Depression is not a normal response to or consequence of chronic or acute illness.
Depression may be a side effect of medications used to treat other chronic conditions; when in doubt try a substitute medication or discontinue it briefly.
Symptoms of depression in the elderly may differ from those in younger adults and often present as physical complaints.
The elderly are at greatest risk for depression related to significant changes, such as moving to a new environment or experiencing bereavement or losses in their life.
Men are far less likely to admit depression than are women, and doctors are less likely to suspect it in men.
The presence of an understandable reason for depression should not mitigate the need for treatment.
Minor depression and dysthymia should be treated in elderly patients.
The risk of suicide increases over age 65. More women attempt suicide, but men are four times more likely to complete a suicide.
Treat an initial episode of depression for at least 6 months, and monitor proactively for subsequent relapse.
Depression can be a chronic condition and lifetime treatment with antidepressants should be considered after two or more occurrences.
Depression is one of the most common, significant, and unrecognized health problems of advancing age, and fortunately one of the most treatable. It affects up to 10% of older adults seen in primary care, with community studies showing up to 25% of the elderly reporting symptoms of depression.1 Depression is underdiagnosed in the elderly; however, only an estimated 20% to 50% of those with depression are diagnosed across a broad range of care settings.2 Many factors contribute to the underdiagnosis of depression, including a widespread belief that depression is a normal response to aging, disability, or serious illness. Depression, however, is not a normal part of aging or illness, and if left untreated it is often associated with severe morbidity or mortality, functional impairment, poor quality of life, increased health care costs, and a great deal of potentially preventable human suffering.3
Depression in clinical settings is likely overlooked in part, because of the many competing demands that occur during a clinic visit, where other conditions and needs vie for the limited available time. Physicians typically focus on established chronic diseases, presenting symptoms, or preventive care measures. Depression and mental health issues are often seen as secondary concerns that will be addressed only as time allows. The effects of depression, however, are not limited to emotional symptoms but instead intersect with every aspect of a patient’s life, including their physical, emotional, and mental well-being. Depression may exacerbate the severity of many other medical illnesses, lead to poor adherence to medication, and amplify somatic symptoms associated with other chronic conditions.4 By treating depression, physicians improve their ability to help patients manage comorbid chronic conditions and improve quality of life.
The elderly are particularly at risk for depression because of the many changes and losses associated with the process of aging. Elderly patients who are experiencing depression are more likely to seek help from their regular primary care physician than from a mental health specialist. Older adults are often reluctant to discuss emotional problems or difficulties, and may resist referral to mental health providers, partly because of social stigma related to mental health disorders. Depression may be seen by the patient or associates as a sign of weakness in character and failure to manage one’s life. Elderly patients, however, most often have long-standing and trusting relationships with their physicians, who they may hold in high esteem. With appropriate encouragement from their physician, more elderly patients may accept treatment for depression and a referral to a mental health clinician when needed.
DEPRESSION DEFINED
Depression is a widely experienced human psychological and emotional reaction to social and interpersonal circumstances, characterized by sadness, disappointment, frustration, unhappiness, or despair. Feelings such as sadness or frustration may occur frequently in relation to stress related to day-to-day work, home situations, or other factors. However, when such feelings become overwhelming, pervasive, increase in intensity and frequency, impair functioning, and last for >2 weeks, a diagnosis of depression should be seriously considered along with appropriate treatment options.5
Depressive disorders are classified along a continuum, with variations in their degree of persistence and severity of symptoms; from short-term, minor or subclinical depression or elation, to severe delusional depression or delirious mania. Specific disorders include major depression, minor or subsyndromal depression, dysthymia, seasonal affective disorder (SAD), and atypical depression. Depression combined with mania often signifies bipolar disorder, whereas cyclothymia represents a milder form of bipolar disorder.5 Depression with mania can be quite complex to treat and manage, and is usually best referred to a mental health specialist or team of mental health providers. The referring physician can then work collaboratively with the mental health provider to rule out other possible medical problems that might cause or exacerbate an episode of depression with mania, such as dementia or medication problems (see section “Differential Diagnosis”).
