Renal cell cancer (RCC) is increasingly diagnosed at an early stage in many countries, which likely contributes to the recent leveling of RCC mortality in the United States and many European countries. However, over all stages nearly 50% of the patients die within 5 years after diagnosis. Smoking and obesity may account for approximately 40% of all incidental cases in high-risk countries. Besides obesity, rising prevalence of hypertension may play a growing role. Several other occupational and lifestyle factors may also affect the risk of RCC. Genetic variations may be an important factor in the differing incidence among populations.
More than 90% of kidney cancers arise in the renal parenchyma, and the remainder in the renal pelvis. Most cancers in the parenchyma are renal cell carcinomas (RCC), a heterogeneous class of tumors arising from different cell types within the nephron with a clinical course ranging from indolent to highly aggressive. Advances in our understanding of the genetics underlying the pathogenesis of renal cell neoplasms have led to a histopathologic classification into several subgroups, of which “clear-cell” histology is the most common (75%–80%). As the increasing incidence of RCC observed for the past several decades in most parts of the world cannot fully be explained by the increasing availability of medical services and the use of novel sensitive imaging procedures, an increase in the prevalence of etiologic risk factors must also play a role.
Descriptive epidemiology
It is difficult to obtain clear population-based patterns of incidence and mortality from RCC because population data from different regions are presented for RCC and renal pelvis cancer combined. Hence, kidney cancer in this section, unless otherwise specified, includes cancers of the renal parenchyma and renal pelvis.
Incidence
The global incidence of kidney cancer increased from the 1970s until the mid 1990s, then leveled out or decreased in many countries. In 2008, kidney cancer was estimated to afflict about 270,000 individuals worldwide, accounting for more than 2% of all malignant diseases. In the United States annual incidence rose by 2.6% per year between 1997 and 2007, and it was estimated that more than 58,000 men and women would be diagnosed in 2010. Kidney cancer was the seventh (4% of total cancer) leading malignant condition among men and the eighth (3%) among women in the United States in 2010. In the United States incidence rates are somewhat higher among the black than among the white population. RCC is more common in men than in women; male to female ratios are generally between 1.5:1 and 2.5:1. The incidence rates are highest in the sixth and seventh decades.
Globally, the incidence of kidney cancer varies more than 10-fold between populations and geographic areas ( Fig. 1 ), suggesting that lifestyle factors may play major role in the difference in incidence across the continents. The highest rates are found in North America, Europe, and Australia, and the lowest in Asia. Moreover, genetic variations among populations may play a role. The increasing incidence observed for past decades in almost all areas and the geographic differences in incidences may also be explained in part by increased use of novel diagnostic imaging methods such as ultrasonography and computed tomography (CT). The widespread use of these imaging procedures has led to an increase in diagnosis of incidentally detected RCCs, which tend to be at a lower stage and more likely localized than symptomatic.
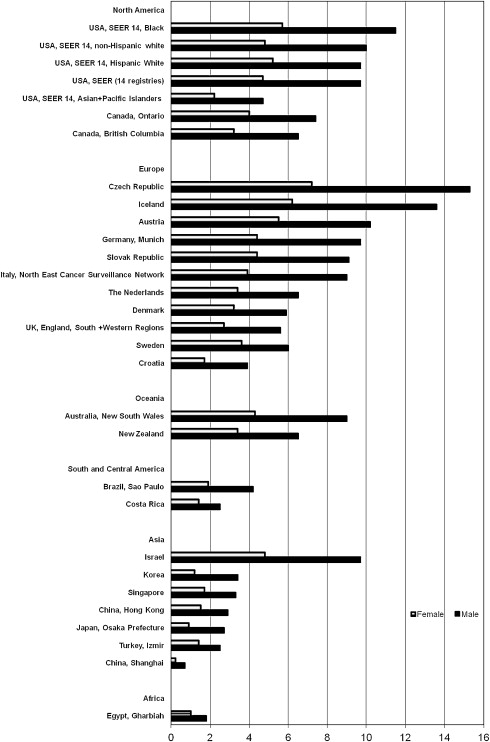
Incidence rates for RCC in the United States have been rising steadily for more than 3 decades, more rapidly among African Americans than Caucasians. In the United States also, RCC incidence differs among racial and ethnic populations (see Fig. 1 ). A recent study reported overall increased incidence rates (2.39%), mainly due to a remarkable increase in the incidence of localized RCC (4.29%) from 1988 to 2006. The incidence of distant stage decreased over time but those of regional spread remained unchanged. This finding strongly indicates changes in the diagnosis of RCC compared with earlier diagnoses in recent years.
