and Karl Reinhard Aigner3
(1)
Department of Surgery, The University of Sydney, Mosman, NSW, Australia
(2)
The Royal Prince Alfred and Sydney Hospitals, Mosman, NSW, Australia
(3)
Department of Surgical Oncology, Medias Clinic Surgical Oncology, Burghausen, Germany
In this chapter, you will learn about:
Cancers of the lips
Cancers of the mouth, anterior tongue and buccal mucosa
Cancers of the posterior tongue, tonsillar region and pharynx
Cancers of the post-nasal space
Cancer of the larynx
Salivary gland cancers
Cancers of the thyroid gland
Cancers of the lips, mouth, tongue, nasal cavity, the paranasal air sinuses, throat, larynx and pharynx constitute about 5 % of all cancers recorded in the United States, and the incidence is similar in most developed and developing countries. Most of these cancers are of squamous cells lining the mucosal epithelium. They are similar in type to squamous cell carcinoma (SCC) of the skin. However, they tend to behave in a more malignant and more aggressive fashion than SCCs of skin. As a rule the further the cancers are away from the lips, the more aggressively they behave. Cancers of the lips are more aggressive than skin cancers. That is, they tend to grow more rapidly locally and have a greater tendency to spread to draining lymph nodes at an earlier stage. Cancers of the floor of the mouth, the anterior two-thirds of the tongue and palate are more aggressive than cancers of the lips. Cancers of the back of the tongue, in the region of the tonsils and pharynx and upper air passages are the most aggressive. Cancers of the vocal cords of the larynx are an exception to this rule. Possibly because the vocal cords are poorly vascularised, these cancers tend to remain localised to the vocal cords with no evidence of spread when they first cause symptoms. The majority are readily curable at that stage.
The further the cancers are away from the lips, the more aggressively they behave.
These cancers are all much more common in smokers than non-smokers and are most common in males over 50. It has been estimated that cancers in the mouth and throat are about six times more common in smokers than in non-smokers, and this is increased to about 15 times if the smokers are also heavy drinkers of alcohol. Other pre-malignant conditions that predispose to cancer in the mouth include leukoplakia, papillomas and chronic irritation from such causes as ill-fitting dentures or jagged teeth (see Chap. 1).
14.1 Cancers of the Lips
Cancers of the lips being more obvious than cancers further back in the mouth or throat are usually diagnosed at an earlier and more curable stage. They may develop as a thickening in an area of hyperkeratosis (sun damage) – most commonly on the lower lip. They tend to ulcerate and possibly bleed or may form a lump. They may then metastasise to lymph nodes under the jaw and in the sides of the neck that may be felt as enlarged and usually firm or hard lymph nodes.
A biopsy is taken to confirm the diagnosis and thereafter treatment is usually by surgical excision. Good results, both cosmetically and clinically, are usually achieved. Radiotherapy can also be used with good results.
For larger cancers of the lips, either radical surgery (removing a large part of the lip with some form of plastic or reconstructive surgery to fashion a new lip) or radiotherapy may be used, and the chances of cure are still good.
If hard, enlarged lymph nodes are present either when the patient is first seen or at a later follow-up visit to the doctor, these are best treated by surgical block dissection to remove all local lymph nodes.
Occasionally, a patient first consults a doctor when the cancer is very large. Possibly the whole of the lip is involved with cancer. In these patients, considerable success can be achieved with induction (neoadjuvant) chemotherapy to first reduce the cancer, then following this treatment with radiotherapy or surgery or both. If special facilities for intra-arterial chemotherapy are available, the chemotherapy may be best given regionally by infusion into the arteries that supply blood to the cancer region, but such treatment should be done only in specialist clinics with special experience, equipment and skills. It is not necessary to use this more complicated, combined treatment for smaller cancers that can be readily cured by operation or by radiotherapy (Figs. 14.1, 14.2 and 14.3).
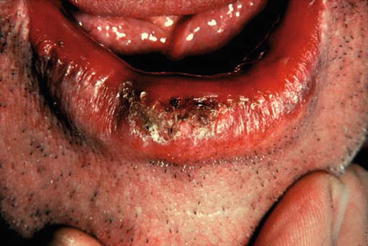

Fig. 14.1
A squamous cell carcinoma developing in sun-induced hyperkeratosis of the lower lip
Fig. 14.2
A localised SCC of lower lip
Fig. 14.3
(a, b) Anteroposterior and lateral photographs of a man who first presented with this very advanced SCC of his lower lip. The swelling under the jaw was a mass of metastatic cancer in lymph nodes. (c) Photograph of the same lip after treatment with chemotherapy (given over 5 weeks by continuous intra-arterial infusion). Three weeks after completion of chemotherapy, “follow-up” treatment with radiotherapy was started. Right-sided cervical nodes and submental nodes were resected 4 weeks after completion of radiotherapy. They included a small residual node mass containing some cancer cells. (d) The end result. This photograph was taken 2 years after completion of treatment. (e) Lateral view of the end result. This man was well and without evidence of cancer when last seen 12 years after treatment
14.2 Cancers of the Floor of the Mouth (Under the Tongue), Anterior Two-Thirds of the Tongue and Buccal Mucosa (Inside the Cheek)
These cancers are more aggressive than lip cancers. Lymph nodes are involved in about 30 % of cases.
