Epidemiological Research on SARS in People’s Republic of China
1. Introduction
Severe Acute Respiratory Syndrome (SARS), also called infectious atypical pneumonia by the Law for Prevention and Control of Infectious Diseases of China, is an acute infectious disease that is caused by SARS-Coronavirus and it principally manifests respiratory symptoms. General population are susceptible to this disease. SARS is characterized by high contagiousness, fast deterioration, poor prognosis, and severe lung damage. Clinically, this kind of pneumonia is different from typical pneumonia (lobar pneumonia caused by pneumococcus), from pneumonia caused by mycoplasma pneumoniae, chlamydia pneumoniae, pneumonia chlamydiapsitatci, legionellapneumophila or Coxiella burnetii. SARS was reported for the first time on 2 Jan. 2003 by Guangdong province of China and a review later found that the earliest case occurred on 16 Nov. 2002 in Foshan city of Guangdong. On 12 and 27 March 2003, WHO delivered its warnings on SARS to the world twice. On 16 March, WHO couched this atypical pneumonia taking place in China as SARS. Based on research on viral morphology, molecular biology, serology and animal experiments conducted by experts from 13 networked laboratories in nine countries, WHO declared on 16 April that it was a new coronavirus that caused SARS, named it SARS-Coronavirus and confirmed all gene sequences for the virus.
SARS once became rampant in China after it made its debut because it is highly contagious and the medical community was unable to confirm its pathogen at that time, the public health system, particularly that in China, was relatively weak in monitoring and giving immediate response to it. Prevention and control measures were in serious shortage, and the public lacked basic knowledge about it. As of 31 July 2003, there had been accumulatively 8,098 SARS cases on the globe, claiming 774 lives. China mainland witnessed the first case of SARS and is the most hit area, with 5,327 SARS cases and a death toll of 349, accounting for 66% of total cases in the world. During the virus’ debut time because of unknown nature of the virus and the disease, China lacked lab diagnostic methods for SARS, and Chinese health professionals did not know the transmission route of the disease and did not have an effective preventive measures such as SARS-specific vaccine, it was extremely difficult for SARS prevention, early detection, and effective treatment. However, the Chinese government, along with its health professionals ultimately contained spread of the disease by using classic prevention measures including isolating the infection source, quarantine, tracing people that have contacted SARS patients, and implementing personal protective measures. WHO stated that China played a vital role in containing spread of SARS in the world.
In late 2003, SARS cases occurred in
Taiwan of China and Singapore due to occupational exposure in laboratories, and some four sporadic SARS cases took place in Guangzhou in early 2004 and April of that year. Nine SARS cases (one died) due to occupational exposure in labs also occurred in Anhui and Beijing.
Taiwan of China and Singapore due to occupational exposure in laboratories, and some four sporadic SARS cases took place in Guangzhou in early 2004 and April of that year. Nine SARS cases (one died) due to occupational exposure in labs also occurred in Anhui and Beijing.
2. Prevalence of SARS
2.1 Prevalence of SARS in China
In China, the first SARS case took place in Foshan of Guangdong province on 16 Nov. 2002. As of 24 June 2003, 24 provinces, autonomous regions and municipalities of China reported 5,327 SARS cases, and with 349 death cases, the mortality rate was 6.55%. Guangdong province reported 1,512 cases (58 died) with a mortality rate of 3.84%. On 1 March 2003, Beijing witnessed its first SARS case coming from another region and from then on reported 2,521 cases (193 died), with a mortality rate of 7.66%. Other severely hit areas include Tianjin, Hebei, Shanxi, and Inner Mongolia. After reviewing the earlier cases, it is considered that Guangdong and Guangxi may be the origin of SARS, and ealrier cases in other 22 provinces, autonomous regions and municipalities of China are imported from other regions (see Table 9.1 ).
