Temperature has long been used in clinical medicine and was included in the cardinal signs of inflammation described as “tumor, rubor, dolor, and fever.” The measurement of temperature by a thermometer, in the sublingual, subaxillary, or rectal locations, is not a clinical skill practiced regularly by doctors. In most cases, temperature is recorded by other health workers or by patients themselves. Normal body temperature is considered to be 37°C, the average core temperature for an adult population.
Temperature is tightly controlled within a narrow range in each individual. Fever is defined as any elevation in the core body temperature above the normal and results from the upregulation of body temperature. More commonly, a temperature >38°C is considered a clinically significant fever. In oncologic practice and many clinical studies, a significant fever is defined as a single temperature reading >38.5°C or three readings (at least an hour apart) of >38°C. The term fever (or pyrexia) of unknown origin, FUO (PUO), is used commonly, and often incorrectly, in the daily practice of medicine. An FUO is defined as an illness lasting at least 3 weeks with a fever higher than 38°C on more than one occasion and which lacks a definitive diagnosis after 1 week of evaluation in a hospital (1).
Fever is often accompanied by other symptoms, including sweating and rigors. Sweating, when it accompanies fever, is a cooling response by the body wherein heat is released from the body as it evaporates water on the skin’s surface. Rigors and shivering also contribute to temperature control and are rapid muscle spasms designed to increase heat production within the body. For adult humans and most large mammals, shivering is the major means of increased heat production in response to a cold environment. Nonshivering thermogenesis, a process involving heat production in brown adipose tissue, is important in the temperature control of infants.
CONTROL OF TEMPERATURE
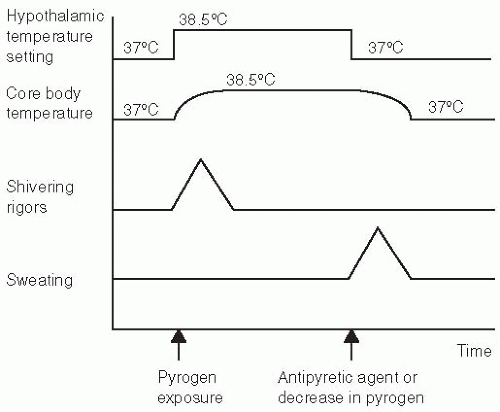
It is proposed that core body temperature is controlled by neurologic mechanisms centered in the anterior hypothalamus. The onset of fever in patients results from an elevation of the body’s regulated set-point temperature through a resetting of the temperature “gauge” in the hypothalamus (2). This may be caused by various drugs or by endogenous pyrogens. As a result of the reset hypothalamic temperature, the body increases the core body temperature to this new level (Figure 8.1) through shivering or nonshivering thermogenesis. The continued presence of pyrogen at the hypothalamus results in the maintenance of this higher temperature. Eventually, either as a result of a decrease in the quantity of pyrogen or the administration of an antipyretic, the hypothalamic temperature is reset to a lower or normal level. The core body temperature is therefore lowered through sweating. This control mechanism may be suppressed in patients administered steroids or anti-inflammatory agents. Older patients may not be able to mount the anticipated febrile response.
The endogenous pyrogens that are responsible for the onset of fever are largely derived from monocytes and macrophages. These cells, as a result of challenge by either endotoxin or infective sources, release tumor necrosis factor (TNF) and interleukin (IL)-1β. Their production is part of the complex cascade that results in the stimulation of other cytokines, such as IL-6, IL-8, and changes in prostaglandin metabolism. Serum levels of IL-6 and IL-8 have been found to correlate with core body temperature in patients with febrile neutropenia (3). The ultimate end point of this cascade is the activation of granulocytes, monocytes, and endothelial cells. Although fever appears to be associated with enhanced function of the immune system, it must nonetheless be noted that a direct connection between such phenomena and a beneficial effect of fever on outcome of infections has not been established. Fever, in fact, may be deleterious in the setting of autoimmune disorders or infections (4).
