Anal cancer is a rare malignancy, although its incidence has been increasingly in recent decades. This article discusses risk factors for anal cancer and how these risk factors affect the changing demographics of this disease.
Key points
- •
Anal canal cancer is a rare malignancy.
- •
The incidence of anal canal cancer is increasing, particularly among young men.
- •
Risk factors for anal cancer include human papilloma virus (HPV) infection, human immunodeficiency virus (HIV) infection, more than 10 sexual partners, and anoreceptive intercourse.
- •
Anal cancer risk increases with the duration of HIV infection.
- •
The increased incidence in anal cancer is caused by increased prevalence of HPV and longer survival of individuals infected with HIV.
Introduction
Anal cancer is an uncommon malignancy, but the incidence of this disease has been increasing over the past 30 years. This article focuses on anal canal squamous cell cancers (SCCAs), which comprise most anal canal cancers. Risk factors for anal canal cancer are well established, including human papillomavirus (HPV) infection and human immunodeficiency virus (HIV) infection, both of which correlate with increased number of sexual partners and anoreceptive intercourse. The increase in anal cancer is attributed to multiple factors, including increased prevalence of HPV and longer survival of individuals infected with HIV.
Introduction
Anal cancer is an uncommon malignancy, but the incidence of this disease has been increasing over the past 30 years. This article focuses on anal canal squamous cell cancers (SCCAs), which comprise most anal canal cancers. Risk factors for anal canal cancer are well established, including human papillomavirus (HPV) infection and human immunodeficiency virus (HIV) infection, both of which correlate with increased number of sexual partners and anoreceptive intercourse. The increase in anal cancer is attributed to multiple factors, including increased prevalence of HPV and longer survival of individuals infected with HIV.
Overview
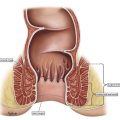
Anal canal cancer refers to malignancy of the mucosa-lined anal canal arising from 1 to 2 cm proximal to the dentate line to the intersphincteric groove separating the anal margin from the anal canal. Roughly 85% of anal canal cancers are of squamous cell origin. Of the remaining cases, roughly 10% are adenocarcinoma and 5% are rare tumor types such as melanoma, small cell carcinoma, and tumors metastatic from other sites.
The American Cancer Society estimates there will be 8080 new cases of anal (anus, anal canal, and anorectum) cancer in 2016, roughly 60% of which will be in women. It is estimated that 1080 individuals will die from their disease. Although generally considered a rare cancer, representing 2.7% of all digestive malignancies and less than 0.5% of all diagnosed malignancies, the incidence of SCCA has been increasing over the last few decades.
Risk factors
Sexual Activity
Risk factors for anal cancer were initially determined by case-control studies comparing men and women with anal cancer with normal control subjects and patients with adenocarcinoma of the colon or rectum. For example, Frisch and colleagues compared 417 patients with anal cancer with 534 patients with adenocarcinoma of the rectum and 554 normal control subjects. The relative risk of anal cancer was highest in people with 10 or more sexual partners or history of sexually transmitted diseases (STDs) such as HIV, herpes, gonorrhea, syphilis, and chlamydia ( Box 1 ).
HPV infection
HIV infection
More than 10 lifetime sexual partners
Anoreceptive intercourse
Chronic immunosuppression
Cigarette smoking
History of gynecologic or hematologic malignancy
Human Papilloma Virus
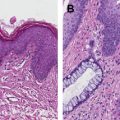
As noted earlier, sexual activity was found to be a risk factor for anal cancer. In addition, an increased risk of anal cancer was noted in individuals with cervical cancer. As the link between cervical cancer and HPV became established, investigators speculated that HPV might also be causative in anal cancer. The well-established progression from HPV infection to cervical intraepithelial neoplasia to cervical malignancy led to exploration of anal epithelial neoplasia as a precursor lesion to SCCA.
Increasing evidence indicates that the oncogenic strains of HPV, specifically subtypes 16 and 18, cause SCCA in the anal canal as they are known to do in the cervix and head and neck. Early evidence, including a study by Frisch and colleagues, that found HPV DNA in 88% of patients with anal cancer but in none of the patients with rectal cancer in the series. HPV subtype 16 was involved in 73% of the anal cancer cases.
HPV risk factors include increased number of sexual partners, anoreceptive intercourse, and other STDs, particularly underlying HIV infection. Thus many of the early identified sexual risk factors are simply risks for acquisition of oncogenic HPV strains. Not surprisingly, personal history of one HPV-associated malignancy is a risk factor to acquire a second HPV-associated malignancy.
The prevalence of HPV in the United States is variable, ranging from 10% in low-risk groups to nearly 90% in individuals infected with HIV. It is thought that HPV is associated with 65% to 89% of all SCCA of the anal canal, making this the leading risk factor for this malignancy. A recent series of 72 metastatic anal cancer cases at MD Anderson revealed that 94% had detectable HPV. Note that, unlike in head and neck cancer, in which HPV-positive disease portends improved prognosis, the prognostic value of HPV in anal cancer is unknown.
Human Immunodeficiency Virus
HIV infection is a well-established risk factor for anal canal cancer. However, the risk of SCCA is not reduced by the use of highly active antiretroviral therapy (HAART). Some degree of the increased incidence of anal cancer in general is likely caused by improvements in HIV patient survival because the risk for SCCA increases with the duration of HIV infection; there is a 12-fold greater risk of anal cancer for persons who have been infected with HIV for 15 years or longer compared with those who have been infected with HIV for 5 years or less. The increased incidence in anal canal cancer from 19.0 per 100,000 person-years from 1992 to 1995 to 78.2 per 100,000 person-years from 2000 to 2003 correlates with the natural history of HIV and HPV coinfections starting during the HIV epidemic in the 1980s. Specifically, the expected progression from viral infection to HPV-associated anal epithelial changes to development of SCCA would be expected to take 1 to 2 decades.
Chronic Immunosuppression
It is well established that anal cancer occurs at increased rates in patients with chronic immunosuppression either because of inherited or acquired immunodeficiency. For example, there is a 10-fold to 100-fold increased relative risk for SCCA in renal transplant patients. Some of this risk is mediated by HPV infections because the infection rate in new renal transplant patients is 23% but increases to 47% in established renal transplant patients. Similarly there is a 4-fold increased relative risk for SCCA in cardiac transplant patients.
Other types of immunosuppression, such as chronic steroid use or immunomodulators used for treatment of autoimmune diseases, are not as clearly linked to SCCA, although there is an increased likelihood of persistent HPV infection.
There is some evidence of increased risk of HPV-driven cervical cancer in patients with inflammatory bowel disease, but no definitively increased risk has been shown for anal cancer in these patients.
Tobacco Use
Case-control studies indicate that cigarette smoking significantly increases the risk of contracting anal cancer. There seems to be a direct correlation between number of cigarettes smoked and increased relative risk. Specifically, Holly and colleagues found a relative risk of 1.9 for persons with a 20-pack-year smoking history and a relative risk of 5.2 for persons with a 50-pack-year history. Current smoking is the highest risk, with a relative risk of 7.7 in women and 9.4 in men.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