In Europe there have been regional differences in rates and trends over time, with high rates remaining in several countries in central and eastern Europe, whereas in Sweden over the last decades there have been decreases in rates, with stable rates in Denmark. In other northern European countries, except for the United Kingdom, incidence rates have tended to decrease or stabilize.
Mortality
Trends in mortality from kidney cancer have reflected trends in incidence, but with a smaller increase over time in the past decades. The worldwide mortality rates of kidney cancer were estimated to be 116,000 in 2008, which is 1.5% of all cancer deaths. Similar to incidence, mortality varies considerably between regions. Among women, mortality rates were in general about half those of men.
In Europe, death rates increased until the early 1990s and thereafter declined or stabilized. In general, the decreases were larger in men of middle age in western European countries. Nevertheless, in the early 2000s there was a greater than threefold difference in kidney cancer mortality within Europe, with high rates remaining especially in the Czech Republic and Baltic countries and the lowest rates in Greece, Spain, Portugal, and Romania.
In the United States it was estimated that 13,000 deaths from kidney cancer occurred in 2010, making it the tenth most common death in malignancy among men. Death rates were highest among American Indians and Alaska Natives. Between the mid-1970s and mid-1990s, kidney cancer mortality increased despite the increasing proportion of localized, incidentally detected tumors; this could in part be the result of increase in all stages including advanced disease. The diagnosis of RCC with smaller tumors and at an earlier stage probably has contributed to the recent plateauing in mortality seen in the United States and also in many European countries.
However, in a recent analysis of RCC cases diagnosed from 1988 to 2006 based on 17 registries from the Surveillance Epidemiology and End Results (SEER) database, the overall estimated age-adjusted rates increased annually by 0.78% where mortality rates for localized RCC increased by 3.16%, but those with regional and distant RCC decreased by 0.46% and 0.53%, respectively, over time. Together this could imply that thus far it has not been shown that early treatment is efficacious. Moreover, the decreased mortality in advanced RCC could in part be due to improvement in the treatment for advanced stages.
Survival
Relative survival rates for kidney cancer are higher in the United States than in Europe. From 2000 to 2002, for data from 47 European cancer registries (EUROCARE-4), the mean 5-year relative survival for kidney cancer was 55.7% compared with 62.6% from 13 United States SEER registries. In the Nordic region relative survival has been increasing in all countries from 1964 to 2003.
In the United States, the 5-year relative survival rates increased from 1983 to 2002 across all stages. In a new report reevaluating SEER data including RCCs diagnosed from 1988 to 2006, 5-year relative survival for RCC of all stages increased from 63.7% in 1988 to 73.9% in 2002. For localized disease, survival rates increased from 91.7% in 1988 to 92.8% in 2002 whereas the rates remained unchanged for regional (63.7% to 64.2%) and metastatic disease (12.1% to 11.9%) over time. This improvement in survival confined to localized disease may reflect the effect of lead-time bias, due to earlier diagnosis than in the past and also detection of indolent, nonlethal tumors with new imaging techniques.
Risk factors
Tobacco Use
Cigarette smoke, containing a wide range of carcinogenic compounds including polycyclic aromatic hydrocarbons, aromatic amines, heterocyclic amines, and N -nitrosamines, can both initiate and promote tumor development in animals. Cigarette smoking is also one of the well-established risk factors for RCC. According to The International Agency for Research on Cancer (IARC) there is sufficient evidence to define tobacco smoking as a cause of RCC. A meta-analysis of 24 (19 case-control and 5 cohort) studies reported a relative risk of 1.38 (95% confidence interval 1.27–1.50) for ever-smokers compared with lifetime never-smokers. Men had a 54% and women had a 22% increased risk for RCC. There was also a dose-dependent increase in risk related to the number of cigarettes smoked per day. Smoking cessation for more than 10 years may reduce the elevated risk attributable to smoking.
Anthropometric Measures
Overweight, especially obesity, is another well-established risk factor for RCC in both women and men. According to a meta-analysis of 17 epidemiologic studies, a 5-unit increase in body mass index increases risk for RCC by 24% in men and 34% in women. Later studies also supported the positive association in both genders. Most studies found a dose-response relationship with increasing body mass index. Waist circumference and waist-hip ratio provide an estimate of abdominal or central obesity, a powerful contributor to metabolic abnormalities such as insulin resistance and hyperinsulinemia. In a few studies, waist circumference or waist-hip ratio was positively associated with RCC risk, as was weight gain or loss. The proportion of all cases of RCC attributable to overweight and obesity has been estimated to be about 40% in the United States and up to about 30% in European countries. There is still an unexplained stronger association in women than in men.
