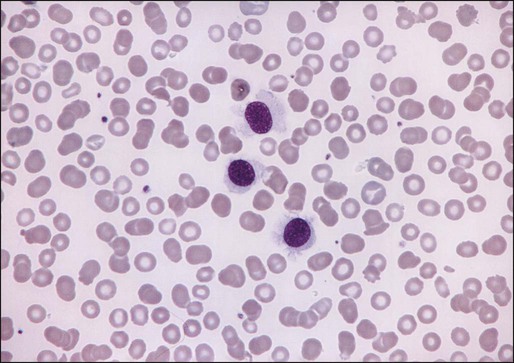
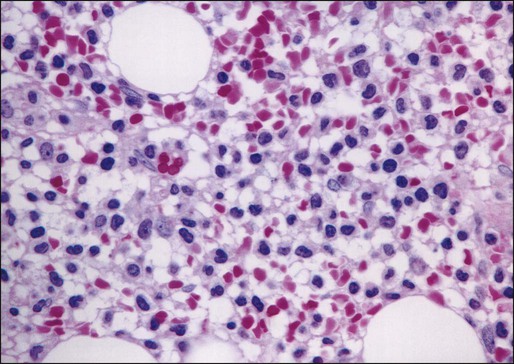
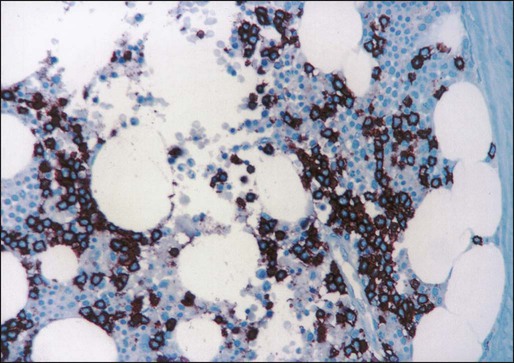
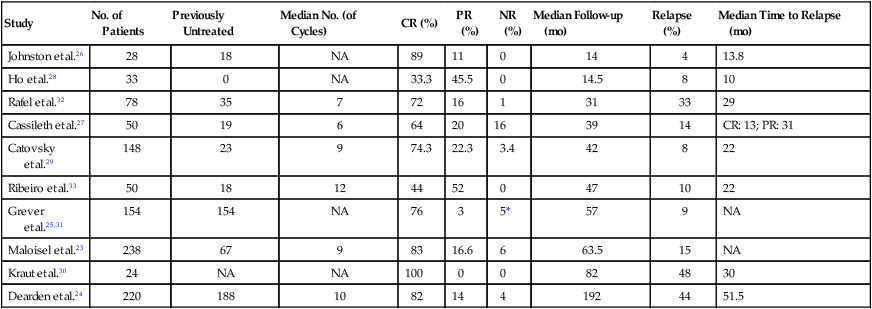
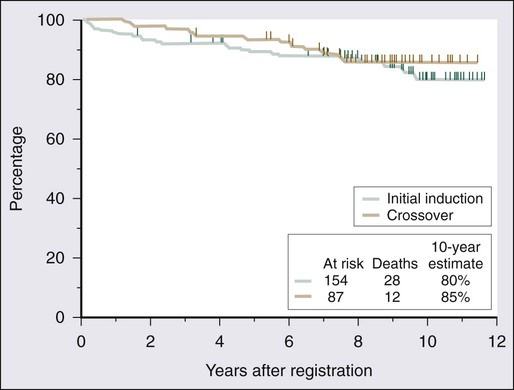
Jae H. Park and Martin S. Tallman • Hairy cell leukemia (HCL) is an uncommon clonal B-cell lymphoproliferative disorder. • BRAF V600E mutation is present in nearly all cases of HCL but absent in other B-cell lymphoproliferative disorders and represents a disease-defining genetic event in HCL. • Physical findings generally are confined to splenomegaly. • The purine analogs are the therapeutic agents of choice. • Most patients who receive treatment with cladribine or pentostatin have prolonged survival. • BL22 or HA22, an immunoconjugate of an anti-CD22 antibody linked to a truncated Pseudomonas exotoxin A, is a novel agent that has been very effective in the management of relapsed and refractory HCL. • BRAF inhibitors represent the first molecularly targeted therapy in HCL and will soon be explored in clinical studies. Hairy cell leukemia (HCL) is a rare chronic B-cell lymphoproliferative disorder with unique morphologic features and an excellent prognosis. Bouroncle and colleagues described 26 patients in 1958 with what then was called “leukemic reticuloendotheliosis” and are credited with the initial description of HCL as a distinct clinical entity.1 The disease is characterized by splenomegaly, pancytopenia, and infiltration of the bone marrow with lymphocytes that have irregular cytoplasmic projections when identified in the peripheral blood.2,3 Although the origin of the malignant cell was unclear for some time, immunoglobulin gene rearrangements confirm that the disease is a clonal B-cell malignancy.6–6 The pattern of expression of B-cell–associated surface antigens (see later discussion) reflects a degree of differentiation between the mature B cell of chronic lymphocytic leukemia and the plasma cell of multiple myeloma.7,8 A majority of patients have few symptoms at the time of diagnosis. However, occasionally patients are seen with life-threatening pancytopenia, symptomatic splenomegaly, serious infections, or constitutional signs and symptoms justifying treatment, or such problems may develop later in the disease course.9,10 Treatment strategies have evolved relatively rapidly during the past 50 years. Splenectomy was the first effective treatment described and remained the therapeutic modality of choice for many years. Although the mechanism of benefit is not clear, removing the spleen leads to normalization of the peripheral blood counts in approximately one half of all patients.11–14 Interferon-α induces a high overall response rate; however, most responses are partial.14–21 Remarkable progress has occurred with the introduction of the two purine analogs, 2′-deoxycoformycin (2′-DCF; pentostatin)22–33 and 2-chlorodeoxyadenosine (2-CdA; cladribine).24,34–44 Most patients with both previously treated and untreated HCL achieve durable complete remission with either of these agents. With use of molecular techniques, however, minimal residual disease (MRD) can be identified in most if not all patients, suggesting that most patients are not actually cured of their disease. Nevertheless, with either purine analog, a majority of patients enjoy prolonged periods of progression-free and overall survival. Recently, whole-exome gene sequencing of HCL identified the presence of BRAF V600E mutation in nearly all patients with this mutation absent in other B-cell lymphoid malignancies.45 This discovery of the highly specific and recurrent mutation in HCL identified the BRAF V600E mutation as the disease-defining genetic event in HCL and has generated great interest and excitement for novel diagnostic possibilities and therapeutic targeting of the BRAF pathway. Relatively little is known about the epidemiology of HCL, partly because of its rarity. In the United States, HCL represents 2% of adult leukemias, with only approximately 600 to 800 new cases diagnosed each year.46,47 Although anecdotal reports of familial HCL have been published, no clear genetic predisposition has been recognized.48–54 The median age at diagnosis is 52 years; and for unclear reasons the disease occurs in men more often than in women, with a sex ratio of approximately 