China, Jiangsu Province had 9 counties. It was estimated that 120,000 cancer patients died in Jiangsu annually, accounting for 10% of overall cancer deaths in China, even though the population in Jiangsu Province only accounts for 5% of China national population. Since 1970’s, cancer has been ranked as the number one killer in Jiangsu Province. The top four cancer sites are cancers of liver, stomach, esophagus and lung, accounting for over 80% of all cancer deaths in Jiangsu Province.
and anti-oxidative properties that can inhibit various human cancer cell lines and also have no serious adverse effects. N-nitroso compounds formed in the human stomach have been implicated as etiological factors of stomach cancer. It is also suggested that Green Tea may inhibit HP infection.
January 1, 1995 and June 30, 1995 with pathologically confirmed diagnoses of stomach adenocarcinoma. Once the stomach cancer cases were diagnosed in the Endoscopic Unit, they were immediately interviewed by the interviewer at the hospital. We interviewed all incident patients with stomach cancer during the study period who consented to be interviewed with the following restrictions: patients must be newly diagnosed, not restricted by age, in stable medical condition as determined by their physician, and willing to participate. The study was restricted to those who lived in Yangzhong for at least one year. In the six-month study period, we recruited a total of 200 patients with esophageal or stomach cancer from the Endoscopic Unit. Of these, 67 patients with esophageal cancer were excluded. We had a total of 133 incident cases with stomach cancer in this study, which represented 80% of all new cases diagnosed in the same study period in Yangzhong (166 stomach cancer cases during the study period were estimated from the incidence of stomach cancer in Yangzhong during the six-month period in 1995). Blood specimens were collected in 63% (84 of 133) of stomach cancer patients who had an interview.
Table 20.1 Case-Control Studies of Green Tea and Stomach Cancer | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
approached 205 patients and interviewed 166 patients with chronic gastritis (81%) from the Endoscopic Unit. Of these, more than 95% were chronic atrophic gastritis cases. Blood specimens were collected in 88% (146 of 166) of patients with chronic gastritis who had an interview.
and no of those studies has demonstrated strong dose-response relationship 22, 25, 28, 31. The epidemiological evidence on green tea drinking and stomach cancer was still unclear at that time. We felt strongly to repeat our own finding on green tea drinking in a City near by Yangzhong. We selected Taixing City, which is across the Yangtze River from Yangzhong. In working with Professor Shun-Zhang Yu and Dr. Lina Mu of Shanghai Medical University School of Public Health, Drs. Hua Wang and Jinkou Zhao of Jiangsu CDC, and Dr. Baoguo Ding of Taixing CDC, We launched the second population-based casescontrol study in 2000 in Taixing City. The
major purpose of the study was designed as a second stage study to confirm the observation of green tea drinking and stomach cancer and to assess the possible interactions between green tea drinking and other risk/protective factors as well as molecular genetic markers. We have also decided to expend our study to three major cancer sites in Taixing, including cancers of the stomach, esophagus, and liver.
Table 20.3 The odds ratios (OR) and 95% confidence intervals of green-tea drinking variables and stomach cancer in Yang Zhong, Jiangsu, China, 1995 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 20.4 The odds ratios (OR) and 95% confidence intervals of green-tea drinking variables and chronic gastritis in Yang Zhong, Jiangsu, China, 1995 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 Explore Route of Transmission for Kala-azar
Explore Route of Transmission for Kala-azar
 A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
 Control and study of the first-time outbreak of angiostrongyliasis cantonensis in P.R. China
Control and study of the first-time outbreak of angiostrongyliasis cantonensis in P.R. China
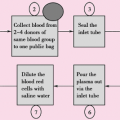 Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
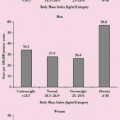 Blood Pressure, Body Mass Index and Risk of End-Stage Renal Disease among Men and Women in China
Blood Pressure, Body Mass Index and Risk of End-Stage Renal Disease among Men and Women in China
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


