron overload, including cardiomyopathy and endocrinopathy, still occur in some patients. Infections by Klebsiella spp in different sites were commonly encountered, which may be associated with significant morbidity and mortality. Other desferrioxamine-associated complications such as skeletal dysplasia are occasionally observed. Deferiprone was shown in a randomized control study to significantly reduce ferritin levels in poorly chelated Chinese patients when combined with desferrioxamine. Therefore, combination therapy of desferrioxamine with deferiprone is frequently used in poorly chelated patients, with benefits validated by MRI T2*. The oral iron chelator deferasirox is recommended for first-line treatment in children aged between 2 and 6 years, and for second-line treatment for children older than 6 years, who are not responding optimally to combined desferrioxamine with deferiprone. Renal tubular dysfunction has been observed to be a frequent but reversible adverse effect.
Hematopoietic Stem Cell Transplantation for Thalassemia Major
In Hong Kong, HLA-matched sibling HSCT for thalassemia started initially with marrow in 1991 and with cord blood in 1994. Using conditioning regimens containing antithymocyte globulin, HSCT results in transfusion independence in more than 90% of recipients. HSCT is a curative treatment that may be suitable for centers unable to meet the demands of lifelong transfusion and chelation and is increasingly adopted in Southern China. Because of a one-child policy, unrelated donor HSCT is predominant in China, with good results reported.
Hemophilia
The incidences of hemophilias A and B in China have not been well-defined. In a global study of hemophilia A, the incidence in China was reported to be merely 0.3 to 0.5/100,000 males, as compared with 7.6 to 8.0/100,000 males in the United States and 17.4 to 22.6/100,000 males in the United Kingdom. This low incidence was likely due to underreporting. Given the vast population in China, hemophilias are important inherited diseases. Although patients with hemophilias may lead a normal life with adequate coagulation factor support, the consequent enormous economic and emotional costs make PND necessary to communities where termination of pregnancy is acceptable.
Prenatal Diagnosis for Hemophilias
In Hong Kong, PND for hemophilia A has been available since 1989. Except those with intron 18 or 22 inversions in the F8 gene, 3 common restriction fragment length polymorphisms provide informativeness for 98% of Chinese families ; this is further enhanced by analysis of dinucleotide repeats in introns 13 and 22. For hemophilia B, the genetic aberrations are heterogeneous and more than 900 mutations of the F9 gene have been characterized. A microarray that examines simultaneously 69 common mutations of the F9 gene has been devised, covering 53% of the 2891 mutation entries in the F9 database.
Treatment of Hemophilias
In Hong Kong, plasma-derived factor VIII and IX concentrates are manufactured from plasma of normal blood donors. This local source of factor concentrates, while adequate for hemophilia B patients, is inadequate for the bigger population of hemophilia A patients, so that plasma-derived factor VIII concentrates are needed from other suppliers. Before the implementation of prophylactic use of factor concentrates in 2004, a significant portion of patients developed chronic joint problems. This complication has much decreased since. Recombinant factor VIII is not reimbursed.
In China, the establishment of the Hemophilia Treatment Centre Collaborative Network of China, in conjunction with the World Federation of Hemophilia, has improved the identification and treatment of hemophilia patients.
Glucose-6-Phosphate Dehydrogenase Deficiency
G6PD deficiency occurs in approximately 4% to 6% of males in South China and Hong Kong, The gene is X-linked. As well as hemizygous male patients, heterozygote female patients (mosaic for normal and G6PD-deficient red cells due to variable X-inactivation of the normal chromosome) may also suffer from mild hemolysis. Neonatal screening of the genetic trait has been implemented in all public hospitals in Hong Kong since the 1980s. Mothers of babies carrying the genetic trait are given a list of offending drugs and agents to avoid.
The most serious clinical manifestation of G6PD deficiency is massive intravascular hemolysis, which can occur as an idiosyncratic reaction to multiple drugs and chemicals (primaquine, sulfonamide, nitrofurantoin, naphthalene, and aniline dye), after ingestion of fava bean (favism) or herbs, and as a complication of febrile illnesses (particularly typhoid fever and viral hepatitis). In the neonatal period, hemolysis may lead to kernicterus. A useful hallmark of severe oxidative injury in G6PD-deficient erythrocytes is the appearance of hemighost. Furthermore, the percentage of hemighosts also indicates the severity of hemolysis within the next 1 to 2 days, providing a useful guide to the necessity of prophylactic measures needed to avert renal shutdown.
Related posts:
 The Global Burden of Anemia
The Global Burden of Anemia
 Sickle Cell Disease in Sub-Saharan Africa
Sickle Cell Disease in Sub-Saharan Africa
 Problems and Approaches for Blood Transfusion in the Developing Countries
Problems and Approaches for Blood Transfusion in the Developing Countries
 Hematological Practice in India
Hematologic Changes Associated with Specific Infections in the Tropics
Improving Laboratory and Clinical Hematology Services in Resource Limited Settings
Hematological Practice in India
Hematologic Changes Associated with Specific Infections in the Tropics
Improving Laboratory and Clinical Hematology Services in Resource Limited Settings
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


