Table 4.1 Male Age-Adjusted Incidence by Cancer Site, 1973-2009 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
and for heavy drinkers, these odds are 9.60 to 11.37 higher.6 There is some heterogeneity in the effect of cigarette smoking by OCPC subsite as tobacco exposure is found to be more strongly associated with cancers of the soft palate than other sites.11 Additionally, the use of black versus blond tobacco may have an even greater risk of oral cavity and pharyngeal cancer.12 Among former smokers, the risk of cancer of the oral cavity is less than that of smokers, and one study reported that after 10 years of quitting, former smokers had the same risk of OCPC as never smokers.9,13
Table 4.2 Female Age-Adjusted Incidence by Cancer Site, 1973-2009 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
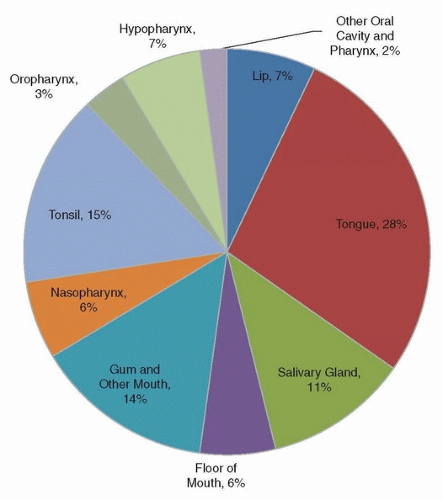 Figure 4.1. Distribution of cancer of the oral cavity and pharynx by subsite in SEER 18 2000-2009. (Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2011 Sub (1973-2010) <Katrina/Rita Population Adjustment>— Linked To County Attributes—Total U.S., 1969-2010 Counties. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission. http://www.seer.cancer.gov) |
drinkers, respectively.23 Some studies have suggested variations in the effect of alcohol by subsite; however, the pattern is inconsistent across studies.10,12,24
decreasing as depicted in Figure 4.4.47,48,49 Between 1988 and 2004, HPV-related OPSCC increased 225% whereas HPV-unrelated OPSCC declined 50% during the same time period.49 Starting in 2004, the incidence of HPV-related OPSCC and OCSCC approached non-HPV-related OPSCC and OCSCC.47 Declines in HPV-unrelated OPSCC are attributed to the reduced prevalence of cigarette smoking in the United States as well as decreases in per capita use of hard alcohol.47 Smoking prevalence for adults in the United States has decreased from 42.4% in 1965 to 18.9% in 2011.44 HPV-related OPSCC and OCSCC have increased across all age groups; however, there are particularly marked increases in more recent birth cohorts, suggesting differences in sexual practices over time. Though data on HPV prevalence in cancers of the oral cavity over time are limited, a study in Colorado reported that the prevalence of HPV in cancer of the oropharynx rose from 33% in the 1980s to 82% in the mid-2000s.50
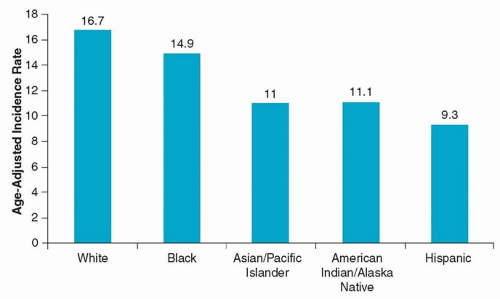 Figure 4.2. Age-adjusted incidence of cancer of the oral cavity and pharynx by race/ethnicity among males, SEER 18 2006-2010. (Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2011 Sub (1973-2010) <Katrina/Rita Population Adjustment>— Linked To County Attributes—Total U.S., 1969-2010 Counties. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission. http://www.seer.cancer.gov) |
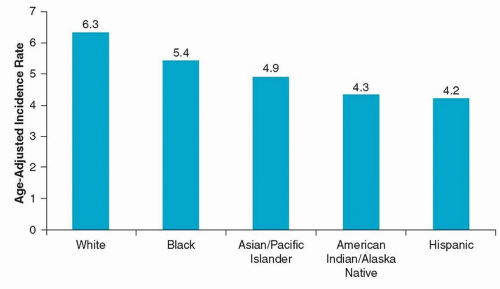 Figure 4.3. Age-adjusted incidence of cancer of the oral cavity and pharynx by race/ethnicity among females, SEER 18 2006-2010. (Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2011 Sub (1973-2010) <Katrina/Rita Population Adjustment>—Linked To County Attributes—Total U.S., 1969-2010 Counties. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission. http://www.seer.cancer.gov) |
