TABLE 15-1 SITES FOR ARTERIAL BLOOD SAMPLING OR CANNULATION | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
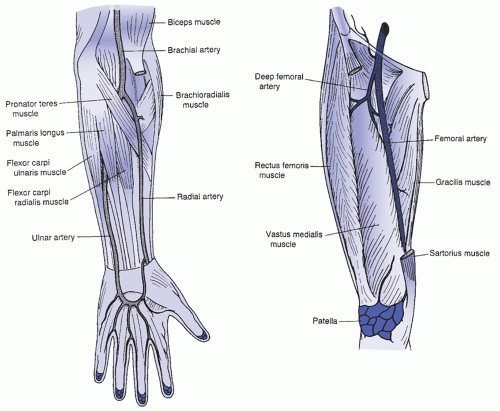 FIGURE 15-1 Location of radial, ulnar, and brachial arteries (left) and location of the femoral artery in the leg (right). |
 PATIENT SAFETY
PATIENT SAFETY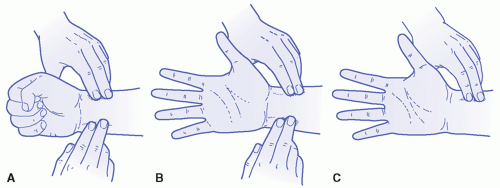 FIGURE 15-2 Performing Allen test to determine circulatory adequacy. A: The patient clenches the fist while nurse applies pressure to both the radial and ulnar artery. B: The patient opens the hand and nurse noting the pallor of the palm surface, releases the ulnar pressure releases pressure while watching to see how long it takes for the hand to color (signifying circulation and patency of vessels). C: Evaluating pulse and blood return. |
Determine if the oxygen status of the patient has been altered only for the blood sampling. If so, resume presampling status as soon as the blood sample is drawn.
Maintain pressure dressing long enough—usually between 10 and 20 minutes depending on the access site—to prevent excessive seepage of blood into the tissue. Be sure that the pressure dressing is not so tight that blanching occurs or that venous blood flow in the hand is severely restricted.
If the patient is receiving anticoagulation therapy, apply digital pressure. Digital pressure is also preferable to the use of a C-clamp at the femoral site because significant occult bleeding into the retroperitoneal space can occur rapidly and may result in unnecessary blood loss and discomfort for the patient.
Remove pressure dressing after bleeding stops.
The artery is located and kept between two fingers held in a “V” pattern, allowing pulsation to be felt on both fingers laterally but at the same time allowing enough room between them for the needle entry. The syringe and needle are held almost straight down. When the puncture is made in this manner, care must be taken not to pierce through the other wall of the artery. The acronym “NAV” (nerve, artery, vein) can assist the practitioner in focusing on the right femoral puncture location by remembering the nerve innervating the leg is to the left of the stick, the artery is central, and the vein is in the direction of the pubis symphysis.
Vessel entry may be performed with the same techniques used for a radial artery puncture. Two or three fingertips are placed along the direction of the femoral artery to the left over the ilium, and the syringe and needle are held at an angle no higher than 90 degrees. This method must be used for femoral artery catheter placement due to the need to manipulate more equipment; if used for a one-time needle and syringe sample, there is less chance of artery perforation using this approach.
 EVIDENCE FOR PRACTICE
EVIDENCE FOR PRACTICE
A heparinized syringe
A plain syringe for withdrawal of dilute heparin from the injection port
A syringe with dilute heparin solution for flushing the catheter after drawing the blood sample
of shock; and, at the same time, to draw arterial blood for ABG measurement and other sampling.