ETIOLOGY OF FEVER IN CANCER PATIENTS
Fever is commonly seen in patients with cancer, even in the absence of infection. The wide range of etiologies of fever in patients with cancer will be considered in relation to the pathophysiology of fever in these patients.
Tumor
Fever associated with tumor is believed to be associated with the release of pyrogens, either directly from a tumor or from tumor stimulation of immunologic mechanisms that cause an elevation in temperature through action on the anterior hypothalamus. The classic association of fever with particular tumor diagnoses relates more to tumors associated with a diagnosis of FUO (Table 8.1). In the combined results of six studies documenting the etiology of FUO, 23% of adults meeting the defined diagnosis were found to have malignancy as the cause (8% of children) (5). In another study of 111 elderly (age >65 years) patients with FUO, 26 had associated malignancy, with 15 patients diagnosed with lymphoma and 4 with renal cell carcinoma (6). Almost 7,000 cancer patients with fever were reviewed by Klastersky et al. and only 47 (0.7%) fit the diagnostic criteria for an FUO (7). Twenty-seven of the 47 patients had leukemia or lymphoma, with disease rather than infection being the cause of the fever in only 11. Tumor was responsible for fever in seven patients with widespread metastatic carcinomas; in six of these, large liver metastases were present.
Figure 8.1. Physiologic mechanisms associated with fever and accompanying symptoms. (Adapted from Boulant JA. Thermoregulation. In: Mackowiak P, ed. Fever: Basic Mechanisms and Management. New York: Raven Press; 1991: 1-22, with permission.)
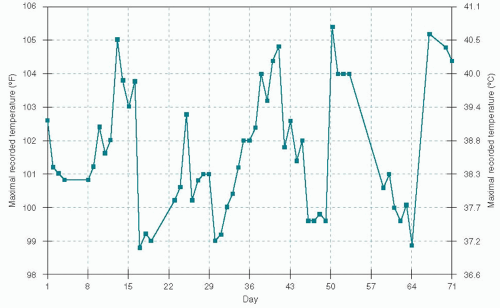
Hodgkin’s disease has classically been associated with the Pel-Ebstein fever (Figure 8.2), where a patient experiences 3- to 10-day cycles of fever alternating with periods of normal temperature (8). Although the presence of fever is an important prognostic indicator in patients with Hodgkin’s disease, there has been some discussion (9) about the value of Pel-Ebstein fever as a diagnostic tool particularly because the original description of the Pel-Ebstein fever was made in two patients who were subsequently found, on pathologic review, not to have Hodgkin’s disease.
TABLE 8.1 Tumors classically associated with fever
Hodgkin’s disease
Lymphoma
Leukemia
Renal cell carcinoma
Myxoma
Osteogenic sarcoma
Although classical teaching is that fever is associated with particular tumors, fever also occurs in patients with many of the more common cancers (Table 8.2). Forty-one percent of those who underwent autopsy had evidence of infection as an explanation of their fever (10). The incidence of infection among the autopsied patients was 50% for acute leukemia, 75% for lymphoma, and 80% for chronic lymphocytic leukemia. Infection was only found in a third of those with chronic myeloid leukemia, 17% of those with Hodgkin’s disease, and 15% of those with lung cancer.
Infection (Including Neutropenia)
Although infection and fever can be a common presentation in patients with cancer, it is of particular concern in patients with neutropenia. Neutropenia, defined as a peripheral blood neutrophil count of <500/µL, results from either increased destruction or decreased production of white blood cells. Decreased production by the bone marrow may result either from disease involving the marrow or from myelosuppression due to chemotherapy. The cause of fever is not identified in approximately 60% to 70% of patients with neutropenia (11). Risk factors for the development of fever in the setting of neutropenia have been identified and include a rapid decrease in the neutrophil count and a protracted neutropenia of <500 cells/µL or >10 days (12). Twenty percent of patients with 1 week of chemotherapy-induced neutropenia develop a fever and the rate of infection increases with lengthening periods of neutropenia. Other factors that may alter the risk of the patient with neutropenia include phagocyte function, the status of the patient’s immune system, and alterations in the physical defense barriers of the body (e.g., mucositis).
