Dyspnea, an unpleasant awareness of breathing, is a very common symptom that is often unrecognized in people with cancer. It is a complex and distressing symptom that can impact people’s daily functioning (1) and result in impaired quality of life (2,3), social isolation (4), and prompt terminal sedation (5). Patients with breathlessness are more likely to visit the emergency department (6) and die in the hospital than at home (7).
Despite the fact that breathlessness is very common in people with cancer (8,9,10,11,12,13), it is often not well controlled. Studies show that unlike pain that is usually improved with current interventions, the intensity of dyspnea is not impacted (14,15). Higginson and McCarthy (14) found that in a group of terminally ill cancer patients cared for at home, pain scores decreased but there was no change in dyspnea scores over time. In a convenience sample of patients admitted to an acute care palliative care unit, Dudgeon et al. (15) also found that for patients who had scores >50 mm on a 100-mm visual analog scale after 7 days of intervention, the median score for breathlessness remained at 50 mm while pain decreased to 30 mm. A recent study found that 27% and 39% of cancer outpatients with moderate to severe pain and dyspnea, respectively, had no evidence of a comprehensive assessment (16).
To optimally manage this distressing symptom, it is necessary to have an understanding of its prevalence and impact; the multidimensional nature of the symptom; the underlying pathophysiology and associated factors; components of a thorough assessment; the clinical syndromes common in cancer patients; and the indications and limitations of current therapeutic approaches.
PREVALENCE
In a large, geographically based cohort with a full scope of cancer diagnoses, over one-half of the patients reported shortness of breath, with half of them having scores on the Edmonton Symptom Assessment System (ESAS) in the moderate to severe range (13). In another study of an outpatient general population, 46% reported breathlessness with only 15% describing the intensity as moderate to severe (8). The differences in intensity may be related to cancer type and/or proximity to death. The first study found that patients with lung cancer had higher intensity scores than other diagnoses and patients with lung cancer composed 19% of the patients as opposed to 4% in the second study. Seow et al. found that patients with lung cancer had 50% greater chance of reporting moderate to severe breathlessness and that the intensity of dyspnea increased over the last 6 months of life (17). Muers and Round found breathlessness to be present at diagnosis in 60% of 298 patients with non-small cell lung cancer and in nearly 90% just prior to death (10). In a radiation oncology community setting, Lutz et al. found that 73% of patients with locally advanced lung cancer presented with breathlessness and the severity was worse in the group that survived <3 months (18). Two studies examined the trajectory of breathlessness in patients with advanced cancer (11,12). In a study of 5,386 cancer patients, Currow et al. showed that the intensity of breathlessness and the prevalence of severe breathlessness increased as death approached, with a significant increase in the rate of change between 3 and 10 days before death (11). Bausewein et al. prospectively followed the intensity of breathlessness in 49 advanced cancer patients and found that breathlessness increased over time and there were 4 different trajectories for individual patients, with fluctuating breathlessness being the most common (12).
IMPACT OF DYSPNEA
Breathlessness is one of the most distressing symptoms for patients (3) and can severely impair their quality of life. In a study of 70 patients with advanced cancer, Reddy et al. identified that patients experienced 2 types of dyspnea: continuous and breakthrough. The majority of patients had breakthrough dyspnea alone (61%), with 39% experiencing constant dyspnea and 20% also having episodes of breakthrough breathlessness (2). Breakthrough dyspnea occurred on an average five to six times a day with a median intensity of 5/10 on ESAS. The median intensity of breathlessness in patients with constant dyspnea was 7/10. Those who experienced continuous dyspnea had a worse quality of life than those with breakthrough dyspnea only, with significant differences in their general activity, mood, walking ability, normal work, and enjoyment of life (2). In a study of late-stage cancer patients, Roberts et al. (1) found that various activities intensified dyspnea for patients: climbing stairs—95.6%, walking slowly—47.8%, getting dressed—52.2%, talking or eating—56.5%, and at rest— 26.1% (1). This study showed that the patients decreased their activity to whatever degree would relieve their breathlessness. Sixty-two percent of the patients with dyspnea had been short of breath for >3 months and most had received no assistance from nurses or physicians, leaving them to cope in isolation. Other studies of patients with lung cancer showed that 97% had decreased their activities, 80% had socially isolated themselves from friends and family (4), 36% were housebound, and 10% largely chair bound because of their breathlessness (19). In a study of terminally ill cancer patients, the willingness to live was directly related to the intensity of breathlessness (20). Uncontrolled dyspnea prompted terminal sedation in 25% to 53% of patients requiring sedation for uncontrolled symptoms (5).
