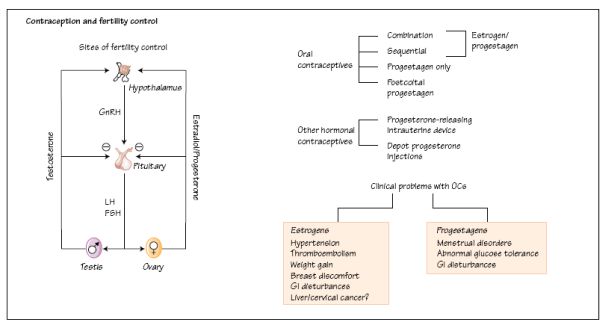
There are many oral contraceptive preparations on the market and a choice should be made to prescribe the one with the lowest estrogen and progesterone concentrations that give good cycle control. Combined oral contraceptives (COCs) can also be used to treat a number of gynaecological conditions involving irregular cycles, menorrhagia or dysmenorrhoea. In addition to progesterone only pills (POPs), intrauterine devices which release progesterone locally to the endometrium are available (Mirena Intrauterine Systems, Schering Health) and are used both for contraception and for the treatment of endometriosis and other painful disorders of menstruation.
COCs are contraindicated in women who are pregnant, or who have a history of various forms of cardiovascular disease, cerebrovascular problems, certain liver disorders and undiagnosed gynaecological problems. COCs influence blood coagulation and there is a small increased risk of deep vein thrombosis, pulmonary embolism, stroke and myocardial infarction. This is slightly higher in women taking COCs containing third- generation progestagens (desogestrel, gestodene), particularly when there are other risk factors such as obesity, smoking and older age (>35 years). COCs should not be prescribed to women with known clotting abnormalities or a history of hemiplegic migraine. Side-effects should be monitored including regular blood pressure readings.
Oral contraception is fertility control using orally active synthetic sex hormone derivatives (Fig. 30a).
Combined oral contraceptives
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