Major Depression
Major depression is defined as at least 2 weeks of a depressed mood or loss of interest in usual activities, accompanied by at least four additional symptoms from the list in Table 17.1.6 A wide range of symptoms may be present with a major depressive disorder including feelings of sadness, irritability, or tension; loss of interest or pleasure in most activities or hobbies; anorexia or hyperphagia; hopelessness and the inability to envision a future; change in sleeping patterns including insomnia, early morning waking, or too much sleep; difficulty concentrating and making decisions; and thoughts of suicide or death. In extreme cases, patients can exhibit psychotic symptoms, with severe impairment in social and personal functioning, loss of contact with reality, and delusions.
Elderly patients also often present with physical complaints, such as persistent headaches, stomachaches, or chronic pain, and they may be reluctant to discuss emotional concerns.7 Elderly patients may also show impaired memory and disorientation not related to illness or disease, or may show an exaggerated indifference or apathy to their surroundings.
TABLE 17.1 CRITERIA FOR MAJOR DEPRESSION
Present for at least the previous 2 wk and represent a change from previous functioning
Must include either symptom 1 or 2 and four or more additional symptoms
Depressed mood—reports feeling sad or empty nearly every day
Loss of interest or pleasure in all, or almost all, activities (anhedonia)
Change in appetite or weight (either gain or loss when not dieting)
Sleep disturbances (nearly every day—insomnia most common)
Restlessness, agitation, or being slowed down (observable by another)
Fatigue or loss of energy (nearly every day)
Feelings of worthlessness or guilt (nearly every day—not just self-reproach or guilt over being sick)
Difficulty thinking, concentrating, or making decisions (nearly every day, by self account or observed by others)
Recurrent thoughts of death or suicidal ideation with or without plans or attempts
Major depression often begins insidiously and therefore can be difficult to diagnose. There can be a prodromal period that lasts for weeks to months with minor depressive symptoms or anxiety. An episode of major depression can last for 6 months or longer. Major depression tends to be recurrent or chronic, with more than 50% of people who experience one episode of major depression eventually experiencing another.
Minor Depression
Minor depression, also called subsyndromal or subthreshold depression, differs from major depression in the degree of severity and number of symptoms present. Minor depression is thought to be far more common among the elderly than major depression and is often precipitated by physical health problems and stress.8 There is currently no firm agreement on diagnostic criteria for minor depression—it is often seen as clinically relevant depression that does not fulfill the diagnostic criteria for major depression.9,10 Minor depression, however, can still have significant health and personal consequences for the elderly, with recent research indicating that even mild chronic depression can impair immune response in older adults and is associated with increased risk of death.11,12
Dysthymia
CASE ONE
Mrs. A. visited her doctor every other month with persistent complaints of low energy, sleeping problems, various aches and pains, and poor appetite. Although a workup years earlier had revealed no physical causes for her problems, at that time, her doctor suggested increased exercise and social activity. Mrs. A. continued with complaints about her husband and children, and felt that no one cared for her. She would lament her inability to go out to activities, and then focus on how poor her health was. Mrs. A.’s husband confided to her doctor that she had always been “a sort of depressed person” who was unwilling to do anything about it but complain.
Mrs. A. probably has dysthymia. Dysthymic disorder is defined as a chronically depressed mood that occurs for most of the day and for most days over at least 2 years. It is far more prevalent in women than in men. The symptoms are the same as those for other depressive disorders, but especially include poor appetite or overeating, insomnia or excessive sleepiness, low energy or fatigue, poor self-esteem, poor concentration and difficulty making decisions, and feelings of hopelessness. Dysthymia is very similar to minor depression in that it is a milder version along the continuum of mood disorders, with less severe symptoms, both in degree of severity and number of symptoms present.
The difference between dysthymic disorder and minor depression is that dysthymia is a chronic long-term condition, which often begins in early life. It was previously called depressive personality, because of the long-term course and features that include low self-interest and self-criticism, with the dysthymic person often seeing himself or herself as uninteresting and incapable.6 People with dysthymic disorder can also experience episodes of major depression at some time in their life.
Seasonal Affective Disorder
SAD is not a specific diagnosis in itself, but rather a term used to add additional specification to an identified depressive disorder, and can be part of either unipolar or bipolar depression. It indicates that the depression is related to temporal or seasonal changes that occur at particular periods of the calendar year. It is believed that these changes are related to the changing patterns of dark and light, because in most cases the disorder begins in the fall or winter and then recedes with spring. It is far more prevalent in higher latitudes and winter seasons, with younger people and women the most at risk. A diagnosis of depression with seasonal pattern can be made if patients report a regular relationship between the onset and improvement of depression and a particular time of year (unrelated to seasonal psychosocial stressors) for at least 2 years.