4 : 1.55 Although reported incidence rates are similar in the United States and Great Britain,46,47 classic HCL is rare in Japan, where a distinct variant form has been described.58–58 The etiology of HCL has not been determined. An association with exposure to benzene,59,60 organophosphorus insecticides,61 or other solvents62 has been suggested but has not been confirmed.63 Exposure to radiation,64 agricultural chemicals,60 or wood dust47 and a previous history of infectious mononucleosis62 also have been suggested as potential associations. However, among a majority of patients, no such exposures can be identified. Cyclin D1, an important cell cycle regulator, may play a role in the molecular pathogenesis of HCL. Overexpression of the cyclin D1 protein has been described in HCL patients.65,66 Unlike in mantle cell lymphoma, 11q13 rearrangements are not detected in most patients with HCL, suggesting other mechanisms of gene deregulation.66 The hairy cell may be derived from the memory B cell because the genome-wide expression profile is close to that of postgerminal center B cells.67 Evidence suggests that hairy cells may come from B cells of the splenic marginal zone because hairy cells have a splenic expression signature that reflects tissue components, such as the marginal zone, that are not well represented in lymph node tissue.68 However, expansion of the red pulp of the spleen, so characteristic of HCL, is in contrast to expansion of the white pulp, which involves the splenic marginal zone. Hairy cells express B-cell CLL/lymphoma 2 (BCL2), a universal inhibitor of apoptosis.69 Survival of hairy cells may be further promoted by overexpression of Fms-like tyrosine kinase 3 (FLT3), which activates the phosphatidylinositol-3-kinase (PI3K) pathway that activates anti-apoptotic signals.67,70 Hairy cells produce basic fibroblast growth factor (bFGF) and overexpress bFGF tyrosine kinase receptor,67,71 which can activate the PI3K-Akt cascade.72 The characteristic appearance of the hairy cells is due to expression of β-actin, which is polymerized to F-actin, located in the cortical cytoskeleton, in the peripheral part of the cell, that serves to support the hairlike projections.67 The actual hairlike projections probably are due to increased expression of pp52, a leukocyte-specific intracellular phosphoprotein, that binds to F-actin.73,74 More recently, whole-exome gene sequencing of HCL identified BRAF V600E mutation in the entire tumor-cell clone of nearly all patients with HCL, which is absent in other B-cell lymphoid malignancies.45 This discovery implicates the BRAF V600E mutation in the pathogenesis of HCL. The concept that the BRAF V600E mutation may represent a key driver mutation in HCL is further supported by a preliminary evidence of striking clinical activity of the specific BRAF inhibitor vemurafenib in a patient with refractory HCL.75 However, further characterization of the BRAF pathway in HCL and formal clinical studies of BRAF inhibitors in this disease will be required to confirm the implicated pathogenic mechanisms of the BRAF pathway in HCL. At the time of diagnosis, most patients have symptoms attributable to anemia, neutropenia, thrombocytopenia, or splenomegaly. Approximately 25% of patients have fatigue or weakness and 25% have infection; another 25% come to medical attention because of incidental discovery of splenomegaly or an abnormal peripheral blood cell count.55 Most patients are relatively well at the time of diagnosis. The most common and invariably the only physical finding is splenomegaly, which occurs in approximately 80% of patients.3,55 The spleen is palpable 5 cm below the left costal margin in approximately 60% of patients. Hepatomegaly occurs in approximately 20% of patients. Unlike in many other chronic lymphoproliferative disorders, peripheral adenopathy is uncommon at diagnosis, with less than 10% of patients having peripheral nodes larger than 2 cm. Although adenopathy is not common at diagnosis, internal adenopathy may develop after a prolonged disease course76,77 and is present in 75% of patients at autopsy.78 The characteristic distribution in HCL is probably caused by expression of the integrin receptor α4β1 by the hairy cells and its interaction with the vascular cell adhesion molecule-1 (VCAM-1) found on splenic and hepatic endothelia and in bone marrow and splenic stroma.79 Patients with HCL are susceptible to both gram-positive and gram-negative bacterial infections.80 In addition, susceptibility to atypical mycobacterial infections,81 particularly those caused by Mycobacterium kansasii, as well as to invasive fungal infections, also has been documented.80 Other opportunistic infections that have been reported include legionnaires’ disease,82 toxoplasmosis,83 and Listeria monocytogenes infection.84 The milieu specific for this increased susceptibility to infections comprises granulocytopenia, monocytopenia, poor granulocyte reserve and abnormal mobilization,85 T-cell dysfunction,86 and decreased numbers of dendritic cells and antigen-presenting cells.87 Rarely, patients with HCL may have associated systemic immunologic disorders,88 including scleroderma and polymyositis89 and polyarteritis nodosa.90 HCL has been associated with other cutaneous lesions such as erythematous maculopapules91 and pyoderma gangrenosum.92,93 An associated coagulopathy manifested by factor VIII antibodies has been reported.94 Osseous involvement also has been described, primarily lytic lesions in the axial skeleton, usually the proximal femur.95,96 Rarely, osteolytic lesions may be associated with paraproteinemia.97 A rare case of HCL occurring with systemic mast cell disease has been reported.98 Pancytopenia is present in approximately 50% of patients with HCL at diagnosis; most other patients have suppression of one or two cell lines.3,55 Most patients with HCL have leukopenia, although 10% to 20% of patients exhibit a “leukemic phase” with a white blood cell count higher than 10,000 to 20,000/µL. Monocytopenia is a characteristic but often overlooked finding.1,3,55 Other laboratory findings include abnormal hepatic transaminase levels (19%), azotemia (27%), and hypergammaglobulinemia (18%), which rarely is monoclonal.3,97,99 Unlike in chronic lymphocytic leukemia, hypogammaglobulinemia is uncommon. The morphologic features of hairy cells are distinctive (Fig. 103-1). The neoplastic cells are one to two times the size of a small lymphocyte. The nuclei are round, oval, indented, or monocytoid; rarely, they appear convoluted.100 The nuclei are located in a central or eccentric position. The chromatin pattern is netlike, and nucleoli are indistinct or absent. The amount of cytoplasm varies, ranging from scant to abundant; a pale blue-gray color is characteristic. The cytoplasmic borders are irregular and exhibit fine, hairlike projections or ruffled borders. Occasionally, cytoplasmic granules are present. Rarely, the cytoplasm exhibits basophilia, or rod-shaped inclusions that correspond to ribosomal lamellar complexes, observed on ultrastructural examination in approximately 40% of cases.101 Examination of the bone marrow core biopsy specimen is critical in the diagnosis of HCL because of its characteristic histopathological appearance102–105 (Figs. 103-2 and 103-3). The bone marrow usually is hypercellular in most patients, but this finding may be variable. Hairy cell infiltration may be diffuse, patchy, or interstitial or a combination of these patterns. In patients with diffuse involvement, large areas of the bone marrow are replaced by hairy cells, with complete effacement of marrow in some patients. With patchy infiltration, small subtle clusters of hairy cells are present focally or scattered throughout the bone marrow. Unlike in lymphomas, the hairy cells do not form well-defined, discrete aggregates; instead, they merge subtly with the surrounding residual hematopoietic tissue. In the interstitial pattern of involvement, variable numbers of hairy cells infiltrate between normal hematopoietic cells and fat, with preservation of the overall bone marrow architecture. Hairy cell nuclei in biopsy sections are round, oval, or indented and widely separated from each other by abundant clear or lightly eosinophilic cytoplasm; rarely, the cells are convoluted or spindle shaped. The nuclear chromatin is lightly condensed, nucleoli are inconspicuous, and mitotic figures are rare or absent. Extravasated red blood cells often are seen, and blood lakes, similar to those observed in the spleen, also may be observed. Reticulin stains of the bone marrow