MULTIDIMENSIONAL NATURE OF DYSPNEA
Dyspnea is a complex subjective experience that depends on the integration of respiratory afferent activity, respiratory motor drive, affective state, attention, experience, and learning (21).
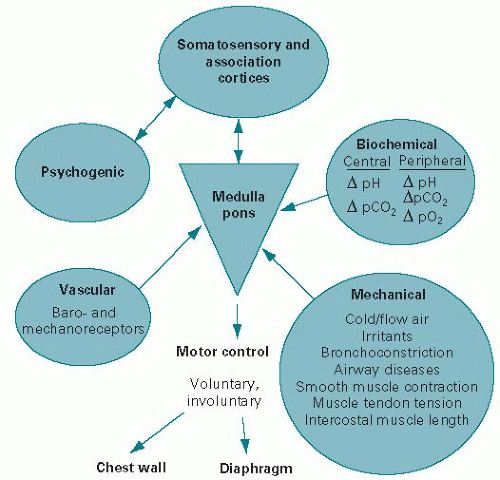
Ventilation results from activation of the respiratory motor drive that is generated in the brainstem respiratory neural network. Receptors in the upper airway, lower airway, lung parenchyma and respiratory muscles, and peripheral and central chemoreceptors provide sensory input to the brainstem respiratory network as well as to higher brain centers (somatosensory and association cortices) (see Fig. 29.1). Normally breathing is not uncomfortable, but if the magnitude of the stimulus from one or more of these sensory afferents is great enough then changes in breathing effort are perceived. Attention, experience/learning, and the person’s affective state further modulate respiratory sensation and perception (21). Recent brain imaging studies suggest that the unpleasantness of dyspnea is processed cortically in the anterior insula and amygdala areas of the brain (22). These neural networks for processing dyspnea are shared with other unpleasant sensations such as pain (23).
Figure 29.1. Brainstem respiratory network.
Abernethy and Wheeler proposed a new conceptual model of breathlessness that they named “Total Dyspnea” (24). This model of Total Dyspnea encompasses four domains: physical, psychological, interpersonal, and existential that contribute to a patient’s distress and suffering. They suggest that “Total Dyspnea” provides a more comprehensive, integrated, conceptual framework to help clinicians understand breathlessness and the suffering of patients and families.
FACTORS ASSOCIATED WITH DYSPNEA IN THE CANCER PATIENT
A number of authors have examined the factors that are associated with dyspnea in patients with cancer (Table 29.1) (2,8,9,25,26,27,28,29,30,31). In two different studies, investigators found that dyspnea in cancer patients had diverse etiologies, commonly with more than one factor contributing to the breathlessness (26,31). In another study, the presence and intensity of dyspnea were strongly related to the number of risk factors a patient had (8). Primary or metastatic involvement of the lung or pleura with cancer was associated with the presence of dyspnea in most studies (2,8,9,25,26,31). In a study of 923 cancer outpatients, Dudgeon et al. found that the risk factors significantly related to the presence of dyspnea were a history of smoking, asthma, or chronic obstructive pulmonary disease (COPD), lung irradiation, or a history of exposure to asbestos, coal dust, cotton dust, or grain dust (8). They also found that the intensity of shortness of breath was significantly associated with the presence of hilar, mediastinal, and rib metastases; and surprisingly, the presence of mediastinal or hilar metastases was associated with a higher intensity of dyspnea than was the presence of lung metastases (8).
The general debility of terminal cancer (9), respiratory muscle weakness (26,27,28), and the presence of the hyperventilation syndrome (25) have been associated with the presence of dyspnea in cancer patients. Interestingly, the presence or severity of dyspnea could not be predicted by the level of oxygen saturation, air flow obstruction, or the type or severity of abnormal spirometry (26,27,28).