The mechanisms by which obesity influences renal carcinogenesis are not clear, but several plausible although speculative explanations exist. For example, sex steroid hormones may affect renal cell proliferation and growth by direct endocrine receptor-mediated effects, by regulation of receptor concentrations, or through paracrine growth factors such as epidermal growth factor. Further, obesity is related to several endocrine disorders such as decreased levels of sex hormone-binding globulin and progesterone, anovulation, insulin resistance, and increased levels of growth factors such as insulin-like growth factor 1 and high circulating levels of leptin. Lower adiponectin levels have also been observed among RCC patients than in healthy controls. There is also some evidence that link obesity, inflammation, and development of insulin resistance.
Adult height is a complex variable because of its multiple determinants, including genetic, nutritional, and health-related factors. Most, but not all studies have found a positive association between height and risk of RCC.
Physical Activity
Because energy expenditure is an important determinant of adult weight and obesity, a role of physical activity in renal carcinogenesis is plausible. The impact of occupational and/or recreational physical activity on the risk of RCC has been reported in several case-control and cohort studies. Some of the studies found that either occupational or recreational physical activity was associated with reduced risk of RCC. It remains unclear whether the association is independent of obesity.
Foods
Meat intake has been hypothesized to elevate risk for RCC, presumably because of its fat and protein content. Besides these nutrients, products in cooked meat such as heterocyclic amines, polycyclic aromatic hydrocarbons, and in cured meat nitrites and nitrates may mediate the renal carcinogenic process. Studies suggest an association between fried, processed, or barbecued meat and RCC risk. A meta-analysis of 13 case-control studies found a positive association between consumption of poultry, processed meat, red meat, and all meat and RCC risk, with 20% to 30% elevated risk among those in the highest compared with the lowest intake category for each of the meat groups. Later case-control studies also supported the positive association between red meat intake and RCC risk. By contrast, a recent pooled analysis of 13 prospective studies from North America and Europe found no association between intakes of red meat, processed meat, poultry, or seafood and RCC risk, nor did a large prospective European study.
Fruits and vegetables contain antioxidant nutrients and other dietary factors that may reduce RCC risk. Several case-control studies found a protective effect of vegetables and/or fruits, often strong for vegetables, especially the dark green and cruciferous varieties. A pooled analysis of 13 prospective studies also found an inverse association between fruit and vegetable consumption and RCC risk. However, in the large prospective European study, no associations between consumption of fruits and vegetables, except root vegetables, and RCC risk were observed.
Neither coffee nor tea drinking has been conclusively associated with RCC risk, although a pooled analysis of 13 prospective studies found an inverse association with both coffee and tea.
Two studies have examined dietary pattern and RCC; one study found an inverse association with “drinker pattern” (wine, hard liquor, beer, and snacks) and the other found a positive association with high-fat and high-protein diets.
Nutrients
Fat and protein intake and RCC risk has been examined in several case-control studies, some of which found a positive association. However, a recent pooled analysis of 13 prospective studies from North America and Europe found no association between intakes of fat and protein or their subtypes and RCC risk. On the other hand, antioxidant nutrients including carotenoids, vitamin C, and vitamin E have been associated with reduced risk of RCC. A pooled analysis of 13 prospective studies found an inverse association between β-carotene intake and RCC risk.
Alcohol
Although alcohol intake is related to elevated risk of several cancer sites such as oral cavity, esophagus, and breast, several case-control studies, a pooled analysis of 13 prospective studies, and a large European study consistently found an inverse association between alcohol consumption and RCC risk. Overall, evidence is convincing that alcohol intake does not increase but most likely reduces risk of RCC, perhaps through enhancement of insulin sensitivity and risk of diabetes.
Hypertension and Antihypertensive Medications
History of hypertension has been consistently associated with an elevated risk of RCC. There is indeed sufficient evidence that hypertension is an independent risk factor for RCC. Use of antihypertensive medications including diuretics and nondiuretic antihypertensive medications has also been associated with elevated risk of RCC. However, these data likely reflect confounding by indication rather than a causal association. As suspected, some studies reported that the association with hypertensive medications disappeared once hypertension was accounted for and high blood pressure was associated with an increased risk also among men and women who never took antihypertensive medications. The association between risk of RCC and hypertension has also been shown to be independent of obesity. The biological mechanism for the association between risk for RCC and hypertension is not known.