These cancers are usually first noticed as an ulcer or a lump either by the patient or sometimes by their dentist before symptoms develop. Other common features are bleeding or localised soreness. These cancers tend to be on the surface at first but soon invade locally with firm induration surrounding the lump or ulcer. They usually become quite tender. Diagnosis is confirmed by taking a small biopsy for microscopic examination.
Cancers in the buccal mucosa of the cheek pouch are most common in India, Pakistan, New Guinea and the Solomon Islands due to the common practice of chewing betel nut. After initial chewing, the nut is often stored in the cheek pouch where its carcinogenic properties take effect.
Most cancers are well treated by surgical excision or radiotherapy. Involved lymph nodes are best treated by block dissection of all lymph nodes in the region. Sometimes reconstructive surgery may be required to replace resected tissue.
For larger cancers in the floor of the mouth, anterior two-thirds of tongue or the cheek, treatment by prior induction chemotherapy followed by radiotherapy or surgery may give the best results. In some specialised clinics, such induction chemotherapy is given by intra-arterial infusion more directly to the tumour site.
By these combined treatment methods, cures can now be achieved in patients with advanced cancers, which, until recently, were considered incurable or possibly only curable by the most radical surgery. Such treatments do require special skills, equipment and experience and should be carried out only in experienced cancer centres (Chap. 8) (Figs. 14.4, 14.5 and 14.6).

Fig. 14.4
Photographs showing (a) leukoplakia in the buccal mucosa of a 54-year-old heavy smoker and heavy alcohol drinker; (b) the same mucosa 2 years later. It had developed into a papillary squamous carcinoma
Fig. 14.5
An ulcerating SCC of the side of the tongue
Fig. 14.6
(a, b) SCC of the floor of the mouth. Most of these cancers are associated with smoking
Case Report
Squamous cancer of the tongue
Tony was a 70-year-old Italian migrant enjoying his retirement in Sydney, Australia. He had generally good health despite a smoking history of 40 years’ duration. He had rolled his own cigarettes (ten daily for 40 years) but had stopped smoking 5 years before his first consultation. After stopping smoking he continued to enjoy beer and wine, having up to five alcoholic drinks daily.
Two months prior to presentation, Tony had noticed a small lump on the side of his tongue. This was initially painless, so he ignored it thinking he must have bitten his tongue in his sleep. However, the lump progressively enlarged. After a few weeks, he felt pain in his tongue, jaw and left ear. Eventually the lump came to interfere with his speech and swallowing. He reported the problem to his family doctor.
His doctor recognised a large cauliflower-like tumour on the left side of his tongue. He was promptly referred to a head and neck surgeon. Tony was then advised that he had developed a cancer of the side of his tongue. A small biopsy was performed in the surgeon’s office under local anaesthesia. Within 24 h it confirmed an invasive SCC.
Neither his family doctor nor the surgeon could feel any involvement of lymph nodes in the neck. For confirmation, Tony underwent a CT scan. There was no evidence of nodal metastasis. A chest X-ray showed some emphysema, but no sign of spread to the lungs.
The tongue cancer was defined as Stage II (T2N0M0). However, because of the tumour’s size and depth of invasion, there was still a 25 % chance of spread to the neck. He was advised to have surgical excision of both the primary tumour and the lymph nodes at risk in the left neck.
Tony underwent excision of the left side of his anterior tongue. His tongue was repaired primarily. A total of 45 cervical lymph nodes were removed. Of these, one proved to contain metastatic cancer. As a result, he also required post-operative radiation therapy to the mouth and neck.
The treatment for his tongue cancer took almost 3 months. Swallowing was particularly difficult during the radiation therapy. He lost a total of 18 kg in weight. His speech remained surprisingly good. After 1 year, he continues to gradually recover from his ordeal. His mouth is very dry due to irradiation involving his salivary glands but some taste has returned and he has managed to regain some weight. He will remain under surveillance for head and neck cancer for several years to come.
14.3 Cancer in the Posterior Third of Tongue, Tonsillar Region and Pharynx
These cancers may present as an ulcer, a lump in the throat or tongue or sometimes a constant sore throat that has not responded to conservative treatment including antibiotics. Sometimes patients will first notice a lump in the side of the neck that is, in fact, an enlarged, hard lymph node containing metastatic cancer. Diagnosis may appear to be obvious but must be confirmed by biopsy.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