Bipolar Disorder
Bipolar disorder, also called manic depressive illness, is characterized by cyclic mood changes, alternating between the highs of mania and the lows of depression. Mood changes can be dramatic and rapid or mild and gradual. Mania is characterized by excessive elation, unusual irritability, decreased need for sleep, grandiose notions, increased talking, racing thoughts, increased energy and sexual desire, poor judgment, and inappropriate behavior.7 Left untreated, it can progress to a psychotic state. Episodes of mania can result in serious consequences for the patient with bipolar disorder and his or her family. Manic behavior often leads to unwise financial decisions, social embarrassment, and deteriorating family relationships.
Bipolar depression is a recurrent disorder, and over 90% of people experience multiple episodes.6 It is thought to have a strong genetic component, but all members of a family with genetic predisposition to the disorder will not develop it. Environmental factors such as stress and life circumstances often appear to trigger the onset of bipolar disorder, or lead to episodic relapses that sometimes require hospitalization. Bipolar disorder most often represents a long-term chronic illness and is usually best managed by mental health specialists with appropriate experience and expertise.
DIAGNOSING DEPRESSION
There are no specific laboratory tests or findings that are diagnostic of depression, despite the fact that a number of neurotransmitters that produce chemical changes in the brain are the source of depressive symptoms. These neurotransmitters include norepinephrine, serotonin, acetylcholine, dopamine, and γ-aminobutyric acid. Because we cannot measure these changes directly, a diagnosis of depression is instead made through assessment and interview, using standardized screening criteria to assess symptoms of depression and potential causes, and then using the standard diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) to determine the presence or absence of specific depressive disorders.6
The U.S. Preventive Services Task Force (USPSTF) now recommends “screening adults for depression (Evidence Level B) in clinical practices that have systems in place to assure accurate diagnosis, effective treatment, and followup.”13,14 The task force notes that the benefits of screening and treatment are unlikely to be realized unless such clinical systems are in place. The recommendations for screening and diagnosis presented here are based on the assumption that the physician has such systems in place to assure consistent management and follow-up of depression in elderly patients. Follow-up and management over time are key to successful treatment of depression in the elderly (see section “Treatment of Depression”).
Assessment may be best regarded as a two-stage process, with (a) a brief screen for the two primary symptoms of depression and (b) a more extensive screening process for depression if the brief assessment is positive (Evidence Level B). This two-stage process saves time during brief clinic visits, identifying those who may require more in-depth evaluation for both major and minor depressive disorders.15 It is also important to remember during the screening process that the expression of depressive symptoms among the elderly is often strongly influenced by cultural norms and expressions and may vary dramatically across cultures. A complete assessment for diagnosing depression should include the components listed in Table 17.2 (Evidence Level C).16
TABLE 17.2 ASSESSMENT FOR DEPRESSION
A brief screen consisting of two questions related to depressed mood and loss of pleasure
If the screen is positive, a full assessment using standardized criteria or a standardized depression screening instrument
Review of the medical history to rule out and treat symptoms that may be related to ongoing chronic medical conditions or past history of depressive episodes
Review of medications to rule out side effects of current medication use
An assessment of current mental, physical, and functional status to rule out the development of new conditions such as dementia, delirium, thyroid disorders, or anemia
Assessment of psychosocial concerns such as recent bereavement, alcohol use, or significant changes in the social environment
Assessment of suicide risk
Signs and Symptoms of Depression
Two major symptoms canbe used as criteria to screenfor the presence of depression in adults: (i) A frequently depressed mood, and (ii) a loss of pleasure or interest in most or all activities (anhedonia). One or both of these symptoms must be present for at least 2 weeks to meet the criteria for a diagnosis of major depression. These questions are incorporated in the Patient Health Questionnaire 2 (PHQ2) and can be used as a formal instrument for this purpose (see Table 20.4).17 The PHQ2 questions are drawn from a larger scale, and can also be used for screening for depression (see Table 17.3). Physicians may best incorporate these two questions into practice by making them part of the rooming system in which nurses ask them as part of vital sign collection. A positive response to either question should prompt the physician to ask additional questions about other symptoms of depression.