Other Medical Conditions
End-stage renal disease
The incidence of RCC in patients with end-stage renal disease developing acquired cystic kidney disease has been reported to be elevated compared with the general population. An increased risk has also been seen in native kidneys after renal transplantation. While proliferation of proximal tubular epithelial cells has been identified as the major pathogenic mechanism of cyst formation, hormones (eg, estrogens), growth factors, and their receptors may stimulate cell proliferation and promote carcinogenesis. This mechanism may also explain, in part, the onset of multiple renal adenomas and bilateral carcinomas that develop in patients with acquired cystic kidney disease.
Diabetes mellitus
Most case-control studies found either no increased risk with diabetes or an excess risk confined to women. Few cohort studies exist, but some reported a significantly increased incidence of RCC among diabetic patients. However, diabetes may not be an independent risk factor because of its strong relation to obesity and hypertension. Elevated levels of growth factors and growth factor receptors may mediate the possible relationship between diabetes and RCC.
Chronic hepatitis C infection
One recent prospective study found that chronic infection with hepatitis C virus was associated with a significantly increased risk of RCC (hazard ratio 1.77), after adjusting for age, gender, ethnicity, and the presence of chronic kidney disease.
Analgesics
Phenacetin-containing analgesics have been implicated chiefly in the etiology of renal pelvic cancer, but their role in RCC risk is less clear. Several studies have found a moderately elevated RCC risk with regular or long-term use of phenacetin. More recent studies had limited power to evaluate phenacetin because the drug has been unavailable for many years. Among other analgesics, a few studies have found a positive association between acetaminophen, a metabolite of phenacetin, and RCC risk. A meta-analysis of 5 case-control studies and 3 cohort studies found some suggestion of positive association between use of aspirin and RCC risk. More recently, prospective data from more than 140,000 individuals found that the risk for RCC was increased among subjects who used nonaspirin, nonsteroidal anti-inflammatory drugs. Aspirin use was not associated with RCC risk.
Reproductive Factors and Hormones
The reason for the consistent gender difference in RCC incidence is unknown, but hormone-related factors may play a role. Several studies found no associations with use of oral contraceptives or hormone replacement therapy, but in some studies risk of RCC was significantly reduced following oral contraceptive use among nonsmokers. Hysterectomy has been associated with increased risk of RCC in case-control studies and one recent cohort study, but not in all. At least 8 studies have consistently found a positive association with number of births. The possible role of reproductive factors in RCC etiology remains poorly understood, but there is some evidence that certain hormone-related factors are associated with the risk, although these associations seem unlikely to explain the lower incidence among women than in men.
Occupation
In contrast to bladder cancer, RCC is generally not considered an occupation-related cancer, although associations have been reported with asbestos, gasoline and other petroleum products, hydrocarbons, lead, cadmium, and trichloroethylene (TCE). The IARC has considered TCE, used mainly in metal degreasing and dry cleaning, as carcinogenic in animals and probably also in humans. A possible association between TCE and RCC has been reported in numerous studies but is not yet proven as causal. It is interesting that RCC patients with high exposure of TCE have been shown to have more frequent somatic von Hippel-Lindau (VHL) mutations.
Risk factors
Tobacco Use
Cigarette smoke, containing a wide range of carcinogenic compounds including polycyclic aromatic hydrocarbons, aromatic amines, heterocyclic amines, and N -nitrosamines, can both initiate and promote tumor development in animals. Cigarette smoking is also one of the well-established risk factors for RCC. According to The International Agency for Research on Cancer (IARC) there is sufficient evidence to define tobacco smoking as a cause of RCC. A meta-analysis of 24 (19 case-control and 5 cohort) studies reported a relative risk of 1.38 (95% confidence interval 1.27–1.50) for ever-smokers compared with lifetime never-smokers. Men had a 54% and women had a 22% increased risk for RCC. There was also a dose-dependent increase in risk related to the number of cigarettes smoked per day. Smoking cessation for more than 10 years may reduce the elevated risk attributable to smoking.
Anthropometric Measures
Overweight, especially obesity, is another well-established risk factor for RCC in both women and men. According to a meta-analysis of 17 epidemiologic studies, a 5-unit increase in body mass index increases risk for RCC by 24% in men and 34% in women. Later studies also supported the positive association in both genders. Most studies found a dose-response relationship with increasing body mass index. Waist circumference and waist-hip ratio provide an estimate of abdominal or central obesity, a powerful contributor to metabolic abnormalities such as insulin resistance and hyperinsulinemia. In a few studies, waist circumference or waist-hip ratio was positively associated with RCC risk, as was weight gain or loss. The proportion of all cases of RCC attributable to overweight and obesity has been estimated to be about 40% in the United States and up to about 30% in European countries. There is still an unexplained stronger association in women than in men.