Fever and neutropenia in patients with cancer are associated with a high risk of medical complications, with a death rate ranging from 4% to 12%. Twenty-one percent of patients with febrile neutropenia at the Dana Farber Cancer Center developed serious medical complications (13). The investigators identified four risk groups for patients with febrile neutropenia. Group 1 consisted of inpatients at the time of onset of fever; group 2, outpatients who developed significant comorbidity within 24 hours of presentation; group 3, outpatients with uncontrolled cancer but without serious concurrent comorbidity; and group 4, outpatients without serious concurrent comorbidity and whose cancer was well controlled. The model was validated in 444 patients with febrile neutropenia, of whom 36% had a significant comorbidity, 27% had serious medical complications, and 8% died. Group 1 had the greatest risk and group 4 had little risk in relation to medical complications and risk (Table 8.3).
Figure 8.2. A 50-year-old man had fever, night sweats, and nonproductive cough for 10 weeks. He took antipyretic medications during the febrile periods. His wife recorded his temperatures, shown in the preceding text, on 56 of the 71 days. Biopsy of a rapidly enlarging cervical lymph node revealed nodular sclerosing Hodgkin’s lymphoma. The patient’s fevers and other symptoms promptly disappeared after the first cycle of doxorubicin, bleomycin, vinblastine, and dacarbazine. (From Good GR, Dinubile MJ. Images in clinical medicine. Cyclic fever in Hodgkin’s disease (Pel-Ebstein fever). N Engl J Med. 1995;332:436, with permission.)
TABLE 8.2 Incidence of fever without evidence of infection at autopsy in patients of different primary tumor types
Number of Patients with Fever Without Associated Infection
Primary Site
Number of Patients Observed
Number
%
Stomach
1,498
573
41
Kidney
208
39
19
Colon and rectum
113
75
66
Liver and gallbladder
98
43
44
Uterus
81
19
36
Squamous skin cancer
41
20
49
Esophagus
20
7
35
Breast
48
16
33
Lung
17
8
47
Small bowel
17
1
6
Prostate
11
7
64
Bladder
10
6
60
Bone
10
7
70
From Boggs DR, Frei E. Clinical studies of fever and infection in cancer. Cancer. 1960;13:1240-1253, with permission.
TABLE 8.3 Incidence of multiple medical complications and mortality in patients with febrile neutropenia as defined by risk
From Talcott JA, Siegel RD, Finberg R, et al. Risk assessment in cancer patients with fever and neutropenia: a prospective, two center validation of a prediction rule. J Clin Oncol. 1992;10;316-322, with permission.
An important component of this study was the identification of those patients at low risk for medical complication 24 hours after the onset of fever. Some of these low-risk patients developed medical complications (5%), but these either were transient and asymptomatic or were heralded by at least 7 days of medical deterioration and therefore readily detectable by appropriate follow-up. Two additional risk factors— a latency period of <10 days from the time of chemotherapy administration to the onset of fever and neutropenia and age >40 years—correlated with the occurrence of more frequent complications. Mucositis was associated with decreased risk of medical complications, suggesting that infection associated with mucositis may be responsive to antibiotics. The identification of a causative organism or positive blood cultures was not associated with increased risk. Talcott et al. then conducted a randomized controlled trial with usual care in hospital versus the same antibiotics at home based on these risk factors, but the study was closed early because of accrual difficulties (14). Five outpatients were readmitted to the hospital, but the number of major medical complications was not significantly different in the two arms. No patient died in either of the study arms and patient-reported quality of life was similar on both arms. The authors concluded that it is safe for clinicians to treat rigorously characterized low-risk patients with febrile neutropenia in suitable outpatient settings with appropriate surveillance for an unexpected clinical deterioration.