There are nine symptoms commonly associated with depression (including the two mentioned above) and are considered the gold standard for diagnosing depression. These symptoms are listed as the diagnostic criteria for depression in the DSM-IV.16 For a diagnosis of major depression, at least five of the nine symptoms must be present for at least 2 weeks, and must include symptom 1 or 2 from the list (Table 17.1). For a diagnosis of minor depression, at least two, but less than five of the symptoms should be present for at least 2 weeks and represent a change from previous functioning; one of the symptoms must be either symptoms 1 or 2 from the list (see Table 17.1).
TABLE 17.3 STANDARDIZED SCREENING INSTRUMENTS FOR DEPRESSION IN THE ELDERLY
Instruments
Type of Response Format
Long Form Number of Questions
Short Form Number of Questions
Minutes to Fill Out
Note
Patient Health Questionnaire (from the PRIME MD)
Ordinal
9
2
5-10
Developed from the DSM-IV symptoms list for ease in office administration—good validity and reliability18
PHQ9—long version
PHQ2—short version
Geriatric Depression Scale (Brink 1982)
Yes/no
30
15
8-10
Good reliability, specificity, and sensitivity with the elderly
Center for Epidemiologic Studies Depression Scale (NIMH)
Ordinal
20
10
8-10
Adequate reliability and validity; can generate high false-positives
Beck Depression Inventory (Beck, 1961)
Ordinal
10
10-15
Good reliability and validity; high sensitivity, but low specificity
The Self-Rating Depression Scale (Zung, 1965)
Ordinal
20
10-15
Adequate reliability and validity; focuses on frequency rather than severity of symptoms
PRIME MD, Primary Care Evaluation of Mental Disorders; PHQ, Patient Health Questionnaire; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders Fourth Edition; NIMH, National Institute of Mental Health.
Symptoms of depression in the elderly may also vary from those in the general adult population, creating difficulty in the assessment process. Elderly patients often focus on physical symptoms as their presenting complaint (e.g., headaches, stomach, or bowel problems). This often leads to other tests to rule out physical causes of depression. The presence of multiple unexplained physical symptoms is highly suggestive of the presence of depression. Elderly patients may also agree that they are depressed, but blame their depression on physical conditions such as pain from arthritis or back pain. Older patients may also present with apathy or a severe lack of motivation; in this case, careful assessment is indicated to rule out other causes such as dementia, pseudo dementia, or a new condition such as anemia. Additional symptoms that may be present in the elderly are included in Table 17.4.
Cultural Considerations
Each culture has unique forms of expression to communicate feelings; this is particularly true in the expression of symptoms related to mental health problems. How patients express and communicate depressive symptoms will be strongly influenced by what are acceptable expressions of depression within their culture. The DSM-IV notes that patients may refer to problems related to their “nerves” (Latino), or “weakness” or “imbalance” (Asian), or heart or being “heartbroken” (Middle Eastern cultures).6 Cultures will also differ in how seriously depression is viewed, presenting significant treatment issues. When cultural differences are present between the patient and the physician, it is particularly important to listen to and question patients carefully, and to express in clear medical terms why treatment of depression is important.
TABLE 17.4 ADDITIONAL SYMPTOMS THAT MAY BE PRESENT IN THE ELDERLY
Increased somatic complaints—headaches, stomach problems, pain (unrelated to a known physical cause)
Apathy toward environment
Diminished self-care
Irritability
Confusion (unrelated to illness or dementia)
Psychomotor retardation
Distractibility
Hopelessness, the inability to envision a future
Screening Tools
There are many standardized screening tools available to assess the symptoms of depression, some of which can be used in primary care settings with older adults. Screening tools for depression vary in length and response criteria; the more complex the screen, the more difficult it will be to use with the elderly. Many instruments have also been modified as short forms that are easier and less time-consuming to complete. Table 17.3 contains a brief overview of validated screening tools that can be self-administered in primary care settings as part of the intake or rooming processes. Other screening tools for depression that are used primarily for research or that must be administered by a mental health practitioner are not included here.
