Hamstrings Muscle Group (Posterior Thigh) Resection
Jacob Bickels
Martin M. Malawer
BACKGROUND
The posterior thigh (hamstring musculature) is the least common of the three compartments of the thigh for sarcomas to arise within. About 15% to 20% of the soft tissue sarcomas of the thigh arise within the posterior hamstring musculature. There is great variation in the size of tumors that occur in the posterior thigh, and the location varies from a proximal location near the ischium to a distal location involving the popliteal space. The posterior thigh is a quiet surgical area; the most significant structure is the sciatic nerve. Almost all low-grade sarcomas can be resected safely. Most high-grade sarcomas can be resected by either a complete or partial muscle group resection. The sciatic nerve is rarely involved, either because of direct tumor extension or because of a primary nerve tumor.
En bloc resection of the sciatic nerve with a malignant tumor of the posterior thigh rarely is done; this has traditionally been considered an indication for amputation.2 This approach was based on the belief that the expected motor and sensory loss around the leg and foot would result in an intolerable functional deficit and the development of pressure sores and, therefore, high rates of secondary amputation. However, it has been shown that limb-sparing resection of the sciatic nerve is associated with a good functional outcome in most patients who have this procedure. Most patients were ambulatory; all used a short-leg brace because of the peroneal nerve palsy, but only half required a walking aid (crutches or a cane).1
ANATOMY
The posterior compartment consists of the semimembranosus, the semitendinosus, and the long and short heads of the biceps muscles. All of these muscles originate at the ischium and the linea aspera. No major artery is involved with this compartment.
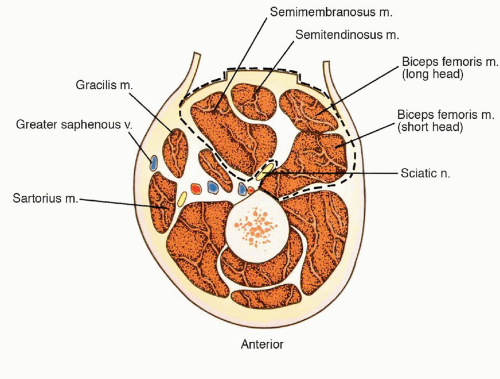
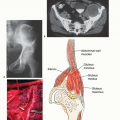
FIG 1 • Cross-sectional anatomy of the midthigh showing the extent of compartmental resection of the posterior thigh. The proximity of the sciatic nerve to large sarcomas within the posterior compartment is clearly indicated. (Courtesy of Martin M. Malawer.)
The sciatic nerve is the most significant structure. It runs from the sciatic notch into the compartment from lateral to the ischium and divides the medial and lateral hamstrings. A thick sheath surrounds the nerve, acting as a barrier to direct tumor extension. Often, tumors arise within one of the individual muscles of the posterior thigh or between the muscles. In most cases, the sciatic nerve is displaced around an adjacent muscle.
INDICATIONS
Almost all low-grade sarcomas of the posterior thigh can be treated by partial or total resection of the involved muscle. High-grade sarcomas are treated by complete myomectomy of the muscle involved. If the tumor is extramuscular but still remains within the compartment, a partial muscle group resection is performed (FIG 1). Multiple muscles or the entire compartment can be resected instead of an amputation.
Contraindications for limb-sparing resections of the posterior compartment include the following:
Extension into ischiorectal space: This makes the resection more difficult and may indicate the need for an amputation.
Extension into the popliteal space with vascular compromise
Femoral involvement with cortical destruction
IMAGING AND OTHER STAGING STUDIES
Preoperative evaluation must include the ischium, the ischiorectal space, the retrogluteal area, and the popliteal space for tumor extension.
The most useful imaging studies are computed tomography (CT) and magnetic resonance imaging (MRI). Angiography is required only if tumor extends distally into the popliteal space (FIG 2).
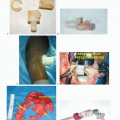
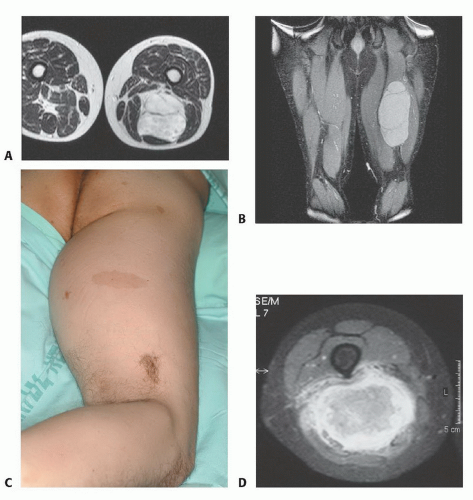 FIG 2 • Axial (A) and coronal (B) magnetic resonance (MR) images of a myxoid liposarcoma of the posterior thigh. The tumor is extramuscular, arising in the space between the medial and lateral hamstrings. Clinical picture (C) and axial MR image (D) of a high-grade neurofibrosarcoma of the posterior thigh in a patient with an underlying neurofibromatosis. Café-au-lait spots are present on the patient’s thigh. This is a primary tumor of the sciatic nerve and must be removed to obtain wide margins of resection. |
TECHNIQUES
▪ Position and Dissection
The patient is placed in a prone position.
A long midline incision is used. An ellipse of skin is outlined so that there is a 2-cm margin of skin around the old biopsy site.
The skin flaps are dissected, with care being taken to taper the flaps as one encounters the lateral margins of the dissection.
The medial extent of the dissection is the gracilis muscle, and the lateral extent is the iliotibial tract (TECH FIG 1).Related posts:
 Biopsy of Musculoskeletal Tumors
Biopsy of Musculoskeletal Tumors
 Overview of Resections around the Shoulder Girdle
Overview of Resections around the Shoulder Girdle
 Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
 Surgical Management of Metastatic Bone Disease: Pelvic Lesions
Surgical Management of Metastatic Bone Disease: Pelvic Lesions
 Adductor Muscle Group (Medial Thigh) Resection
Adductor Muscle Group (Medial Thigh) Resection
 Distal Femoral Resections with Endoprosthetic Replacement
Distal Femoral Resections with Endoprosthetic Replacement

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


