Fig. 8.1
Classification of tumor depth for superficial esophageal cancer. Ep epithelium, lp lamina propria, mm muscularis mucosae, m mucosa, sm submucosa, mp muscularis propria, ad adventitia (from Ancona et al. 2008)
In addition, skip metastases as an intraesophageal spread of tumor cells in submucosal lymphatics are frequently observed in esophageal cancer (Cheng et al. 2013). This influences the target volume, too, with an increasing likelihood from pT1 tumors (about 4 %) to pT4 tumors (about 30 %). It should also be regarded that a metachronous or even synchronous secondary cancer of the upper aerodigestive tract can occur in up to 10 %.
This tumor behavior has major implication on the target volume of definite and preoperative radiotherapy as well. On the other hand, patient’s status and comorbidities should be taken into account, not to unnecessarily increase the risk of side effects by unjustified enlargement of the target volume. It is not yet proven if elective nodal irradiation is reasonable (Zhao et al. 2010).
As a basis for treatment planning, the classification of the Japanese Society for Esophageal Diseases may be used (Table 8.1), although only very recent publications with detailed prescription of lymph node spread refer to this terminology (Cheng et al. 2013) (Table 8.2).
Description of LN position | Numbering (Japanese) | Numbering (RTOG) |
|---|---|---|
Superficial cervical | 100 (right, left) | |
Cervical paraesophageal | 101 (right, left) | |
Deep cervical | 102 (right, left) | |
Peripharyngeal | 103 (right, left) | |
Supraclavicular | 104 | 1 |
Upper thoracic paraesophageal | 105 | |
Middle thoracic paraesophageal | 108 | 8 (middle) |
Lower thoracic paraesophageal | 110 | 8 (lower) |
Recurrent nerve | 106 rec | |
Pretracheal | 106 pre | |
Aortopulmonal | 5 | |
Paratracheal superior | 2 (right, left) | |
Paratracheal inferior | 4 (right, left) | |
Tracheobronchial | 106 tbL (left) | 10 (right, left) |
Bifurcational | 107 | 7 |
Main bronchus | 109 (right, left) | |
Supradiaphragmatic | 111 | 15 |
Posterior mediastinal | 112 | 3 |
Ligamentum arteriosum Botallo | 113 | |
Anterior mediastinal | 114 | 6 |
Cardiac | 1 (right), 2 (left) | 16 |
Lesser curvature | 3 | |
Greater curvature | 4 | |
Left gastric artery | 7 | 17 |
Common hepatic artery | 8 | 18 |
Splenic artery | 11 | 19 |
Celiac artery | 9 | 20 |
Table 8.2
Prediction of lymph node status according to infiltration depth (positive lymph nodes in %)
First author | Pat. No. | T-stage | Histology | |
|---|---|---|---|---|
AD | SCC | |||
Ancona et al. (2008) | 27 | 1 m | 0 | 0 |
71 | 1sm1 | 8.3 | 12.5 | |
1sm2 – 3 | 42.9 | 50 | ||
Bollschweiler et al. (2006) | 16 | 1 m | 0 | 0 |
44 | 1sm1 | 22 | 33 | |
1sm2 | 0 | 17 | ||
1sm3 | 78 | 69 | ||
Siewert et al. (2008) | 1002 | 1 m | 0 | 22 |
1sm1 – 3 | 18 | 22 | ||
2 | 67 | 50 | ||
3 | 85 | 74 | ||
4 | 89 | 79 | ||
Gockel et al. (2011) | 289 | 1sm1 | 6 | 27 |
340 | 1sm2 | 23 | 36 | |
601 | 1sm3 | 58 | 55 | |
Hölscher et al. (2011) | 70 | 1 m | 0 | 0 |
101 | 1 sm1 | 9 | 29 | |
1sm2 | 13 | 27 | ||
1sm3 | 43 | 76 |
In principle, the direction of lymphatic flow is primarily directed to the upper mediastinum and cervical region in patients with suprabifurcal tumors and to the lower posterior mediastinum and celiac axis in patients with infrabifurcal tumors. Tumors located at the level of the tracheal bifurcation tend to metastasize in both directions (Cheng et al. 2013). It should be considered that, especially in squamous cell carcinoma of the esophagus, even very early cancer (T1sm1) may infiltrate lymphatic vessels and disseminate into regional and distant lymph nodes (a detailed recommendation is presented in Table 8.4). Lymphographic studies and histopathological specimen indicate a lymphatic pathway from the lower esophagus upward into the mediastinum and also downward along the celiac axis (Fig. 8.2).