Table 9.1 Prevalence of SARS in China (November 16, 2002-June 24, 2003) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
On 15 Feb. 2003, Hong Kong witnessed its first SARS case. Since then it has
reported 1,755 SARS cases, falling into the group of Prince of Wales Hospital and of Amoy Garden, with 299 dead and a mortality rate of 17.1%. There are 346 SARS cases reported in Taiwan with 37 dead, and a mortality rate of 11%. The first SARS case in Taiwan took place on 25 Feb. 2003.
reported 1,755 SARS cases, falling into the group of Prince of Wales Hospital and of Amoy Garden, with 299 dead and a mortality rate of 17.1%. There are 346 SARS cases reported in Taiwan with 37 dead, and a mortality rate of 11%. The first SARS case in Taiwan took place on 25 Feb. 2003.
From Nov. 2002-June 2003, SARS became an epidemic. SARS cases reported by China mainland, Hong Kong, Macau and Taiwan accounted for 91.7 % of all SARS cases in the world.
In Dec. 2003, four new SARS cases occurred in Guangdong and were confirmed as sporadic, not endemic.
In April 2004, nine SARS cases due to occupational exposure in labs were reported in Anhui and Beijing.
2.2 Prevalence of SARS in the World
As of 31 July 2003, SARS cases had been seen in 20 nations and districts in Asia, America, and Europe. Six nations and districts had SARS cases over 60 including China, Hong Kong, Taiwan, Canada, Singapore, and Vietnam. SARS cases in the USA and Philippines were between 10-50, and other nations had cases less than 10. Most SARS cases occurred during the period of Feb to April in 2003.
SARS-infected individuals once accommodated in a hotel in Hong Kong spread SARS to medical professionals of Vietnam, Singapore and Canada, along aviation routes to the world. Singapore had 238 SARS cases accumulatively, 33 deaths with a mortality rate of 14%, since 25 Feb. 2003. Vietnam had 63 cases and 5 deaths with a mortality rate of 8% since 23 Feb. 2003. The mortality rate in Vietnam was lower than the average of the world. On April 28, 2003, WHO removed Vietnam from SARS epidemic areas, leaving Vietnam the first nation that successfully controlled SARS outbreak and contained spread to other areas. SARS cases in Canada were stemmed from two spread chains that originated from two hospitals, with a total of 251 cases, 41 death cases and a mortality rate of 17%. Canada’s first case occurred on 23 Feb. 2003 who was a traveler to Hong Kong and was associated with the outbreak of SARS in Hong Kong. The last case in Canada was diagnosed on June 8. In the U.S.A., after corrections and retest, the ultimate reported SARS cases were confirmed as 29, and no death toll.
3. Epidemiological Features of SARS
3.1 Distribution of SARS in terms of Region, Time and Population
3.1.1 Regional distribution
In 2003, 24 provinces, autonomous regions and municipalities in China mainland reported SARS cases and seven provinces and autonomous regions reported no case including Hainan, Guizhou, Yunnan, Heilongjiang, Tibet, Qinghai and Xinjiang. The majority of cases clustered in six areas including Beijing (2,521 cases), Guangdong (1,512), Shanxi (448), Inner Mongolia (282), Tianjin (175) and Hebei (215) (Figure 9.1), accounting for 96.7% of total cases in China. Three hundred twenty-nine died (accounting for 94.3%) in those six areas. Other provinces had rare cases, with six provinces with between 10-35 cases, and 12 provinces with less than 10 cases.
Surveys indicate that SARS cases taking place in 24 provinces of China mainland are apparently associated in epidemiological features (Figure 9.2). Both Guangdong and Beijing were considered
two major originated and spread sou rces in China. Guangdong was associated with the SARS outbreaks in Sichuan, Hunan, Inner Mongolia, Shanxi, Beijing, Anhui, Shanghai and Fujian, and Beijing is related to the outbreaks in Gansu, Jilin, Liaoning, Shaanxi, Chongqing, Hubei, Zhejiang, Tianjin and Hebei.
two major originated and spread sou rces in China. Guangdong was associated with the SARS outbreaks in Sichuan, Hunan, Inner Mongolia, Shanxi, Beijing, Anhui, Shanghai and Fujian, and Beijing is related to the outbreaks in Gansu, Jilin, Liaoning, Shaanxi, Chongqing, Hubei, Zhejiang, Tianjin and Hebei.
