Chapter 6 CULTURAL ISSUES
INTRODUCTION
An older person’s cultural background has a great influence on many aspects of their mental health. When considering treatment options, it is imperative to consider a person’s cultural background. Australia like many other countries is culturally diverse, but its Anglo-Saxon or Western population is dominant. The culturally and linguistically diverse (CALD) section of the population is chronically underserviced and their health needs are not clearly articulated. This chapter provides an introduction to and an overview of issues important to understanding the complex relationship between cultural issues and mental healthcare. It highlights some of the cultural factors that influence seeking of mental healthcare, access to and utilisation of mental health services, and the quality of mental healthcare received by older people from CALD backgrounds.
Cultural diversity is referred to in terms of race and ethnicity. Cultural awareness is a cognitive construct that requires knowledge of major between-group differences, such as food preferences and religious practices. Cultural sensitivity lies in the affective domain and relates to a person’s attitude about themselves and others, and their openness to learn along cultural dimensions. Finally, cultural competence is a behavioural construct that encompasses the actions that are in response to cultural diversity, awareness and sensitivity. Some behaviours constituting cultural competence have been identified as workforce diversity and training, interventions addressing barriers, transcultural communication practices and adapting care based on the assessment of individual needs (Schim et al 2007).
CULTURAL DIVERSITY
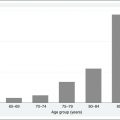
There is diversity, not often recognised, found with the original Australian peoples—the Aboriginal and Torres Strait Islanders. The tribal groups alone have up to 300 different languages (Harkins 1994). Based on the 2006 Australian census, Aboriginal and Torres Strait Islander people make up just over half a million (2.5%) of the total Australian population. The structure of the population is relatively young, with very small numbers of older people. Only 2.8% of the total Indigenous population are aged 65 years and over (approximately 16,000 people altogether) and 0.8% are aged 75 years and over. Overall, people aged 65 years and over constitute less than 3% of the Indigenous population, whereas people aged 65 years and over make up 13% of the non-Indigenous population (Australian Bureau of Statistics 2008).
The reason for this disparity is Indigenous people have a lower life expectancy based on poorer living standards due to systemic discriminatory practices since white settlement over 200 years ago. As these issues are addressed, the life expectancy of Indigenous Australians is increasing, albeit very slowly. Indigenous people mainly live in metropolitan (30%) and regional (43%) areas, with the remaining 27% residing in remote areas. In remote areas they make up 12% of the population and 45% in very remote areas. Some of these people continue to speak their traditional languages and do not have English as their second language or read English (Australian Institute of Health and Welfare 2007). The mental health status of Indigenous Australians is very poor as well. This can be attributed to chronic feelings of dislocation due to repeated losses that have occurred for many generations. These losses have been related to relocation from tribal lands, disruption of cultural practices and language, forced removal of children and the breakup of extended families, and high mortality and morbidity rates (McKendrick & Ryan 2007).
Nearly 54% of Australia’s population aged 65 years and older were born overseas, representing more than 200 different ethnic communities. About 39% of these older people are from English-speaking countries, with the vast majority (61%) from non-English-speaking countries. It is the latter that is continuing to grow faster than other segments of Australia’s population, so much so that population projections indicate that in the next 10 years one in every four people over the age of 80 will be from a CALD background (Australian Institute of Health and Welfare 2007).
CULTURAL AWARENESS
According to the statistical evidence (Australian Institute of Health and Welfare 2008), most migrants are very healthy because this is a criterion set down in government immigration policies. However, the act of migration and resettling in another country puts people under a lot of stress, because it usually means they no longer have family and friends close by for support. The value of established networks, such as health and welfare services, should not be underestimated in maintaining good mental health. The experience of ‘culture shock’ is very real and this can have detrimental effects on a person’s overall wellbeing (Minas & Silove 2007). There is a difference between people who have migrated voluntarily and those who have been forced to migrate as refugees, or asylum seekers. Many people who have arrived in Australia in the last few years have come from countries that have been devastated by political unrest and wars, and not surprisingly often have a mental health problem that can range from chronic mental health problems to trauma and distress. These extreme symptoms are particularly prominent in people who have been detained, tortured or fled persecution, and they are therefore very susceptible to mental health problems (Silove 2002).
Some ethnic groups with a long history of migration to Australia are very well established and because of their sizeable concentrations have, over the years, lobbied for and built up services that meet their specific ethnocultural needs. But the commonalities between the ethnic groups are fewer than their differences. The groups most at risk with regard to mental health are smaller ethnic groups who are very disadvantaged, not only from extreme social isolation, but also from many health, economic and political perspectives. The major issue is lack of knowledge about health services and entitlements due to poor reading and conversational ability in the English language. This issue is followed by more enduring negative influences, such as poor childhood nutritional and healthcare standards, leading to a poorer overall health status. Not having the benefit of being educated to at least the minimal education standards of a country such as Australia can mean employment is limited to intermittent, low-paid, unskilled jobs. In some cases, a person could have qualifications but they are not recognised by Australian standards. Additionally, not having complete employment means a lack of insurance and superannuation contributions that may support a person upon retirement (Minas 1990).