trephine biopsy specimen in HCL show a moderate to marked increase in reticulin fibers. Normal hematopoietic cells usually are decreased in HCL; the number of granulocytes typically is more severely reduced than are erythroid precursors and megakaryocytes. In 10% to 20% of patients with HCL, the bone marrow is hypocellular. The hypocellularity may be severe,106 with a marrow appearance resembling that in patients with aplastic anemia. Historically, cytochemical demonstration of tartrate-resistant acid phosphatase (TRAP) activity has been used to confirm the diagnosis of HCL.107 TRAP-positive cells are found in most cases of HCL at diagnosis, although the percentage of positive cells varies greatly among patients. A positive TRAP stain in conjunction with characteristic histopathology is essentially diagnostic of HCL. Today, however, the routine use of immunophenotyping by flow cytometry for the diagnosis of chronic lymphoproliferative disorders has made reliance on the TRAP stain less important. Flow cytometric immunophenotyping is an essential part of the diagnostic evaluation, both to identify the characteristic immunophenotypic profile of HCL and to distinguish it from other chronic B-cell and T-cell lymphoproliferative disorders. Because hairy cells exhibit distinctive light scatter characteristics and immunophenotype, they can be identified even when present in very low levels (less than 1% of lymphocytes) in either the peripheral blood or bone marrow aspirate.108 This property is useful not only at the time of diagnosis but also after therapy to assess for residual disease.109 Hairy cells show bright CD45 expression with increased forward and side scatter resembling that of large lymphocytes or monocytes. They exhibit a mature B-cell phenotype and express one or more heavy chains and monotypic light chains. The numbers of cases with expression of kappa or of lambda light chains are approximately equal. Surface immunoglobulin is of moderate to bright intensity. Hairy cells strongly express pan–B-cell antigens, including CD19, CD20, CD22, and CD79b. They usually stain negatively for CD5, CD10, and CD23. They strongly express CD11c, CD25, and FMC7. CD103, an antigen expressed on mucosal T cells and some activated T cells, is expressed in a majority of cases of HCL.108,110 Approximately 35% of patients have a variant immunophenotype, but the hairy cells from such patients have the characteristic morphologic features of classic hairy cells and these patients have the same excellent response to treatment with purine analogs.111 Several B-cell–associated antibodies, including CD20, CD79a, and DBA.44, react with hairy cells in fixed, routinely processed tissue sections. Although these antibodies are not specific for HCL, they are useful in documenting the B-cell nature of the infiltrate and highlighting the extent of bone marrow infiltration at the time of diagnosis and after therapy.112–115 Clonal cytogenetic abnormalities are present in approximately two thirds of patients with HCL. Karyotype analysis is rarely required or useful to establish the diagnosis, however. The most frequently involved chromosomes include chromosomes 1, 2, 5, 6, 11, 14, 19, and 20. In particular, chromosome 5 is altered in 40% of patients, most commonly as trisomy 5, pericentric inversions, or interstitial deletions involving band 5q13.118–118 In rare cases, the diagnosis of HCL is made by histologic analysis of splenic tissue after splenectomy or splenic needle core biopsy. Splenic involvement in HCL is characterized by diffuse infiltration of the red pulp cords and sinuses, with atrophy or replacement of the white pulp. Blood-filled sinuses, lined by hairy cells, often are present but are not pathognomonic for HCL; they have been referred to as “pseudosinuses.”119 The liver shows both sinusoidal and portal infiltration by hairy cells. Involved lymph nodes commonly exhibit partial effacement, with hairy cells infiltrating the paracortex and medulla in a leukemic pattern. The leukemic cells often surround residual lymphoid follicles and extend through the capsule. A recent whole-exome sequencing study of HCL cells in parallel with normal cells has identified the presence of the BRAF V600E mutation in all of 48 cases of HCL.45 This finding has been extended and