The mechanisms by which obesity influences renal carcinogenesis are not clear, but several plausible although speculative explanations exist. For example, sex steroid hormones may affect renal cell proliferation and growth by direct endocrine receptor-mediated effects, by regulation of receptor concentrations, or through paracrine growth factors such as epidermal growth factor. Further, obesity is related to several endocrine disorders such as decreased levels of sex hormone-binding globulin and progesterone, anovulation, insulin resistance, and increased levels of growth factors such as insulin-like growth factor 1 and high circulating levels of leptin. Lower adiponectin levels have also been observed among RCC patients than in healthy controls. There is also some evidence that link obesity, inflammation, and development of insulin resistance.
Adult height is a complex variable because of its multiple determinants, including genetic, nutritional, and health-related factors. Most, but not all studies have found a positive association between height and risk of RCC.
Physical Activity
Because energy expenditure is an important determinant of adult weight and obesity, a role of physical activity in renal carcinogenesis is plausible. The impact of occupational and/or recreational physical activity on the risk of RCC has been reported in several case-control and cohort studies. Some of the studies found that either occupational or recreational physical activity was associated with reduced risk of RCC. It remains unclear whether the association is independent of obesity.
Foods
Meat intake has been hypothesized to elevate risk for RCC, presumably because of its fat and protein content. Besides these nutrients, products in cooked meat such as heterocyclic amines, polycyclic aromatic hydrocarbons, and in cured meat nitrites and nitrates may mediate the renal carcinogenic process. Studies suggest an association between fried, processed, or barbecued meat and RCC risk. A meta-analysis of 13 case-control studies found a positive association between consumption of poultry, processed meat, red meat, and all meat and RCC risk, with 20% to 30% elevated risk among those in the highest compared with the lowest intake category for each of the meat groups. Later case-control studies also supported the positive association between red meat intake and RCC risk. By contrast, a recent pooled analysis of 13 prospective studies from North America and Europe found no association between intakes of red meat, processed meat, poultry, or seafood and RCC risk, nor did a large prospective European study.
Fruits and vegetables contain antioxidant nutrients and other dietary factors that may reduce RCC risk. Several case-control studies found a protective effect of vegetables and/or fruits, often strong for vegetables, especially the dark green and cruciferous varieties. A pooled analysis of 13 prospective studies also found an inverse association between fruit and vegetable consumption and RCC risk. However, in the large prospective European study, no associations between consumption of fruits and vegetables, except root vegetables, and RCC risk were observed.
Neither coffee nor tea drinking has been conclusively associated with RCC risk, although a pooled analysis of 13 prospective studies found an inverse association with both coffee and tea.
Two studies have examined dietary pattern and RCC; one study found an inverse association with “drinker pattern” (wine, hard liquor, beer, and snacks) and the other found a positive association with high-fat and high-protein diets.
Nutrients
Fat and protein intake and RCC risk has been examined in several case-control studies, some of which found a positive association. However, a recent pooled analysis of 13 prospective studies from North America and Europe found no association between intakes of fat and protein or their subtypes and RCC risk. On the other hand, antioxidant nutrients including carotenoids, vitamin C, and vitamin E have been associated with reduced risk of RCC. A pooled analysis of 13 prospective studies found an inverse association between β-carotene intake and RCC risk.
Alcohol
Although alcohol intake is related to elevated risk of several cancer sites such as oral cavity, esophagus, and breast, several case-control studies, a pooled analysis of 13 prospective studies, and a large European study consistently found an inverse association between alcohol consumption and RCC risk. Overall, evidence is convincing that alcohol intake does not increase but most likely reduces risk of RCC, perhaps through enhancement of insulin sensitivity and risk of diabetes.
Hypertension and Antihypertensive Medications
History of hypertension has been consistently associated with an elevated risk of RCC. There is indeed sufficient evidence that hypertension is an independent risk factor for RCC. Use of antihypertensive medications including diuretics and nondiuretic antihypertensive medications has also been associated with elevated risk of RCC. However, these data likely reflect confounding by indication rather than a causal association. As suspected, some studies reported that the association with hypertensive medications disappeared once hypertension was accounted for and high blood pressure was associated with an increased risk also among men and women who never took antihypertensive medications. The association between risk of RCC and hypertension has also been shown to be independent of obesity. The biological mechanism for the association between risk for RCC and hypertension is not known.