In a multinational study, a risk index score was developed to “stage” those patients with febrile neutropenia (15). Predictive factors included blood pressure, presence of chronic obstructive pulmonary disease or solid tumor, previous fungal infection in patients with hematologic malignancies, outpatient status, status of hydration, and age in relation to 60 years (Table 8.4) On the validation set, a Multinational Association for Supportive Care in Cancer (MASCC) risk index score >21 identified low-risk patients with a positive predictive value of 91%, specificity of 68%, and sensitivity of 71%. The authors went on to test their rules with low-risk patients treated with oral antibiotics after an initial observation period (16). Seventy-nine of 178 patients treated orally were discharged early, with only 3 having to be readmitted, a success rate of 96%.
This tool was further used to assess those deemed to have “apparent clinical stability.” However when used in this population, the tool had a low sensitivity in predicting those who may develop complications (17). However, the authors identified risk factors for the development of complications, which included a performance status >1, chronic bronchitis, chronic heart failure, stress hyperglycemia, a low monocyte count (<200 mm3), and stomatitis (>grade 1). It was suggested that clinicians should be cautious in sending home patients with febrile neutropenia, especially those with the above clinical findings.
On the basis of a number of retrospective studies, similar definitions of low risk have been applied to pediatric patients with fever and neutropenia (18). Low risk included evidence of bone marrow recovery in culture-negative patients who were afebrile for at least 24 hours and who had no other reason to continue intravenous antibiotics in the hospital. The control of any localized infection and the patient’s ability to return promptly in the event of fever or other complications were also necessary. In a prospective study of 70 patients who met these criteria and who were discharged home with neutropenia, none were readmitted with fever. Seven patients who were inadvertently discharged without evidence of marrow recovery were readmitted with recurrence of fever. Neutropenic children with positive cultures were also assessed to identify risk factors for bacteremia (19). Of the cases of bacteremia, 92.5% occurred in those where cancer was not controlled, were <1 year of age, <10 days past their last chemotherapy, and had no evidence of marrow recovery.
TABLE 8.4 Multinational Association for Supportive Care in Cancer scoring index
Characteristic
Score
Burden of illness: no or mild symptoms
5
Burden of illness: moderate symptoms
3
Burden of illness: severe symptoms
0
No hypotension (systolic BP > 90 mmHg)
5
No chronic obstructive pulmonary disease
4
Solid tumor/lymphoma with no previous fungal infection
4
No dehydration
3
Outpatient status (at onset of fever)
3
Age < 60 years
2
Scores ≥21 are at low risk of complications.
Points attributed to the variable “burden of illness” are not cumulative. The maximum theoretical score is therefore 26.
Two studies reported that hypotension and bacteremia in the setting of neutropenia are significant risk factors for prolonged hospitalization (>7 days) and high mortality. Malik et al. (20) reported, from Pakistan, a mortality rate of 82% associated with febrile neutropenia in patients presenting with shock and a study from France reported that patients admitted to an ICU with febrile neutropenia experienced a 54% 30-day mortality, with a higher mortality in those with respiratory and renal failure (21). While a number of clinical characteristics may provide prognostic information regarding the outcomes of hospitalized patients with febrile neutropenia, predictive models are needed to better identify high-risk patients who may benefit from the addition of adjunctive colony-stimulating factors (CSFs).
Organisms (Bacteriology)
A basic understanding of the classification and sensitivities of the different organisms is essential to understand the infection in patients with cancer. Over time there have been changes in the underlying organisms associated with febrile neutropenia as evidenced by progressive studies by the European Organization for Research and Treatment of Cancer (EORTC) (22). Gram-negative organisms were the leading cause of infection in patients with febrile neutropenia, but their incidence decreased from 71% of identified causative organisms during the 1973 to 1978 period to 31% during the 1989 to 1991 period. Infection by one of these gram-negative organisms—Pseudomonas aeruginosa—became a driving force in the selection of antibiotics. However, the incidence of pseudomonas infection also decreased as reflected by an incidence of only 0.1% of febrile neutropenic cases at the National Cancer Institute (23). The incidence of both acute and chronic fungal infections increased, with up to 33% of patients with febrile neutropenia not responding to a week of antibiotic therapy having a systemic fungal (Candida or Aspergillosis) infection (24).