corroborated in larger cohorts of patients from different institutions using allele-specific or quantitative real-time polymerase chain reaction (PCR) assays. The BRAF mutation has now been reported in more than 400 cases of HCL and was not evident in more than 700 cases of other B-cell lymphoproliferative disorders.45,120–125 These data suggest that the BRAF V600E mutation represents a reliable molecular marker for diagnosis of HCL, and the BRAF mutational analysis will likely become part of the diagnostic armamentarium in HCL. However, a recent study reported the absence of the BRAF mutation in a subset of classic HCL, particularly HCL cases expressing immunoglobulin heavy variable 4-34 (IGHV4-34) immunoglobulin rearrangement.124 Therefore, as more information becomes available on the prevalence and functional role of BRAF mutations in HCL, the BRAF mutation analysis should be used in combination with cytomorphology and immunophenotyping to further improve and strengthen the diagnosis of patients with HCL. Considerations in the differential diagnosis for HCL include other chronic B-cell lymphoproliferative disorders associated with splenomegaly, including prolymphocytic leukemia, splenic marginal zone lymphoma, and hairy cell variant (Box 103-1). Patients with prolymphocytic leukemia typically have splenomegaly, but this disorder usually can be distinguished from HCL by the marked leukocytosis, the characteristic morphologic appearance of the prolymphocytes, and an immunophenotypic profile different from that for HCL.126–129 Splenic marginal zone lymphoma exhibits some clinical and morphologic features similar to those of HCL, but, in contrast, the bone marrow infiltrates are sharply demarcated from the surrounding normal tissue and intrasinusoidal infiltration often is prominent. In addition, the immunophenotypic profile differs from that for HCL, including negative staining for CD103.130–133 Hairy cell variant exhibits morphologic features that are intermediate between those of HCL and prolymphocytic leukemia. Unlike HCL, hairy cell variant is associated with prominent leukocytosis, lack of monocytopenia, and absence of CD25 expression.134–138 Finally, infiltrates of systemic mastocytosis in the bone marrow may resemble those seen in HCL. Immunohistochemistry studies, however, show the mast cells, unlike hairy cells, to be negative for B-cell antigens and positive for tryptase.139 Although cytomorphologic and immunophenotypic analysis along with clinical presentation can usually secure the diagnosis of HCL, the molecular analysis for the BRAF V600E mutation can be used to further improve the discrimination of HCL from HCL variant cases and other chronic B-cell lymphoproliferative disorders. HCL almost always has an indolent course, with some patients surviving 10 years without need for therapy.140 In a majority of patients, however, progressive disease eventually leads to complications resulting from anemia, bleeding, splenomegaly, or recurrent infections. Therapy is indicated when the patient has significant cytopenias; symptomatic organomegaly or adenopathy; repeated infections; or constitutional signs and symptoms such as fever, night sweats, or fatigue. Persistent blood cell counts showing an absolute neutrophil count less than 1000/µL, a hemoglobin value less than 11.0 g/dL, or a platelet count below 100,000/µL are guidelines that can serve as indications for therapy. Splenectomy was the first effective therapy for HCL and remained the initial treatment of choice until approximately 2 decades ago.11–14 After splenectomy, counts for all three cell lines return to normal in 40% to 70% of patients.13,141 This response is maintained for a median of 20 months in approximately two thirds of patients, and the overall 5-year survival rate is approximately 70%.141 No correlation has been found between spleen size and response to splenectomy. Splenectomy may have a possible role in an occasional patient to establish the diagnosis, in rare cases of splenic rupture, or in patients with life-threatening thrombocytopenia or a significant bleeding diathesis, because emergency splenectomy can lead to a rapid rise in the platelet count. Except in these very unusual circumstances, however, little, if any, role for splenectomy is recognized since