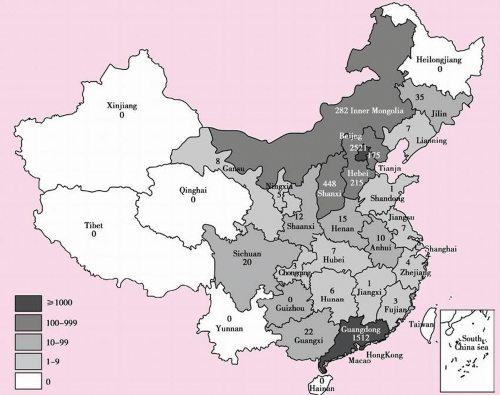 Figure 9.1 2003’s Distribution of SARS in 24 Provinces, Autonomous Regions, and Municipalities in China Mainland |
SARS outbreaks usually occurs in traffic hubs or densely populated areas, spreading via traffic vehicles from source areas across provinces, nations and continents. Surveys conducted in Beijing showed that the less densely populated areas, the lower the prevalence rate. In Shanxi province SARS clustered in urban areas, accounting for 83.82%, and in rural areas it was sporadic. Guangdong and Beijing are key areas for SARS in China, accounting for 75.71% of total SARS cases. Convenient traffic and frequent migration enhanced SARS spread from Guangdong, Beijing and Hong Kong to other areas. All traceable infection sources in Guangdong province were distributed in the Pearl River delta and Hong Kong.
In 2003, Guangdong was considered a major epidemic source. It is associated directly or indirectly with most SARS cases in the world. The cases in that year principally clustered in China and southeast Asia nations spreading to North America and Europe via aviation. Ninety-seven percent of SARS cases in the USA were imported, and all cases in Australia, France, Germany, Italy, Switzerland, Korea
and Thailand were imported [2].
and Thailand were imported [2].
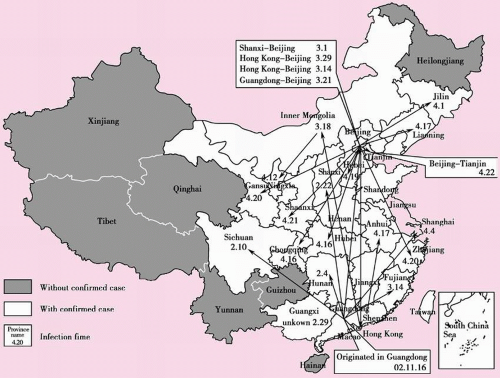 Figure 9.2 Spread of SARS in Chinese Mainland |
3.1.2 Time distribution
a) Scenario of SARS epidemic in China in 2003
SARS epidemic in China in 2003 fell into four stages:
Stage 1: Before late Feb. 2003 The epidemic was contained within Guangdong, few provinces saw imported cases, and the debut cases did not cause endemic.
Stage 2: Early March 2003-mid April 2003 The epidemic was still contained within Guangdong but incidence lowered, local transmission in Shanxi, Beijing and Inner Mongolia occurred.
Stage 3: Late April 2004-mid May 2004 The epidemic principally occurred in Beijing and its outskirt areas, beginning to spread to other provinces. The outbreak in Beijing spread to four provinces in northern China.
Stage 4: In late May in 2004 The epidemic in China was gradually contained. On June 24, WHO declared to lift quarantine and isolation in Beijing, indicating SARS was fully contained. Later, there was no SARS case report.
b) Time distribution
China is the first area that reported SARS in the world, stating occurrence of SARS in its Guangdong province on 16 Nov. 2002. Peak of SARS epidemic in China occurred during March 21 – May 19 in 2003, with an average daily incidence of 30 cases. The highest daily incidence was on April 23; from then on the incidence began to sag, entering a platform stage with 15 cases each day. Since May 19 the incidence began to be one digit and since May 29 no
cases were available. As of Aug. 16 China mainland had no clinically diagnosed SARS case. Incidence in Guangdong and Beijing made up two peaks for China SARS outbreak (Figure 9.3). Guangdong peaked its incidence during Jan. 28-Feb. 26, 2003, and Beijing peaked its incidence on April 25, with its first case on March 8, 2003 and the last case on May 28.