Other Medical Conditions
End-stage renal disease
The incidence of RCC in patients with end-stage renal disease developing acquired cystic kidney disease has been reported to be elevated compared with the general population. An increased risk has also been seen in native kidneys after renal transplantation. While proliferation of proximal tubular epithelial cells has been identified as the major pathogenic mechanism of cyst formation, hormones (eg, estrogens), growth factors, and their receptors may stimulate cell proliferation and promote carcinogenesis. This mechanism may also explain, in part, the onset of multiple renal adenomas and bilateral carcinomas that develop in patients with acquired cystic kidney disease.
Diabetes mellitus
Most case-control studies found either no increased risk with diabetes or an excess risk confined to women. Few cohort studies exist, but some reported a significantly increased incidence of RCC among diabetic patients. However, diabetes may not be an independent risk factor because of its strong relation to obesity and hypertension. Elevated levels of growth factors and growth factor receptors may mediate the possible relationship between diabetes and RCC.
Chronic hepatitis C infection
One recent prospective study found that chronic infection with hepatitis C virus was associated with a significantly increased risk of RCC (hazard ratio 1.77), after adjusting for age, gender, ethnicity, and the presence of chronic kidney disease.
Analgesics
Phenacetin-containing analgesics have been implicated chiefly in the etiology of renal pelvic cancer, but their role in RCC risk is less clear. Several studies have found a moderately elevated RCC risk with regular or long-term use of phenacetin. More recent studies had limited power to evaluate phenacetin because the drug has been unavailable for many years. Among other analgesics, a few studies have found a positive association between acetaminophen, a metabolite of phenacetin, and RCC risk. A meta-analysis of 5 case-control studies and 3 cohort studies found some suggestion of positive association between use of aspirin and RCC risk. More recently, prospective data from more than 140,000 individuals found that the risk for RCC was increased among subjects who used nonaspirin, nonsteroidal anti-inflammatory drugs. Aspirin use was not associated with RCC risk.
Reproductive Factors and Hormones
The reason for the consistent gender difference in RCC incidence is unknown, but hormone-related factors may play a role. Several studies found no associations with use of oral contraceptives or hormone replacement therapy, but in some studies risk of RCC was significantly reduced following oral contraceptive use among nonsmokers. Hysterectomy has been associated with increased risk of RCC in case-control studies and one recent cohort study, but not in all. At least 8 studies have consistently found a positive association with number of births. The possible role of reproductive factors in RCC etiology remains poorly understood, but there is some evidence that certain hormone-related factors are associated with the risk, although these associations seem unlikely to explain the lower incidence among women than in men.
Occupation
In contrast to bladder cancer, RCC is generally not considered an occupation-related cancer, although associations have been reported with asbestos, gasoline and other petroleum products, hydrocarbons, lead, cadmium, and trichloroethylene (TCE). The IARC has considered TCE, used mainly in metal degreasing and dry cleaning, as carcinogenic in animals and probably also in humans. A possible association between TCE and RCC has been reported in numerous studies but is not yet proven as causal. It is interesting that RCC patients with high exposure of TCE have been shown to have more frequent somatic von Hippel-Lindau (VHL) mutations.
Related posts:
 Renal Cell Carcinoma
Renal Cell Carcinoma
 Systemic Therapy for Metastatic Non–Clear-Cell Renal Cell Carcinoma: Recent Progress and Future Directions
Systemic Therapy for Metastatic Non–Clear-Cell Renal Cell Carcinoma: Recent Progress and Future Directions
 Management of Treatment-Related Toxicity with Targeted Therapies for Renal Cell Carcinoma: Evidence-Based Practice and Best Pr actices
Management of Treatment-Related Toxicity with Targeted Therapies for Renal Cell Carcinoma: Evidence-Based Practice and Best Pr actices
 Clinical and Molecular Prognostic Factors in Renal Cell Carcinoma: What We Know So Far
The Role of Surgery in the Management of Early-Stage Renal Cancer
mTOR Inhibitors in Advanced Renal Cell Carcinoma
Clinical and Molecular Prognostic Factors in Renal Cell Carcinoma: What We Know So Far
The Role of Surgery in the Management of Early-Stage Renal Cancer
mTOR Inhibitors in Advanced Renal Cell Carcinoma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