the introduction of the purine analogs. Cytotoxic chemotherapy was given for the treatment of HCL before the advent of more effective therapies in the early 1980s. A variety of agents, including anthracyclines,142 alkylating agents (chlorambucil),143 and high-dose methotrexate,144 demonstrate activity. Combination chemotherapy, such as the CHOP regimen (cyclophosphamide, hydroxy doxorubicin [Adriamycin], vincristine [Oncovin], prednisone), produces long-lasting normalization of peripheral blood counts.145 In one report in the literature of successful syngeneic (identical twin) bone marrow transplantation, the patient remained free of disease at least 15 years later.146 Although HCL is sensitive to chemotherapy, significant myelosuppression and toxicity are associated with use of this modality. Therefore, conventional chemotherapy is now a therapy of only historical interest. Interferon was first reported in 1984 to be an effective therapy for patients with HCL15; since then, many large studies have confirmed its activity.15–21 The precise mechanism of action of interferon is not known, but its activity may be attributable to a decrease in the production of cytokines such as granulocyte colony-stimulating factor, granulocyte-macrophage colony-stimulating factor, interleukin-3, and interleukin-6, perhaps related to the characteristic monocytopenia associated with interferon treatment.147 Studies suggest that interferon-α results in apoptotic death of hairy cells, mediated by tumor necrosis factor-α.148 Despite a high overall response rate of 75% to 90%, most patients achieve only partial remission (i.e., they have a partial response [PR], defined as normalization of all peripheral blood counts).18,19 Interferon commonly is administered subcutaneously at a dose of 3 million IU/m2 three times a week for 12 to 18 months. During the first 2 months of treatment, the white blood cell count and hemoglobin level often decrease, occasionally precipitating transfusion. The platelets normalize earliest in responding patients, followed by the hemoglobin and the white blood cell count. An absolute neutrophil count greater than 1500/µL is achieved after a median of 5 months of therapy. The most common manifestations of toxicity include flulike symptoms, anorexia and fatigue, nausea and vomiting, diarrhea, dry skin, peripheral neuropathies, and central nervous system dysfunction, usually manifested as depression or memory loss. Other than myelosuppression, the most common laboratory abnormality is elevation of hepatic transaminase levels. The median failure-free survival period after discontinuing interferon therapy ranges from 6 to 25 months in different series.18–20,149 Patients with more than 30% hairy cells in the marrow or a platelet count less than 160,000/µL at the end of treatment have a higher risk of early relapse.20–20 In addition, patients who express the CD5 antigen appear to respond poorly to interferon.150 Patients can be maintained on long-term interferon therapy at a dose of 3 million IU subcutaneously given three times a week with minimal toxicity. Sixty percent of patients have sustained their initial response for a median of 5 years, 9% discontinued therapy early because of unexpected neurologic toxicity, and only 13% stopped therapy because of progressive disease.21 A recently updated study by Benz and colleagues confirmed the tolerability and efficacy of long-term therapy with interferon.151 In this study, 9% discontinued therapy because of progressive disease and 17% stopped therapy because of side effects. Although treatment of HCL with interferon is effective, complete responses are uncommon, and failure-free survival usually is short after discontinuation of treatment. Furthermore, the purine analogs have completely supplanted interferon for the treatment of newly diagnosed HCL. As early as the 1960s, Giblett and colleagues observed that 30% of children with severe combined immunodeficiency syndrome lacked the enzyme adenosine deaminase (ADA).152 It appeared that the accumulation of the triphosphorylated form of deoxyadenosine was responsible for lymphocyte depletion.153 Therefore, the deliberate inhibition of ADA was recognized as a potentially useful antileukemic strategy. The methods to accomplish this therapeutic effect