The intensity of fatigue, sleep, anxiety, depression, and sense of well-being were significantly associated with ESAS shortness of breath scores in univariate analyses in a prospective observational study of 70 cancer patients with dyspnea (2). In multivariate analyses, ESAS dyspnea was associated with fatigue, forced expiratory volume in 1 minute (FEV1), pain, and depression.
TABLE 29.1 Factors associated with dyspnea in cancer patients
A. Dyspnea Due Directly to Cancer
Lung involvement (primary or metastatic)
Pleural involvement (primary or metastatic)
Hilar or mediastinal metastases
Rib metastases
B. Dyspnea Due Indirectly to Cancer
General debility
Fatigue
Respiratory muscle weakness
C. Dyspnea Due to Cancer Treatment
Lung included in the radiation field
D. Dyspnea Unrelated to Cancer
History of smoking
Chronic obstructive pulmonary disease
Asthma
History of exposure to: asbestos, coal dust, cotton dust, and grain dust
Anxiety
Depression
Poor sleep
In another study of 171 consecutive outpatients with lung cancer, psychological distress, the presence of organic causes, cough, and pain were significantly correlated with total dyspnea as measured by the Cancer Dyspnea Scale (30). In this study, heart rate significantly correlated with the “sense of effort” subscale, and psychological distress and pain significantly correlated with the “sense of anxiety” factor.
Anxiety is significantly correlated with the intensity of dyspnea in a number of studies in cancer patients (2,25,26,27,28,30). These correlations are significant (p = 0.03-0.001) but low (r = 0.26-0.32), with anxiety explaining only 9% of the variance in the intensity of dyspnea. Tanaka et al. also found significant correlations with the intensity of dyspnea and depression scores as measured by the Hospital Anxiety and Depression Scale (HADS) (30). When they combined the HADS anxiety and depression scores the correlation coefficient was r = 0.63 (p < 0.01), explaining 36% of variance in the intensity of dyspnea. Reddy et al. found HADS depression, but not anxiety, to be significantly correlated in univariate and multivariate analyses with the Oxygen Cost Diagram, an instrument that evaluates the effect of shortness of breath on the person’s activities of daily living (2).
PATHOPHYSIOLOGY
The pathophysiologic mechanisms of dyspnea can be categorized as increased ventilatory demand, impaired mechanical responses, or a combination of these two mechanisms. Spirometry and other pulmonary function tests (PFTs) are useful in determining the underlying etiology of dyspnea. Table 29.2 outlines the pathophysiologic mechanisms of dyspnea with the potential clinical causes in a person with cancer.
Increased Ventilatory Demand
The brainstem respiratory neural network will activate the respiratory motor drive and ventilation if there is an increase in physiologic dead space in the lung, hypoxia from any cause, severe deconditioning with early and accelerated rise in blood lactate levels, changes in VCO2 or arterial PCO2 set points, and psychological causes such as anxiety and depression. Increased physiologic dead space can occur as a result of thromboemboli, tumor emboli, vascular obstruction, or chemo- or radiation acute or chronic pneumonitis.
When dyspnea is secondary to an increased ventilatory demand spirometry is usually normal.
Impaired Mechanical Responses
Impaired mechanical responses result in restrictive or obstructive ventilatory deficits or a combination of both.
Restrictive Ventilatory Deficit
A restrictive ventilatory deficit results from decreased distensibility of the lung parenchyma, pleura, or chest wall; from reduced movement of the diaphragm; or from a reduction in the maximum force exerted by the respiratory muscles. The principal diagnostic features of a restrictive ventilatory deficit are a concurrent reduction in both FEV1 and vital capacity (FVC), decreased total lung capacity (TLC) and residual volume (RV), and often decreased diffusing capacity as well.
Obstructive Ventilatory Deficit
An obstructive ventilatory deficit refers to impedance to the flow of air within the lung. Progressive narrowing of the airways can result from structural changes from external compression or obstruction within the lumen of the airway by tumor, mucus, inflammation, or edema. Bronchoconstriction, a functional change which causes narrowing of the airways, results from increased bronchomotor tone from the release of histamine, leukotrienes, and other mediators. The hallmarks of an obstructive ventilatory deficit are a reduced FEV1/FVC and an increased TLC, RV, and functional residual capacity.
