4.1 Crohn’s Disease
4.1.1 Name of Disorder
Crohn’s disease, regional enteritis.
4.1.2 Clinical Definition
Chronic bowel inflammation secondary to an autoimmune reaction to intestinal tract affecting any region from mouth to anus.
4.1.3 How It Is Diagnosed
History, physical, and gastrointestinal histologic changes in conjunction with laboratory and radiology studies.
4.1.4 Nutritional Implications
Abdominal pain and diarrhea lead to poor oral intake, and inflammation leads to poor absorption, resulting in poor growth. Many nutrient deficiencies are common in patients with Crohn’s disease as well. Growth failure is found in 30% of Crohn’s disease patients at the time of diagnosis.
4.1.5 Pearls
- Growth failure is common in patients with Crohn’s disease, secondary to poor appetite, early satiety, poor absorption, and increased metabolic demand.
- Vitamin D deficiency is very common in children with Crohn’s disease. Supplementation is often required to assure proper intake, especially in the northern latitudes.
- Deficiencies of folate, calcium, and iron are quite common in patients with Crohn’s disease, as well as fat-soluble vitamins, vitamin B12, magnesium, copper, selenium, and zinc. It is important that all patients be supplemented with a multivitamin as well as calcium and iron if deficient.
- Permanent growth failure is not uncommon in Crohn’s disease, occurring in 19–35% of patients.
- Individuals on sulfasalazine and methotrexate should be supplemented with folic acid.
- Individuals who have Crohn’s disease who are not in flare-up are recommended to have a regular well-balanced diet without restriction.
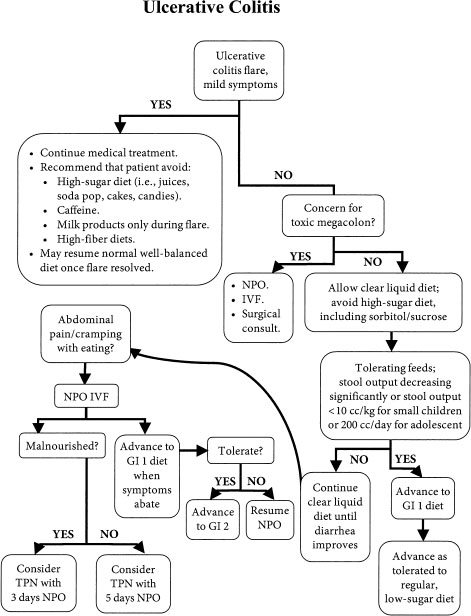
Nutritional Algorithm for Ulcerative Colitis
4.2 Ulcerative Colitis
4.2.1 Name of Disorder
Ulcerative colitis.
4.2.2 Clinical Definition
Chronic bowel inflammation secondary to an autoimmune reaction to the large intestine.
4.2.3 How It Is Diagnosed
History physical histology in conjunction with laboratory and radiology studies.
4.2.4 Nutritional Implications
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