included the development of agents to bind irreversibly to ADA or to resist the action of the enzyme. These agents affect both dividing and nondividing cells.154 After purine analog therapy, accumulation of deoxyadenosine triphosphates leads to DNA strand breaks and inhibition of DNA repair, which ultimately results in cell apoptosis. Pentostatin, or 2′-DCF, was the first agent to induce a significant number of complete responses in HCL.22,155 This drug binds to ADA, resulting in irreversible inhibition of the enzyme,156 which is found in all lymphoid cells and is important in purine metabolism. In most studies, complete response is defined by disappearance of hairy cells in the blood and bone marrow, complete normalization of peripheral counts (hemoglobin concentration > 12.0 g/dL, platelet count > 100,000/µL, and absolute neutrophil count > 1500/µL), and resolution of splenomegaly and lymphadenopathy. A partial response requires normalization of blood cell counts, greater than 50% reduction in hairy cells in the bone marrow, and greater than 50% reduction in splenomegaly. A number of studies demonstrate the efficacy of 2′-DCF in patients with HCL (Table 103-1).23–33 A large prospective, randomized study showed that the complete response rate and relapse-free survival rate are significantly better with 2′-DCF than with interferon.31 Various dosing schedules have been reported in early studies, but the current dose is 4 mg/m2 given by intravenous infusion every 2 weeks until maximum response. The median number of cycles required by patients until best response has ranged from 6 to 12 cycles.24,27,29,33 In one of the earlier studies conducted by the Eastern Cooperative Oncology Group, most patients achieved maximal response within the first 6 months.27 Therapy is relatively well tolerated; neutropenia, fever, and infections are the most frequent toxicities.25,27,32 One of the largest published series providing long-term evaluation was reported by the Southwest Oncology Group.25 A total of 241 patients received 2′-DCF on a phase III trial comparing interferon and 2′-DCF; 154 were randomly assigned to receive 2′-DCF initially, with crossover of 87 additional patients from the interferon group after it failed to produce improvement. Seventy-two percent of patients achieved a complete response with 2′-DCF. Long-term survival was not statistically different based on initial treatment; in both groups, overall survival was 90% at 5 years and 81% at 10 years (Fig. 103-4). With longer follow-up, 2′-DCF does not appear to be curative in all patients. Studies with follow-up periods longer than 5 years after treatment report relapses in 15% to 48% of patients.23–25,30 Table 103-1 Activity of 2′-Deoxycoformycin in Hairy Cell Leukemia CR, complete response; NA, not available; NR, no response; PR, partial response. Cladribine, or 2-CdA, is a purine analog that is resistant to the action of ADA. This agent accumulates in the lymphoid cells, possibly because they are rich in the enzyme deoxycytidine kinase.153 This enzyme phosphorylates 2-CdA to the active 5′-triphosphate form, creating a deoxynucleotide that cannot readily exit the cell. This compound inhibits ribonucleotide reductase, which results in decreased synthesis of deoxynucleotides. Both DNA synthesis and repair are impaired.
Hairy Cell Leukemia
Introduction
Epidemiology
Etiology and Pathogenesis
Clinical Presentation
Laboratory Evaluation
Differential Diagnosis
Treatment
Indications
Role of Splenectomy
Chemotherapeutic Approaches
Interferon
Purine Analogs
Pentostatin (2′-Deoxycoformycin)
Study
No. of Patients
Previously Untreated
Median No. (of Cycles)
CR (%)
PR (%)
NR (%)
Median Follow-up (mo)
Relapse (%)
Median Time to Relapse (mo)
Johnston et al.26
28
18
NA
89
11
0
14
4
13.8
Ho et al.28
33
0
NA
33.3
45.5
0
14.5
8
10
Rafel et al.32
78
35
7
72
16
1
31
33
29
Cassileth et al.27
50
19
6
64
20
16
39
14
CR: 13; PR: 31
Catovsky et al.29
148
23
9
74.3
22.3
3.4
42
8
22
Ribeiro et al.33
50
18
12
44
52
0
47
10
22
Grever et al.25,31
154
154
NA
76
3
5*
57
9
NA
Maloisel et al.23
238
67
9
83
16.6
6
63.5
15
NA
Kraut et al.30
24
NA
NA
100
0
0
82
48
30
Dearden et al.24
220
188
10
82
14
4
192
44
51.5
Cladribine (2-Chlorodeoxyadenosine)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Hairy Cell Leukemia