The incidence of gram-positive organisms increased from 29% during the 1973 to 1978 period to 69% during the 1989 to 1991 period, requiring a review in treatment regimens used in patients with febrile neutropenia. Some of these gram-positive organisms, such as coagulase-negative staphylococci or Corynebacterium jeikeium, represent indolent infections that were methicillin resistant and only susceptible to vancomycin, quinupristin-dalfopristin, and linezolid. Other gram-positive bacteria such as Staphylococcus aureus, viridans streptococci, and pneumococci may cause fulminant infections with serious complications and possibly death if not treated promptly. Gram-negative bacilli, especially P. aeruginosa, Escherichia coli, and Klebsiella species, remain prominent causes of infection and must be treated with selected antibiotics as recommended by the Guidelines of the Infectious Disease Society of America (IDSA) (25). This was supported by a single cancer center review of the cause of bacterial infections in low-risk, febrile neutropenic patients (26). Among microbiologically documented infections, monomicrobial, gram-positive infections accounted for 49% (with coagulase-negative staphylococci the most frequent); monomicrobial, gram-negative infections accounted for 36% (with E. coli the most frequent); and 15% of infections were polymicrobial.
Location
Infections can occur throughout the body and need to be sought carefully through history and examination. Collapse, consolidation, and superimposed infection may develop behind an obstructing bronchial tumor. Aspiration pneumonia may occur in those with esophageal tumor either secondary to an obstruction or as a result of a tracheoesophageal fistula.
The gastrointestinal system is the most common site of indigent organisms that cause infection in patients with neutropenia. Clostridium difficile infection may present with fever and diarrhea and must be considered in those who are already taking antibiotics. Fungal and viral infections of the esophagus need to be suspected in those with dysphagia and odynophagia. Anaerobic infections may be a factor in severe mucositis or gingivitis and in those patients with perianal discomfort. Spontaneous bacterial peritonitis may be a cause of fever in patients with ascites. A urinary catheter increases the risk of urinary tract infection as does the presence of urinary obstruction, but the presence of asymptomatic bacteriuria in a catheterized patient without neutropenia is not usually an indication for antibiotic treatment.
Central nervous system infections can be difficult to diagnose and usually require lumbar puncture to confirm. Infection is the most common complication of Ommaya reservoirs, used to administer intraventricular chemotherapy, and is more likely to occur in those with previous radiotherapy or in whom repeated surgical procedures have been necessary (27). Most infections are due to Staphylococcus epidermidis and can usually be successfully treated with antibiotics (28).
Particular attention to sites of recent surgery is essential in assessing infection. Surgical collections may include infected hematomas that develop following surgery. The skin is also a common site of infection that may range from infected decubitus ulcers to herpes zoster infections. The use of percutaneous catheters in oncology has created another portal for the introduction of infection in patients with cancer. Of a total of 322 indwelling devices placed in 274 patients with cancer by a single surgeon, device-related sepsis occurred in 28 of 209 patients (13%) with catheters and 6 of 113 patients (5%) with subcutaneous ports (29). Triple lumen catheters were associated with a higher rate of thrombosis but not of infection. The complications of 1,630 venous access devices for long-term use in 1,431 consecutive patients with cancer were reviewed (30). Of the catheters inserted, 341 of 788 (43%) had caused at least one device-related infection compared with 57 of 680 (8%) of the completely implanted ports (P = 0.001). The number of infections per 1,000 device days was 2.77 for catheters compared with 0.21 for ports (P = 0.001). The predominant organisms isolated in catheter-related bacteremia were gram-negative bacilli (55%) compared with gram-positive cocci (65.5%) in port-related bacteremia. Patients with solid tumors were less likely to have device-related infectious morbidity compared with patients with hematologic cancers. Updates on reducing the risk of infections from intravascular devices have been provided by the Center of Disease Control (CDC) (31).
Only gold members can continue reading. Log In or Register to continue