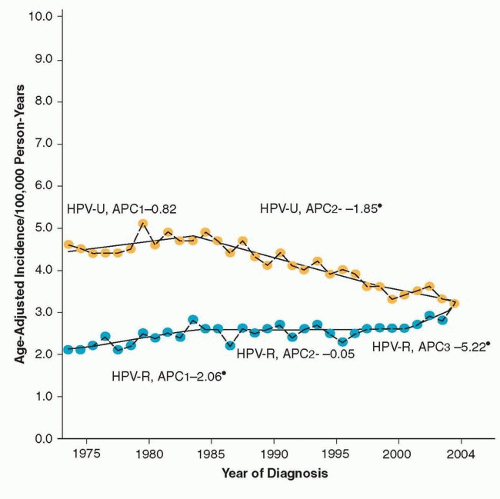 Figure 4.4. Incidence of HPV-related and HPVunrelated squamous cell carcinomas of the oral cavity, 1975-2004. (Chaturvedi AK, Engels EA, Anderson WF, et al. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol. 2008;26:612-619.) |
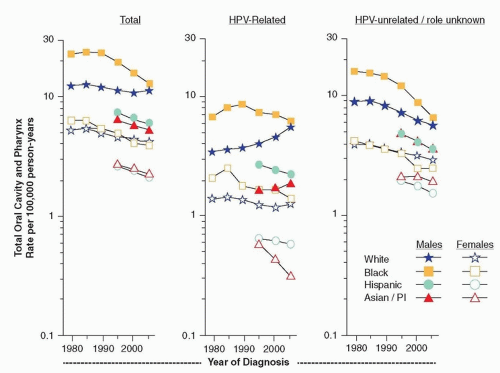 Figure 4.5. Age-adjusted HPVrelated and HPV-unrelated squamous cell carcinoma of the oral cavity by diagnosis year, race, and gender, 1977-2007. (Brown LM, Check DP, Devesa SS. Oropharyngeal cancer incidence trends: diminishing racial disparities. Cancer Causes Control. 2011;22:753-763.) |
blacks have poorer survival even among those with localized cancer, indicating that other factors, including lower socioeconomic status (SES) and suboptimal treatment, also contribute to poorer survival among blacks than whites.53 Black patients with cancer of the oral cavity and pharynx were less likely to receive cancer-directed surgery and more likely to receive radiation without chemotherapy.56 Even after adjusting for treatment, insurance, and other sociodemographic factors, blacks had a 45% increased risk of all-cause death in a recent study of over 20,000 cases of cancer of the oropharynx.57 Some of the increased hazard of death among blacks could be due to other competing causes of death as this study examined overall survival; however, after adjusting for comorbidity, blacks still had a higher hazard of death in this study.
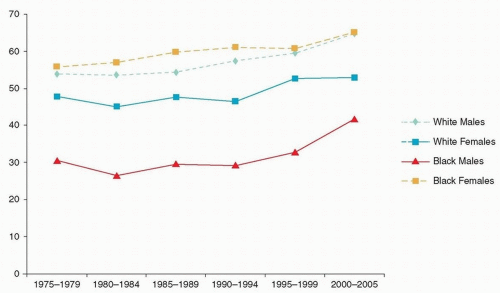 Figure 4.6. A 5-year relative survival for cancers of the oral cavity and pharynx by race and gender, SEER 18 1975-2005. (Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2011 Sub (1973-2010) <Katrina/Rita Population Adjustment>—Linked To County Attributes—Total U.S., 1969-2010 Counties. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission. http://www.seer.cancer.gov) |
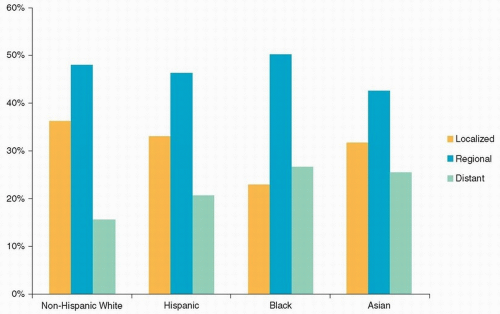 Figure 4.7. Stage distribution among cancers of the oral cavity and pharynx by race/ethnicity, SEER 18 2000-2010. (Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2011 Sub (1973-2010) <Katrina/Rita Population Adjustment>—Linked To County Attributes—Total U.S., 1969-2010 Counties. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission. http://www.seer.cancer.gov) |
Table 4.3 Five-Year Relative Survival for Pharynx Cancers of the Oral Cavity by Race/Ethnicity, Stage, and Gender, SEER 18 2003-2009 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
studies have reported a positive association among males,63 whereas another reports a significant association for females only64 and another study reported null findings for both males and females.65 Studies have more consistently reported an association between radiation exposure and cancer of the major salivary glands.63,64,66 Some studies have reported an association between occupational exposures and cancer of the major salivary glands,63,66 whereas others have not.65
Table 4.4 Age-Adjusted Incidence of Cancer of the Major Salivary Glands by Sex, Site and Race/Ethnicity, and Age per 100,000 Person-Years, SEER 18 1990-2009 | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