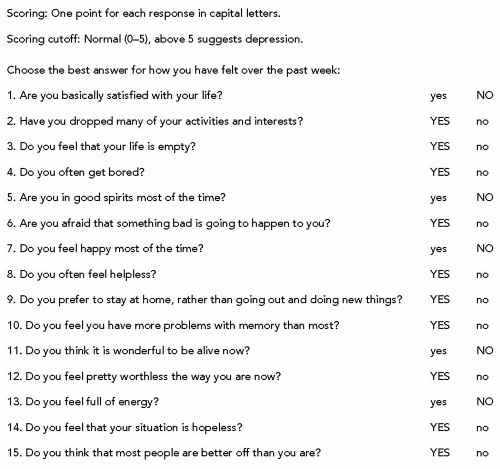
Figure 17.1 The Geriatric Depression Scale—Short Form.
There has been some question in the literature as to whether standard instruments for assessing depression take into account features such as sleep disturbance or weight loss that may occur in the elderly as a result of the normal effects of aging rather than from depression per se. The Geriatric Depression Scale (GDS) is the only instrument from the list in Table 17.3 that is specifically designed to assess depression in the elderly; the instrument does not rely on somatic symptoms and is simple and clear in ease of administration. The GDS has been found to perform just as well as other measures of depression, with good reliability and validity (see Fig. 17.1).19
Screening instruments can be helpful in clinical practice if they are short, reliable, can be self-administered, and are readily available when needed. Focusing on a two-stage screening system that incorporates a brief two-question screen into regular clinical practice has many benefits. First, even if depression is not present, it provides an opening for the patient to talk about their mental health concerns. Many elderly are reluctant to discuss emotional concerns, but may be willing if a trusted physician raises the question first. Second, the brief screen will clarify who needs more in-depth assessment for depression, rather than spending time during limited visits on a more extensive screening process, especially with the elderly who are likely to have many physical concerns that need to be addressed. The brief screen also demonstrates to patients on a regular basis that good mental health is as important as good physical health. Finally, a brief assessment done regularly may identify many of the estimated 50% of cases of depression that go unrecognized in clinical practice every year.20
Diagnosis
Once a screening test for depression is positive, further questioning will be needed to establish a diagnosis and determine whether a treatment course is needed. The diagnosis is based not only on the number of symptoms present, but also on the degree of persistence and severity, and the change represented in the patient’s ability to function in his or her daily life. For a diagnosis of major depression, five of the nine symptoms listed in Table 17.1 must be present for the past 2 weeks and must include the two primary symptoms of depressed mood and anhedonia. The episode should also be accompanied by clinically significant distress, or impairment in other important areas of functioning and should represent a change from previous functioning for the patient.
For a diagnosis of minor depression, two to four of the symptoms listed in Table 17.1 should be present for at least 2 weeks and represent a change in previous functioning, with one of the symptoms being either depressed mood (symptom 1) or anhedonia (symptom 2). The distinguishing feature between minor depression and dysthymic disorder is chronicity, with dysthymia characterized by a chronically depressed mood that occurs for most days over a period of at least 2 years.
The standard ICD-9 code that has long been used in primary care settings for a diagnosis of depression is the code 311 (depression not otherwise specified). This code does not distinguish between major and minor depression or dysthymia, nor does it specify recurrence or additional features, as is the case with ICD-9 coding using the DSM-IV. There has been some movement in recent years toward more accurate coding of major depression using the DSM-IV code 296.xx for major depression. Unless the physician can clearly distinguish between major and minor depression and dysthymia, the standard ICD-9 coding of 311 is recommended.
Differential Diagnosis
Once a diagnosis of depression is made, a review of the patient’s medical history and current medications should be conducted to rule out other causes of depressive symptoms. Serious medical conditions can be primary or secondary to depression, with some symptoms of medical conditions mimicking symptoms of depression, including problems with sleep, changes in appetite, or changes in normal energy levels (see Table 17.5). A review of past episodes of depression will help in clarifying recurrent or chronic depression. Major depression is recurrent or chronic in at least 50% of people and a past history of depression should guide treatment decisions for the current episode.
TABLE 17.5 DIFFERENTIAL DIAGNOSIS FOR DEPRESSION
Depressive Disorders Related to Other Medical Conditions
Taxonomy of Primary Depressive Disorders
Conditions that are Primary Causes of Depression (Correct Underlying Cause)
Depression Secondary to a Medical Condition (293.83) (Treat Symptoms)
aSee DSM-IV for further clarification of depressive disorders.
bMany chronic medical conditions are associated with depression, especially those conditions resulting in significant physical symptoms and/or associated with significant life changes.
NOS, not otherwise specified.
Only gold members can continue reading. Log In or Register to continue