have treatment delays extending their overall radiation treatment time6,7,8,9 or who have a prolonged interval between surgery and beginning their treatments. Intensifying the radiation dose delivery by treating “faster” is a method to compensate for accelerated tumor cell repopulation.
Table 30.1 Sampling of Trials with Impact on Current or Future Head and Neck Radiation Oncology Practice | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
chemotherapy. These studies established a favored recommendation (in patients deemed fit to receive cisplatin) for the use of concurrent chemotherapy with radiation in the postoperative setting for those patients with high-risk pathologic features including positive margins and/or ECS.
medical oncology, and radiation oncology is an important initial step in the evaluation of patients with head and neck cancer. In our clinics, patients meet with the radiation oncology nursing staff prior to beginning radiation to discuss management of toxicity, oral hygiene, and skin care. They are provided a booklet containing recipes for oral rinses, suggestions for skin care, and to address common questions.
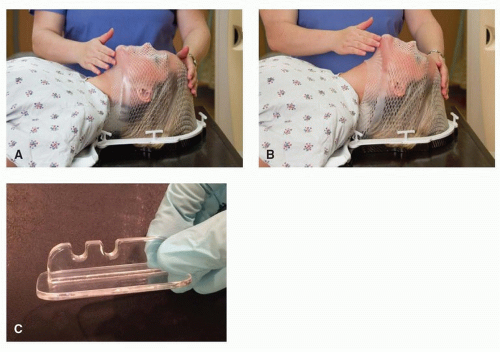 Figure 30.1. Patient setup. Patient immobilization and setup at the time of simulation is a critical step in the radiation treatment-planning process. A: Thermoplastic masks immobilize the patient with high reproducibility to minimize day-today variation in patient setup. B: Additional modifications that can be taken to position the patient include the use of different degrees of neck flexion. C: The use of bite blocks can provide spatial separation between critical structures and tumor. |
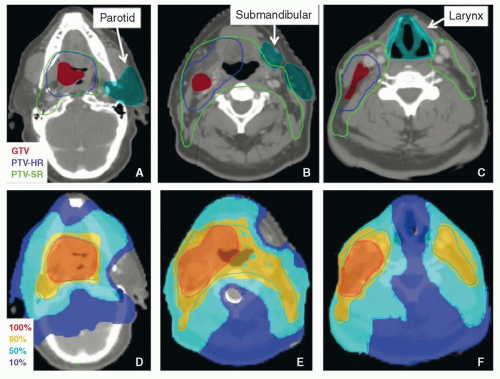 Figure 30.2. Representative IMRT plan for a patient with a T2 N2b M0 squamous cell carcinoma of the tonsil. Panels A to C show the delineated normal tissues and target volumes. Panels D to F show the isodose distribution from the IMRT plan. Note that the parotid, submandibular, and larynx are spared. (GTV, gross target volume; PTV-HR, planning target volume-high risk; PTV-SR, planning target volumestandard risk.) |
in quality assurance begins before the patient ever enters the radiation oncology workflow and continues until the treatment is completed (Table 30.2). Encompassing multiple steps in the process, quality assurance is performed to regulate and validate each step in the process with the ultimate goal of ensuring the accurate and precise delivery of radiation treatments.
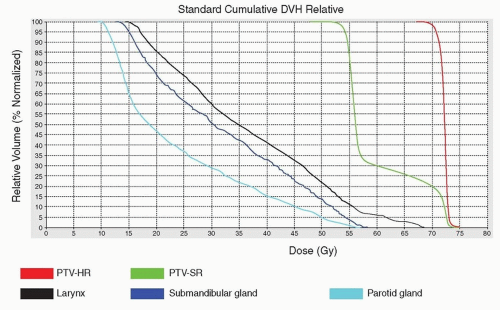 Figure 30.3. DVHs relate radiation dose to tissue volume. Graphical representation of dose to volume is provided by a DVH but do not provide spatial context as to the location of the dose within a given tissue. For most PTVs, more than 95% of the volume should receive at least 95% of the dose. Depending upon the normal structure, the median or maximal dose has greater relevance to potential toxicities. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