TABLE 15-2 KEY INTERVENTIONS: POSTARTERIAL CATHETER INSERTION CARE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
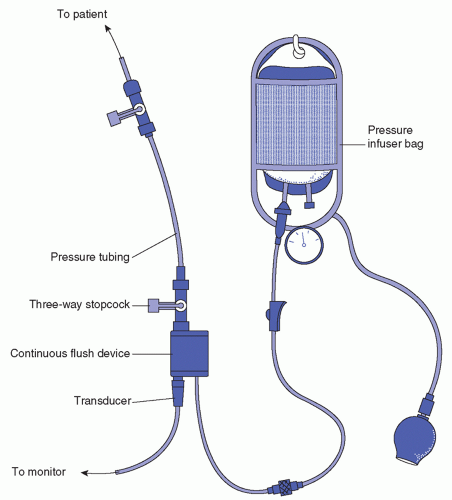 FIGURE 15-3 Cable and transducer setup. |
practices should be used to reduce nosocomial infection rates. Thorough hand hygiene before catheter insertion and maintenance of aseptic technique during setup of the system, during insertion, and during all manipulations of the line are mandatory. Use of observation monitoring and checklist compliance to sterile technique and practitioner insertion methods have been incorporated into line insertion practices in hospital settings to enhance sterile insertion and reduce infection rates of invasive lines.
TABLE 15-3 MALFUNCTIONS OCCURRING IN ARTERIAL PRESSURE MONITORING | ||||
|---|---|---|---|---|
|
partial pressure of oxygen in arterial blood (PaO2) is in the normal range between 80 and 100 mm Hg and when SaO2 ranges from 93% to 100% (Horne & Derrico, 1999; Tortora & Grabowski, 2003). Under normal resting conditions, blood contains 20 mL oxygen per 100 mL blood. Of that, 97% (19.4 mL) is attached to hemoglobin of the red blood cells, and 3% (0.6 mL) is dissolved in the plasma (Margereson, 2001). If the PaO2 is high, more oxygen is able to bind with hemoglobin; the converse is also true. It is important to interpret SaO2 and PaO2 values in relation to the amount of supplemented oxygen the patient is receiving. The alveolar-arterial gap is the difference between the mean alveolar PaO2 and the measured arterial PaO2. The alveolar PaO2 is always higher than the arterial PaO2. Elevations in the gap indicate a ventilation perfusion imbalance in the lungs and inadequate diffusion of oxygen to carbon dioxide at the pulmonary blood supply.
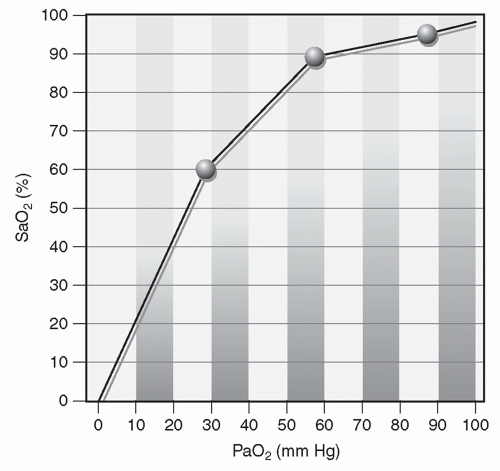 FIGURE 15-4 Oxyhemoglobin dissociation curve. Normally, PaO2 and SaO2 values are closely related. When PaO2 decreases slightly, so does SaO2. However, when PaO2 drops below 60 mm Hg, the close association is disrupted. The disruption is represented graphically as the oxyhemoglobin dissociation curve, which illustrates the relationship between PaO2 and SaO2 values known as the 30-60-90 rule. When PaO2 measures 30 mm Hg, SaO2 is usually 60%, and when PaO2 is 60 mm Hg, SaO2 is usually 90%. (Adapted from Horne, C., & Derrico, D. (1999). Mastering ABGs: The art of arterial blood gas measurement. American Journal of Nursing, 99(8), 26-33.) |
pH
Respiratory function
Metabolic function
Electrolytes + metabolites
pH
Respiratory function—three core measurements (PaCO2, PaO2, and SaO2)
Metabolism function—two core measurements (bicarbonate, HCO3− and base excess, BE) noting whether each aspect of one to three as normal, low, or high to baseline ranges
Is compensation occurring (compare pH with respiratory and metabolic function)? If so, which direction is the change?
Note electrolytes + metabolites
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