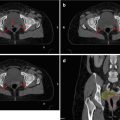
Fig. 8.2
Spread of esophageal cancer into regional lymph nodes: cervical cancer infiltrates predominantly in cranial direction and lower mediastinal cancer to the lower posterior mediastinum and celiac axis. Tumors at the level of the tracheal bifurcation metastasize in both directions
8.3 Target Volume Definition in Trials and Guidelines
The guidelines and recommendations of radiation therapy have been extremely simple in the vast majority of former clinical trials. While the length of treatment portals, later the length of the target volume, has been described just by two numbers in former trials – margins between 3 and 5 cm above and below the primary – it became nowadays obvious that an optimization of radiation therapy besides an improvement of surgery and further escalating the combinations of chemo- or targeted therapies is essential. Only by optimizing the locoregional control, making the risk of regional tumor recurrences by far less than 40 %, cure can be achieved. On the other hand, normal tissue sparing especially in multimodality concepts is a prerequisite. Therefore, in modern trials, precise definitions of clinical target volumes and dose-volume constraints are standard (Table 8.3).
Table 8.3
Definition of clinical target volume (CTV) in recent clinical trials (without cervical esophageal cancer) and guidelines
First author | Tumor | Oral margin (CTV) (cm) | Aboral margin (CTV) (cm) | Axial margin (CTV) (cm) | Further recommendations |
|---|---|---|---|---|---|
Stahl et al. (2009) | AEG 1-2 | 5 | 3 | 2 | All positive LN with 1 cm margin |
Elective nodal irradiation (No. 1, 2, 3, 7, 8, 9, 11) | |||||
Mean dose kidney < 15 Gy | |||||
Mean dose liver < 17 Gy | |||||
Crosby et al. (2013) | SCC and AEG 1-2 | 2 | 2 | 1 | No nodal irradiation |
V20 lung < 25 % | |||||
V40 heart < 30 % | |||||
Tomblyn et al. (2012) | SCC and AEG 1 | 5 | 5 | 1 | All positive LN with 2 cm margin |
Elective nodal irradiation for upper (No. 104) and for lower mediastinal cancer (No. 9) | |||||
Wang et al. (2012) | SCC | 3 | 3 | 0.8 | V20 lung < 30 % |
V30 lung < 18 % | |||||
Dmean heart <45 Gy | |||||
CALGB 9781 | SCC and AEG 1 | 5 | 5 | 2 | Elective nodal irradiation in upper (No. 104) and in lower mediastinal cancer (No. 9) |
French FFCD 9102 | SCC and AEG 1 | 3 | 3 | 2 | Elective nodal irradiation in upper (No. 104) mediastinal cancer |
SAKK 75/08 | SCC and AEG 1-2 | 3.5 | 3.5 | 1 | All positive LN |
Elective nodal irradiation in upper/middle (No. 105, 108) and distal esophageal cancer (No. 9) | |||||
NCCN (2013) | SCC and AEG | 3–4 | 3–4 | 1 | All positive LN with 0.5–1.5 cm margin |
Elective nodal irradiation in cervical (No. 101, 102, 103,104), upper and middle mediastinal cancer (No. 104, 105) and AEG I (No. 110, 9, 3)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|