TABLE 29.2 Pathophysiologic and clinical mechanisms of dyspnea in the cancer patient
A. Impaired Mechanical Response
(a) Restrictive ventilatory deficit
(i) Pleural or parenchymal disease
Primary or metastatic
Pleural effusion
Reduced movement of diaphragm
Ascites
Hepatomegaly
Reduced chest wall compliance
Pain
Hilar/mediastinal involvement
Chest wall invasion with tumor
Deconditioning
Neuromuscular
Neurohumoral
Respiratory muscle weakness
Phrenic nerve paralysis
Cachexia
Electrolyte abnormalities
Steroid use
Deconditioning
Obstructive ventilatory deficit
Tumor obstruction
Asthma
COPD
Mixed Obstructive/Restrictive Disease (any combination of factors)
B. Increased Ventilatory Demand
Increased physiologic dead space
Thromboemboli
Tumor emboli
Vascular obstruction
Radiation pneumonitis
Chemotherapy-induced pneumonitis
Severe deconditioning
Hypoxemia—Anemia
Change in VCO2 or arterial PCO2 set point
Increased neural reflex activity
Psychological causes
– Anxiety
– Depression
COPD, chronic obstructive pulmonary disease.
Modified from Booth S, Dudgeon D. Dyspnea in advanced disease: a guide to clinical management. New York, NY: Oxford University Press, 2006.
MULTIDIMENSIONAL ASSESSMENT OF DYSPNEA
As dyspnea is a complex subjective experience a comprehensive assessment requires a qualitative appraisal, clinical assessment, and measurement of the different factors that impact on the perception of breathlessness and the effects of shortness of breath on the individual.
Qualitative Aspects of Dyspnea
The majority of scientists studying dyspnea accept that dyspnea is not a single sensation (32). They have found that there are a variety of sensations of breathing discomfort that differ in the quality of the experience, the stimuli that evoke them, and the afferent pathways (32). In COPD patients, there are at least four different “qualities” of uncomfortable breathing sensations: air hunger, work, unsatisfied inspiration, and tightness (21). In a study of 131 patients with primary or secondary lung cancer, Wilcock et al. found that there were clusters of words that were associated with the underlying cause of breathlessness (collapse, metastases, and pleural thickening) but that the overlap in the clusters between groups was too great to be useful in differential diagnosis (33).
Others suggest that to adequately characterize dyspnea, measurement of both the sensory intensity and affective intensity or unpleasantness of dyspnea is necessary. There is growing evidence to support that there are different/separate dimensions of sensory intensity and affective intensity or unpleasantness and that the ratio of sensory intensity to affective rating varies among subjects (32). In addition, there is cognitive evaluation and an emotional response to the sensation that will be affected by the person’s life experiences and personal situation and perhaps personality (32). There is great variation in the “dyspnea” experienced by different patients with similar disease states. Lansing et al. (32) suggest that knowing whether a therapy works by decreasing intensity or reducing the affective response can help determine which patients are most likely to benefit. Better measurement/assessment could provide a more sophisticated assessment of how potential therapies work and lead to appropriate choice of treatments for individuals in whom affect is a major component of respiratory discomfort.
Clinical Assessment
Clinical assessments are usually directed to determine the underlying pathophysiology and appropriate treatments and to evaluate response to therapy.
History
As in all areas of medicine, a thorough history is central to determining the underlying etiology of a person’s breathlessness. This should include its temporal onset (acute or chronic), whether it is affected by positions, qualities, associated symptoms, precipitating and relieving events or activities, and response to medications. A past history of smoking, underlying lung or cardiac disease, concurrent medical conditions, allergy history, and details of previous medications or treatments should be elicited (34,35).
The initial approach to assessment and possible treatment is greatly affected by whether the breathlessness is an acute, subacute, or chronic problem (36). The differential diagnosis of acute shortness of breath is relatively narrow: pneumonia, pulmonary embolism, congestive heart failure, or myocardial infarction. This knowledge should guide further questioning, the physical examination and possible investigations. In the setting of advanced disease, it is important to determine if the breathlessness is related to the underlying disease and potentially irreversible or whether it is completely unrelated and potentially curable.
Only gold members can continue reading. Log In or Register to continue