cases were available. As of Aug. 16 China mainland had no clinically diagnosed SARS case. Incidence in Guangdong and Beijing made up two peaks for China SARS outbreak (Figure 9.3). Guangdong peaked its incidence during Jan. 28-Feb. 26, 2003, and Beijing peaked its incidence on April 25, with its first case on March 8, 2003 and the last case on May 28.
Guangdong began to see SARS cases as early as in Nov. 2002, Guangxi in Dec., Sichuan, Hunan, and Shanxi in Feb., and Beijing, Inner Mongolia, Hubei, Shanghai, Ningxia and Shandong in March (6 provinces), Henan, Jiangxi, Jiangsu, Hubei, Liaoning, Jilin, Shaanxi, Gansu, Chongqing, Tianjin, Hebei, Zhejiang and Anhui in April (13 provinces).
2002-2003′ SARS epidemic showed that, similar to other respiratory infectious disease, SARS is also prone to break out in winter and spring, and biological features of SARS virus and outbreak peaks in northern and southern China also suggest that measures to prevent and control SARS should be ready before winter and spring set in.
In winter of 2003, there were four new sporadic SARS cases in Guangdong, indicating that the outbreak peak of SARS is in winter and spring.
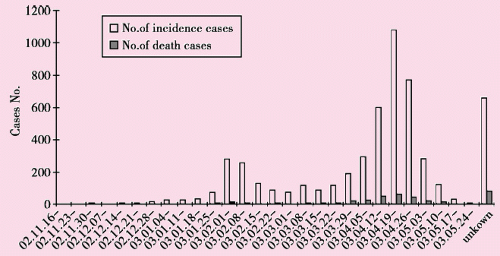 Figure 9.3 Time Distribution of SARS in terms of Incidence and Death |
SARS hit Guangdong and Beijing most. Guangdong’s outbreak peaked during Jan. 28 – Feb. 26, 2003 (accounting for 50.69% of total cases), and sagged later, and maintained a low incidence, the last case took place on June 3, an exotic case. Beijing saw its first SARS case on 8 March 2003 and peaked the outbreak on 25 April; its last case was on 28 May.
3.1.3 Population distribution
a) Gender and age-dependent distribution
The youngest patient in China was one month old and the oldest was 96 years old. SARS cases principally ranged from 20 – 49 years old accounting for 70.23% of all cases. Patients under 20 years old accounted for 8.6%, and older than 50 years accounted for 21.12%. The elderly had a higher mortality rate than the young; the highest mortality rate was seen in people older than 75 years, with a mortality rate of 39.34% (Figure 9.4). Child SARS cases are rare because they have little chance to expose to infection source since the adult in a family will be immediately isolated once he or she presents symptoms. The assumption that SARS-infected adults do not spread the disease needs further research. At present,
there are two case reports stating that adults transmit SARS to children and no report relating spread among children. Ratio of male SARS patients versus female SARS patients is 0.97:1, and among those who died, the ratio is 1.29:1.
there are two case reports stating that adults transmit SARS to children and no report relating spread among children. Ratio of male SARS patients versus female SARS patients is 0.97:1, and among those who died, the ratio is 1.29:1.
Related posts:
 Explore Route of Transmission for Kala-azar
Explore Route of Transmission for Kala-azar
 A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
 Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
 The risk factors and mechanisms of hepatitis B virus intrauterine transmission
Green Tea Drinking and Stomach Cancer in Jiangsu Province, People’s Republic of China Correspondence and Reprint Requests:
The risk factors and mechanisms of hepatitis B virus intrauterine transmission
Green Tea Drinking and Stomach Cancer in Jiangsu Province, People’s Republic of China Correspondence and Reprint Requests:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