If health matters are viewed as a family affair with multiple family members involved with the care of the older person, then the family has a great influence on an individual’s health-seeking behaviour and pathway to formal mental healthcare treatment (O’Brien & Jackson 2007). There are likely to be highly contrasting family household structures among the various ethnic groups. While some will have living arrangements similar to what is known as the ‘nuclear family’, there remains a high propensity for living with children in multigenerational households. According to the Australian Institute of Health and Welfare (2007), family care remains an important source of support for older people from non-English-speaking backgrounds who were born overseas, with 70% living with their families compared with 58% of Australian-born older people. Additionally, they have lower usage of residential aged care facilities, but a higher use of community aged care packages.
However, it would not be prudent to assume these older people live in supported, extended families. The situation could be the exact opposite, with all the younger adults out working long hours and the older people expected to be at home caring for children. Such circumstances could create significant stresses. For example, for some older Aboriginal and Torres Strait Islander people, such an arrangement may prevent them from participating in important kinship responsibilities, such as a death ceremony which can take place over a number of weeks (McGrath & Phillips 2008). Additionally, even when an extended family network exists, caring may still be shouldered by one person, so the assumption should not be made that the need for professional care is reduced because of an ‘extended family’ living situation.
Another reason the older person may live with their family is dependency due to the inability to speak English and handle money. Some older Italian women in North Queensland, for example, although they have lived in Australia for 50 years or more, have very poor English proficiency due to living in isolated, predominantly Italian farming communities, and not being involved in outside workforce or business dealings. Such circumstances create an environment where the needs of the individual are attempted to be managed within the family and community. Seeking help outside of such protective environments is also challenging, particularly if one has faced difficulties or prejudices in the past. It is not surprising that people would hold unconventional health beliefs and practices, and look to family for decision making and care, rather than the formal service agencies, or that they would have a degree of caution in interacting with and using them (Dare 2006).
Older people in many cultures are traditionally held in high esteem and viewed as leaders and teachers. It is expected that families will care for their older members. However, despite these close family bonds, as the younger generations become assimilated to Western ways, they can become critical of older people’s traditional practices which are not seen as relevant. This diminishes the role and status of the older person. As the younger generations become involved in the work and school culture of their new country, a divergence in cultural values will invariably arise and the older person will begin to feel more lonely, isolated and alienated because they are not involved and lack understanding of many things. Additionally, if the person is an older member of a poorer, less-established, marginalised group, they may have fewer peers close to their age, thereby exacerbating the feelings of alienation and loneliness (Abrahamson et al 2002, Dare 2006, Dein & Huline-Dickens 1997).
The family dynamics in many cultures involve extremely complex processes with intricate protocols. Within Aboriginal and Torres Strait Islander families, for example, the concept of family has a collective approach in which there is much ascribed status to family members, the needs of the family outweigh the needs of the individual, mutual goals exceed individual goals and there are strong bonds of mutual obligation (O’Brien & Jackson 2007). In these circumstances, health matters become family decisions and it is important for the whole family to be involved in the decision. This is usually done with family meetings where everyone with a right and responsibility attends. Issues discussed might include the disease, current and potential symptoms, treatment options and caring issues. All the family members like to be well informed about progress and need to know what to expect (McGrath et al 2005, McGrath et al 2007).
Sometimes, a lot of consultation can take place and the family may advise the older person, but the older person is not obliged to listen to younger family members. If such a dilemma occurs, it may turn out that another approach is needed, such as the involvement of an Aboriginal health worker. This person may be more successful in having a positive impact on the healthcare issue that needs to be addressed (McGrath et al 2005, McGrath et al 2007, McGrath & Phillips 2008, O’Brien & Jackson 2007, Stein-Parbury 2009).
The stigma of mental illness permeates many cultures, causing feelings of shame and embarrassment for all involved. Stigma can be so powerful in some cultures that it can ruin a family’s public image and respect within the community. Not only is the whole family marginalised because they are seen as having ‘bad breeding’, but the individual is also subjected to fear, rejection and ridicule (Cloutterbuck & Zhan 2005, Minas 1990). The effect of these negative attitudes and beliefs on the individual can range from denial of the mental health problem and expression of psychological distress through the body rather than in the mind, lack of disclosure of problems to family members and healthcare professionals, serious delay in seeking help, and irreparable damage to family relationships and consequently support (Cloutterbuck & Zhan 2005, Dare 2006, Minas 1990). Stigma is a strong barrier in the utilisation of mental health services to the extent that, in some Asian families, the acceptance of formal support services can be seen as moral failure (Minas 1990).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


